This study summarizes the evaluation of the first and only universal BBV testing program in a German ED setting.
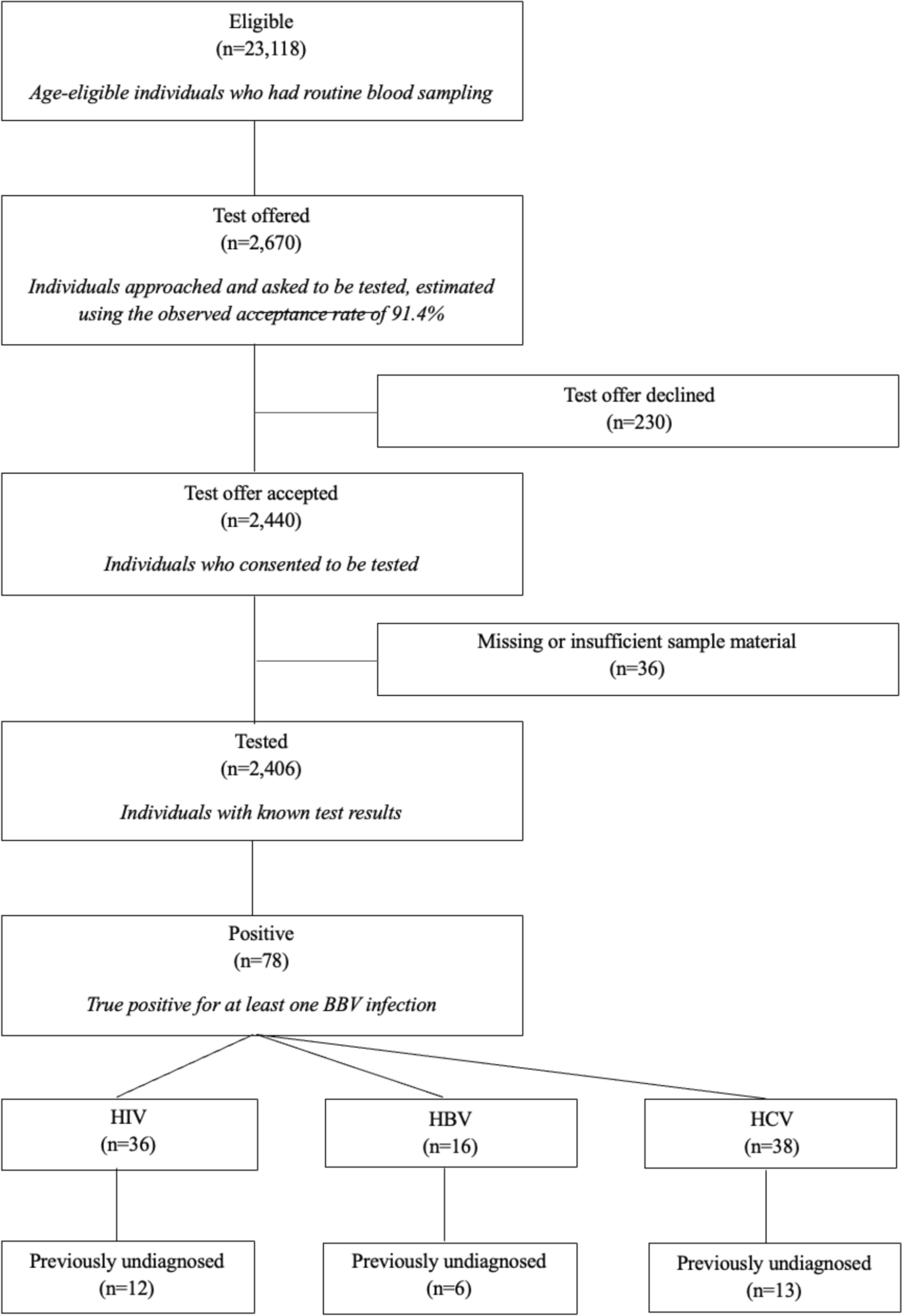
Offering testing for all three BBV infections (HIV, HBV, and HCV) was a deliberate strategy to reduce the stigma associated with HIV-only testing and to increase acceptance. This approach proved effective: our combined testing strategy achieved higher acceptance rates than those reported in previous studies that focused solely on HIV testing in emergency departments, where acceptance typically ranged from 80 to 90% [19,20,21] or lower [22, 23]. This finding suggests that combined BBV-testing may enhance patient acceptance rates and destigmatize the testing process. Furthermore, the identification of concurrent infections in 12 of 78 patients with at least one positive test result (15.4%) highlights the public health value of comprehensive BBV screening programs.
