
Remember me
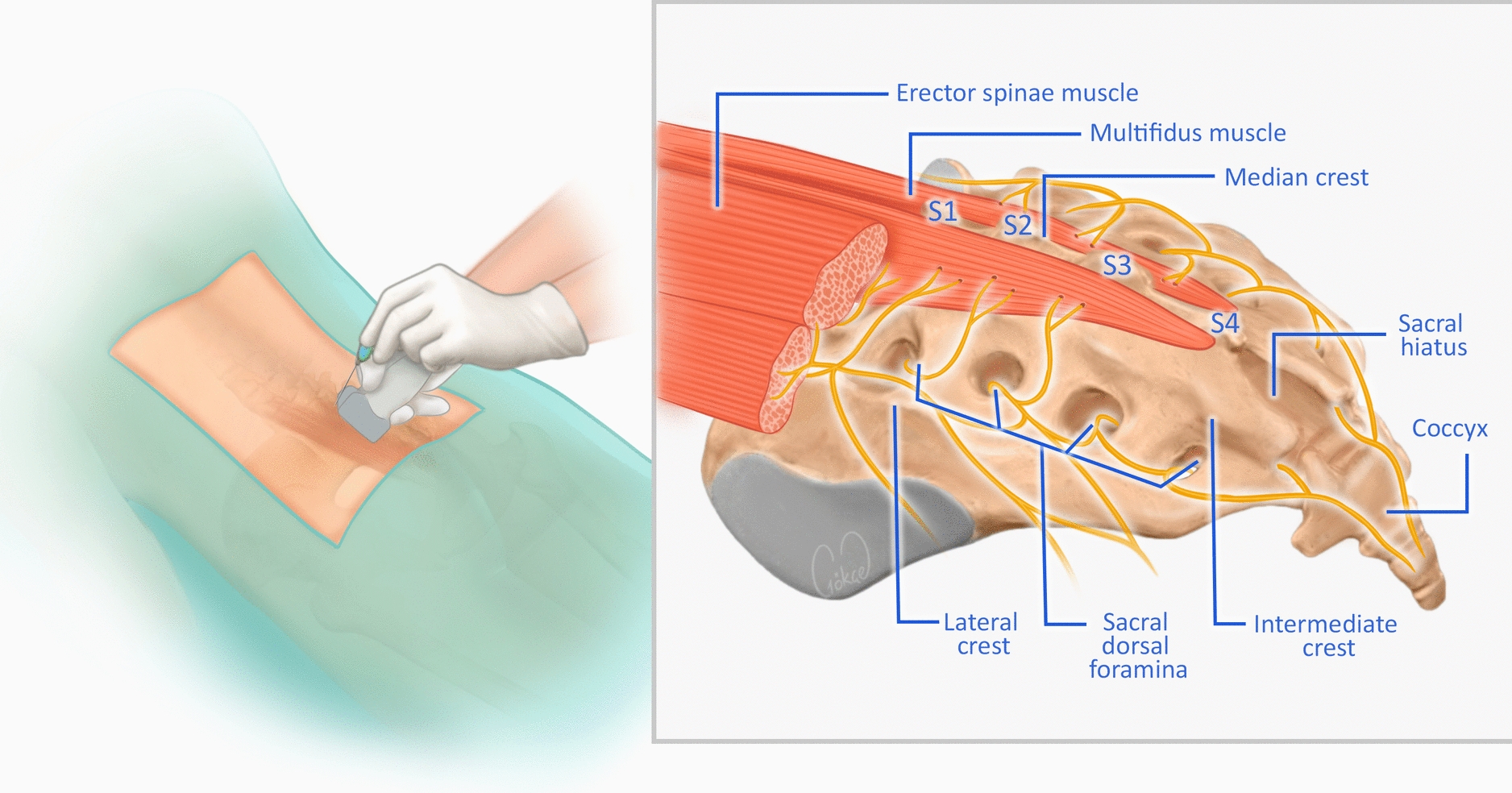
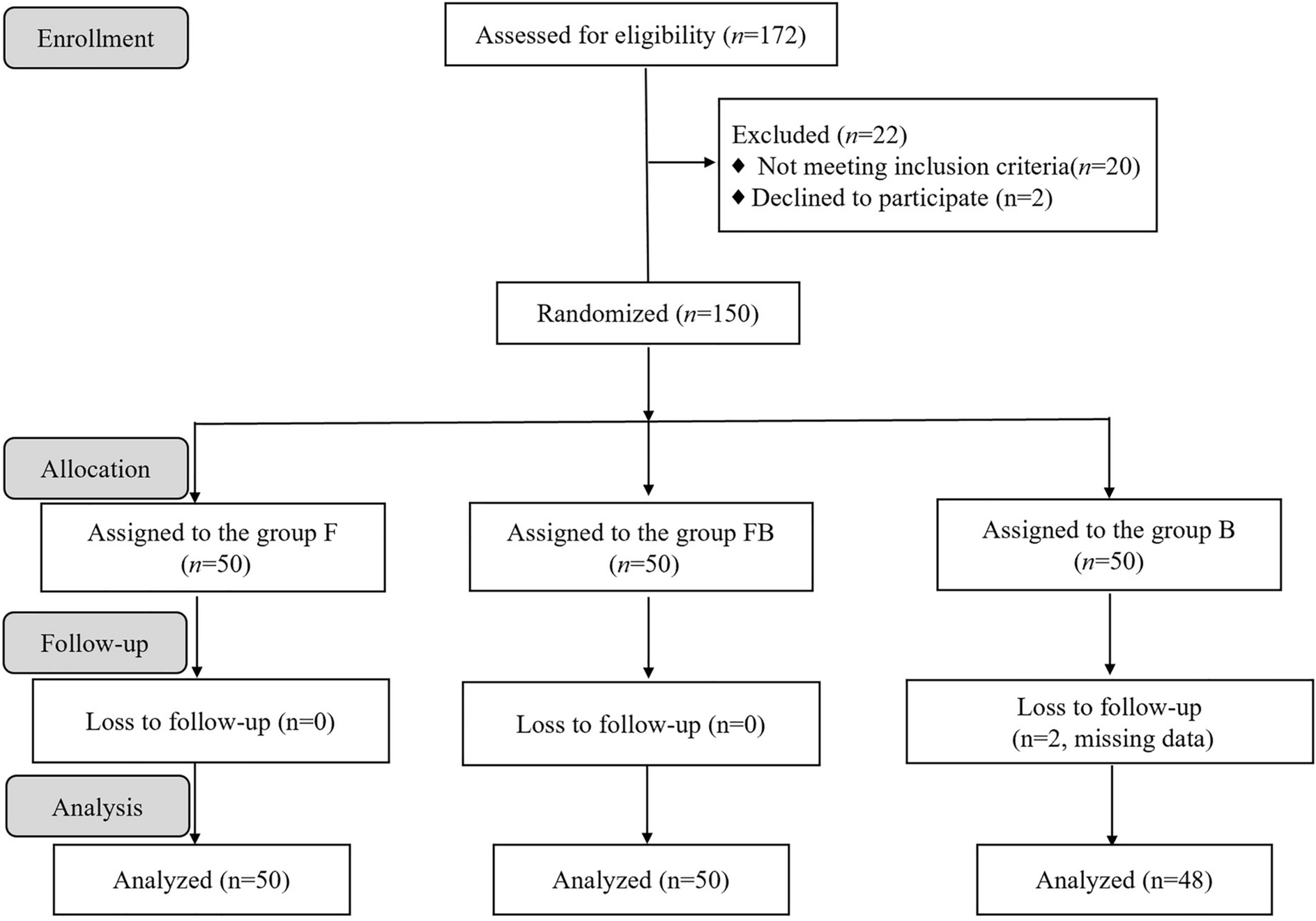






Figure 1 illustrates the schematic design of the study. The cadaver study was approved by the Ethics Committee of Shenzhen University Health Science Center (approval no: 202202021). The prospective, double-blind, randomized, and controlled study was approved by the Ethics Committee of Guangzhou Hospital of Integrated Traditional and Western Medicine (approval no: 20240424062) and registered at ChiCTR (ChiCTR2500098200). All procedures in the study adhered to the Helsinki declaration.