Another key element of our implementation model was the integration of testing into routine blood sample collection, minimizing additional staff burden and patient inconvenience. This seems to be an important prerequisite, according to a CDC report from 2021, which showed that, despite the revised recommendations of 2006, less than 1% of patients were tested in primary care settings in the US in recent years [24]. A likely reason may be the setting itself as EDs are specifically characterized by high workloads, high patient turnover, and staff shortages. The integration of tests into existing workflows without significant disruption to emergency care, the integration with existing laboratory infrastructure and the development of streamlined protocols for consent procedures and result notification seem therefore to be important considerations [25,26,27].
Our findings confirm that testing in EDs in urban areas can effectively identify individuals with previously undiagnosed HIV infections. The diagnostic yield of 0.5% aligns with previous studies in the US [28] and is even higher compared to some other European settings [21, 22, 29,30,31]. It is a key finding with several important implications. First, this rate exceeds commonly accepted cost-effectiveness thresholds for HIV screening in healthcare settings, suggesting that the testing strategy is not only clinically meaningful but may also be economically justified, however, a potential economic gain still warrants further investigation. Second, the prevalence of newly diagnosed HIV infections in our study population lies well above both the overall HIV prevalence in Berlin as reported by the Robert Koch Institute (RKI) and, more notably, the estimated prevalence of undiagnosed HIV infections. While this could indicate an underestimation in surveillance data, a more plausible explanation is that emergency departments serve populations with a higher baseline prevalence and pre-test probability of HIV infection.
CD4 cell counts at diagnosis in our study were lower than we would expect from national surveillance data [12, 14] and comparable initiatives in other countries [32]. We thus must acknowledge that surveillance data is influenced by case definitions, reporting mechanisms, and population denominators which should be considered, to avoid overinterpretation.
Nevertheless, most individuals with previously undiagnosed HIV infection had not yet developed AIDS-defining conditions at the time of diagnosis. This finding suggests that, although many were diagnosed late in the course of infection, they were not diagnosed too late to benefit from timely initiation of antiretroviral therapy.
The diagnostic yield of 0.2% for new HBV and 0.5% for new HCV infections drastically exceeds surveillance-based incidence estimations for Berlin. This supports the hypothesis that inner-city emergency departments serve populations with higher BBV pretest probabilities even more. Consistent with the surveillance data [33], males where diagnosed more often with HBV and HCV respectively. Similar to the situation with HIV, linkage to care was achieved for only a few of the cases with newly diagnosed HBV and HCV infections. To prevent identified individuals from being lost to follow up after diagnosis, future testing programs need to specifically target homelessness and lack of health insurance as key determinants of unsuccessful linkage to care.
Our testing rate remained low, raising the question of why so few patients were offered a test despite repeated staff training interventions. The major barrier was likely the opt-in model, which requires informed consent. Actively seeking the patient’s consent imposes additional demands on the emergency department staff, which, due to high patient volumes or individual circumstances, may not have been met by the nurses. This argument is supported by significant temporal variations in testing volumes, ranging from near-zero to 240 tests per month, with notable peaks coinciding with staff training sessions. These findings suggest that continuous education and reminder systems are crucial for maintaining consistent screening rates. At the same time, it becomes clear that in an opt-in setting even the most intensive staff education and reminder systems will probably not result in a significant increase in testing rates above approximately 10%. The data indicate that, even during periods with the highest testing activities, a large number of opportunities for testing were missed or in other words, the testing program operated far below it’s potential, a finding that is consistent with the analysis of an opt-in screening program in London [34].
Evidence from England strengthens the premise that an opt-out approach can lead to significantly higher testing rates. In a 2011 pilot project, only 14% of eligible patients were offered testing under an opt-in approach in London emergency departments [34]. In contrast, in the same setting four years later, an opt-out strategy that included combined BBV testing resulted in 28% of patients receiving a test [35]. Overall, the implementation of an opt-out HIV screening program in emergency departments of the NHS England has been remarkably successful: More than 80 hospitals are now offering universal opt-out testing [36], thereby bringing down the rates of undiagnosed HIV infection from 5.8% to approximately 4.5% between 2019 and 2023 [37]. This approach demonstrates the effectiveness of opt-out routine testing in reaching populations that might otherwise be missed [38]. In addition, an Italian study demonstrated a significant gain in both life time and quality with opt-out screening compared to indicator-triggered opt-in screening [39], and an epidemic projection model study in the US provides further evidence for the positive effects of opt-out screening in EDs [40]. Moving from an opt-in to an opt-out strategy marks an important paradigm shift: Despite the absence of specific legal regulations governing the implementation of HIV testing, legal concerns and objections from patient organizations continue to impede the adoption of opt-out HIV testing programs in Germany. Given that HIV is now a treatable chronic condition and effective therapy enables a normal life expectancy, reconsidering the current opt-in versus opt-out paradigm could offer an opportunity to enhance early detection.