Fig. 1
Schematic illustration of the study design. Cadaver study was performed to evaluate the high-density nerve areas and develope strategies for electrode placement in these areas. Furthermore, a randomized and double-blinded trial was then carried out to evaluate the different TENS electrode placement in treating knee osteoarthritis (OA)
The Cadaver StudyIdentifying High-Density Nerve Areas Around the KneeAt first, a systematic anatomical dissection was conducted on 20 specimens to examine the course, distribution, and density of the cutaneous nerves around the knee (Supplementary Fig. 1). Subsequently, following the method described by T. Peker et al. [13], the high-density nerve area was identified based on the number of cutaneous nerve branches. Electrodes were placed on the high-density nerve area, and their horizontal and vertical distances from the key anatomic landmarks (patella, medial joint line, and patellar ligament) were measured (Fig. 2). To mitigate the individual heterogeneity, the patellar width was also measured, and the ratios of the horizontal and vertical distances to the patellar width were calculated.
Fig. 2
High-density nerve areas the knee. A, B There are four high-density nerve areas at the quadriceps tendon, patellar ligament, medial joint line area, and superior medial region, respectively. C The red rectangle represents the high-density nerve area at the quadriceps tendon; D The vertical distance between the base of the patella and the inferior margin of the electrode covering the high-density nerve area at quadriceps tendon was defined as A; E. The horizontal distance between the medial margin of the patella and the medial margin of the electrode covering the high-density nerve area at quadriceps tendon was defined as B; F The red rectangle represents the high-density nerve area at the patellar ligament; G The vertical distance between the inferior pole of the patella and the superior border of electrode covering the high-density nerve area at the patellar ligament was defined as C. H The horizontal distance between the medial border of the patellar ligament and the medial edge of the electrode was defined as D. I The red rectangle represents the high-density nerve area at the superior medial area; J The vertical distance between the medial joint line and the inferior margin of the electrode covering the high-density nerve area at superior medial region is defined as E; K The horizontal distance between the medial margin of the patella and the lateral border of the electrode is defined as F; L The red rectangle represents the high-density nerve area at the medial joint line area; M. The vertical distance from the medial joint line to the superior border of the electrode at the medial joint line area is defined as G; N. The horizontal distance between the medial margin of the patella and the lateral border of the electrode is defined as H. MFCNs medial femoral cutaneous nerves, IFCNs intermediate femoral cutaneous nerves, IPBSNs infrapatellar branch of saphenous nerves
Preclinical Verification of Electrode PlacementOn the basis of the findings from the section “Identifying High-Density Nerve Areas Around The Knee”, strategies for electrode placement in high-density nerve areas were developed. First, patellar width was measured. Then, electrode was positioned at specific vertical and horizontal distances proportional to patellar width, a method termed “patella-informed electrode placement.”
To verify the accuracy of this approach, preclinical verification was performed on two specimens. First, the electrodes were placed according to the patella-informed method. Then, pins were inserted around the electrodes to mark their locations (Fig. 3A, B). Finally, cutaneous nerve branches were dissected to confirm whether the electrodes were correctly positioned in the high-density nerve areas.
Fig. 3
Preclinical verification of patella-informed electrode placement. A Patellar width was first measured; B Simulated electrodes were placed according to the patella-informed electrode placement and pins were used to mark their locations around the electrodes. C The cutaneous nerve branches were dissected to verify whether the electrodes were positioned at the high-density nerve areas. C1–C4. The amplification of C
The Clinical StudyTrial Design and PatientsThe clinical study was designed as a prospective, double-blind (patient and assessor), randomized, and controlled trial (Fig. 4). Patients with knee OA were eligible if they met the American Rheumatism Association criteria [14] and the following standards: (1) aged between 50 and 75 years; (2) radiographic evidence of Kellgren-Lawrence grade 2 or 3 knee OA; (3) a score of at least 20% on one or more pain dimensions of Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index; and (4) treated at a single institution.
Fig. 4
CONSORT flow diagram. The whole flow diagram included enrollment, allocation, follow-up, and analysis. CONSORT: Consolidated Standards of Reporting Trials. VAS Visual Analog Scale, WOMAC Western Ontario and McMaster Universities Osteoarthritis Index
The exclusion criteria were as follows: patients had a history of epilepsy, knee joint trauma or diabetic neuropathy; diagnosed with lower extremity neuropathy; had electrical implants (e.g., defibrillators, deep brain stimulator, or pacemakers); took oral NSAIDs in the past 2 weeks; received TENS treatment on the target knee in the past 4 weeks; had infectious or inflammatory skin diseases in the target knee area; were pregnant or planning to become pregnant during the trial period, and had active liver, kidney, cardiovascular, or cerebrovascular diseases.
RandomizationThe sample size was calculated with NCSS-PASS (V23.0.2), assuming a standard deviation [SD] of 1.78 (on a 0–10 visual analog scale (VAS)) on the basis of previous studies [15, 16]. To achieve 80% power at a 0.05 significance level, while accounting for a 10% predicted dropout rate, 40 patients per group were required. Randomization was conducted on an individual basis with consecutively numbered sealed envelopes (1–80), which were opened after patient recruitment. After obtaining informed consent, patients were assigned as follows: odd-numbered patients were allocated to the patella-informed electrode placement (electrode on high-density nerve area, study cohort); even-numbered patients were assigned to the traditional electrode placement group (electrode in pain area, control cohort). In total, 80 patients were enrolled in the study, with 40 in the study cohort and 40 in the control cohort.
TENS InterventionsAccording to the patient allocation, electrodes were placed on the high-density nerve areas for patients in the study cohort. In contrast, for the control cohort, electrodes were positioned directly in the pain areas (Fig. 5A, B). The physiotherapist set the TENS stimulation parameters and intensity using XY-K-SJD-A TENS device (Sunnyou Co., Ltd., China). TENS modality was individualized using standard recommended stimulation parameters (low-frequency, high-frequency, or burst TENS) and biphasic pulse waveform, according to symptom presentation. The frequency was initially set from 60 to 100 Hz and the pulse duration was gradually increased from 100 µsec to 250 µsec. TENS treatment sections were conducted five times per week, with each session lasting up to 30 min.
Fig. 5
Electrode placements in the clinical trial. A In the study cohort, electrodes were placed on the high-density nerve areas. B In the control cohort, electrodes were placed directly in the pain areas
Outcome MeasurementClinical outcomes were evaluated by an assessor who was blind to the patient allocation. WOMAC and VAS indexes, the most widely used assessment for knee OA pain, were used as the assessment tools. The WOMAC index and VAS index questionnaires were collected at baseline and at one week and two weeks post the first TENS intervention. The WOMAC index includes 5 pain-related questions, 2 stiffness-related questions, and 17 questions on difficulty in daily activities. Each subscale is graded on a 5-point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = extreme).
Adverse events were defined as any new or worsening signs, symptoms, or undesirable occurrences during the study. Referring to the report by Reichenbach et al.[17], adverse events include local skin reactions. Serious adverse events were classified as those resulting in hospitalization, prolonged hospitalization, significant or persistent disability, life-threatening events, or death.
Statistical AnalysisStatistical analysis was performed with IBM SPSS Statistics 20.0 (Armonk, New York, USA) and GraphPad Prism 8 (GraphPad Software Inc.). Categorical variables were presented as numbers and percentages and continuous variables as median values. Friedman test was used for the comparison of repeated non-parametric measurements, the Wilcoxon signed-rank test for the paired comparison. Differences at a P level of < 0.05 were identified as statistically significant.
Comments (0)