What if all eligible patients had been tested in a hypothetical opt-out setting in Berlin? It is unlikely that the rate of undiagnosed infections would have remained as strikingly high. The comparative analyses of the tested versus the untested study population with respect to age and sex suggest that testing was not offered at random. Rather, it appears that the nurses offering the tests made a selective choice, likely influenced by implicit or explicit biases. Therefore, while expanding the program to include all eligible patients that do not opt out would likely have identified a greater absolute number of individuals with BBV infections. However, the overall rate of new diagnoses per test would probably have been lower in a truly universal screening program. A randomized trial in U.S. emergency departments demonstrated this elegantly: although targeted screening yielded a nearly 60% higher proportion of previously undiagnosed HCV infections than universal screening, the absolute number of new HCV diagnoses was greater in the universally screened population [41]. In this context, it remains uncertain whether, under such a hypothetical opt-out model, the rate of newly diagnosed infections per test would have exceeded the cost-effectiveness threshold for each individual BBV. Nonetheless, it is important to note that estimate-driven modelling suggests cost-effectiveness for an opt-out testing strategy in high-prevalence areas in Germany. An opt-out strategy was further estimated to improve linkage to care for individuals with both previously known and newly diagnosed infection [42].
The 50.0% rate of successful linkage to care in individuals with previously undiagnosed HIV infection demonstrates the importance of an efficient referral system. The linkage-to-care rates in this project were lower than those reported in other emergency department-based testing programs [9, 21, 28, 30], which may be attributable to differences in access to the health care system between countries. Our findings suggest that lacking health insurance coverage and being homeless are significant barriers to effective linkage to BBV treatment. This reflects a structural shortcoming of the German healthcare system in addressing the needs of marginalized populations. The problem is most pronounced in the context of HCV (15.4% linkage to care rate), however it sadly confirms the findings of the HCV screening program in US EDs [40]. It is followed by HBV (33.3%) and HIV (50.0%). From a public health perspective, the effectiveness of a costly BBV testing strategy is substantially reduced if not integrated into a systems-based approach that guarantees timely and effective linkage to care for individuals diagnosed. Addressing this critical gap may represent an important future role for non-governmental organizations (NGOs) and community-based actors.
The cost-effectiveness implications of our findings merit consideration. While a detailed economic analysis was beyond this study's scope, previous research suggests that universal HIV screening is cost-effective in settings with prevalence rates of previously undiagnosed HIV infections of > 0.1% [43]. Given Berlin's HIV prevalence of 0.4% [13] and our diagnostic yield, our findings support the economic viability of universal screening in this setting [16]. The finding that a high proportion of individuals with previously undiagnosed HIV infections were diagnosed with low CD4 cell counts, yet still without AIDS-defining conditions highlights the potential for substantial healthcare cost savings through earlier intervention and prevention of complications. Moreover, timely diagnosis and initiation of antiretroviral therapy contribute to reduced HIV transmission rates via treatment as prevention, reinforcing the public health value of early detection.
This initiative is timely as Germany falls short of the UNAIDS 95-95-95 targets. While treatment and viral suppression goals have been met, the diagnosis target remains unmet. Our findings highlight the potential of ED-based universal screening to help close this gap—particularly in high-prevalence urban areas—provided systemic barriers related to social factors and health insurance access are addressed.
This study has several limitations. Its single-center design may limit generalizability, particularly to settings with different prevalence rates, different populations and a different philosophy to access to health insurance. Berlin has a comparatively large population of individuals without access to health insurance coverage, driven by factors such as lack of legal residency status, homelessness, and substance use—challenges typical of major urban centers in Germany and elsewhere. These barriers might be less relevant in countries with a more liberal access to health care. Testing was not offered systematically, and implicit staff bias may have influenced who was approached. Selection bias in this context likely means that individuals with a higher pre-test probability were preferentially tested. This, in turn, limits the generalizability of the findings to a universal screening context, as a certain proportion of non-random test offerings must be assumed. As a retrospective analysis of a pilot program, data collection was not standardized, and misclassification cannot be ruled out. Key information, including linkage to care, was manually retrieved and may be incomplete or inconsistent. Caution is particularly warranted when interpreting linkage-to-care rates, as we only recorded initial connections, not long-term retention. Interpretation here is also limited by a substantial proportion of missing data in linkage-to-care outcomes, which cannot be assumed to be missing at random and may introduce bias. The low approach rate remains unexplained and warrants further qualitative investigation.






Comments (0)