Study population
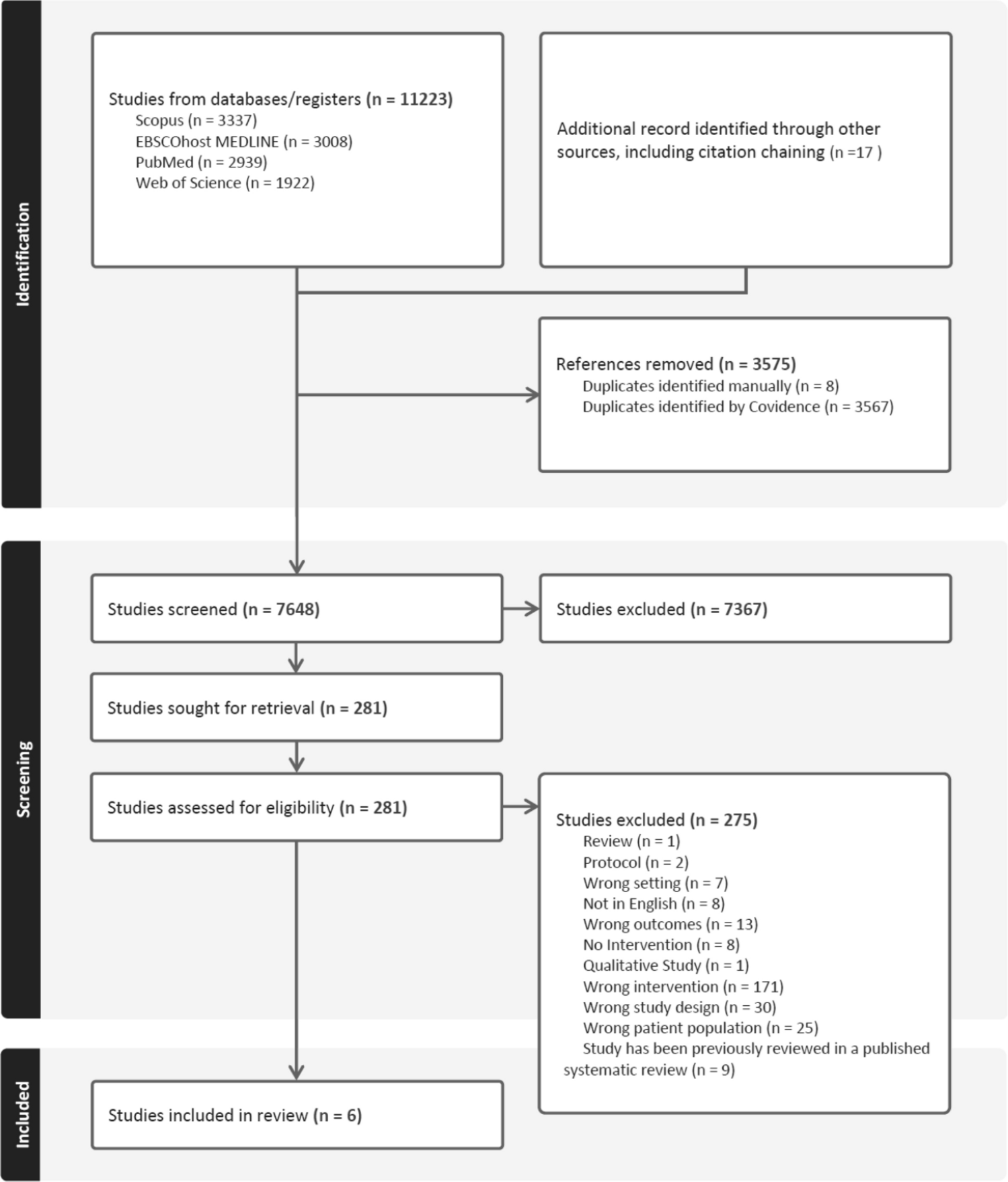
We included baseline pre-randomization data from three randomized, double-blinded, placebo-controlled clinical trials (RCTs) conducted at the University of Southern California (USC) Atherosclerosis Research Unit that enrolled healthy, cognitively intact male and female adult participants between 2000 and 2006 [B-Vitamin Atherosclerosis Intervention Trial (BVAIT; ClinicalTrials.gov identifier NCT00114400) (Hodis et al. 2009b), Women’s Isoflavone Soy Health Trial (WISH; NCT00118846) (Henderson et al. 2012), and Early Versus Late Intervention Trial with Estradiol (ELITE; NCT00114517) (Hodis et al. 2015)]. The primary outcome for the three RCTs was reduction in progression of early atherosclerosis, and all RCTs included assessment of depressive symptoms (see below). Briefly, postmenopausal women without clinical evidence of CVD or cognitive impairment were eligible for WISH and ELITE and otherwise healthy men and postmenopausal women with fasting plasma homocysteine levels ≥ 8.5 µmol/L were eligible for BVAIT. Recruitment occurred from Los Angeles County, covering a geographic area of approximately 64,000 km2. A total of 8538 individuals were screened across the three trials via telephone or in person; 5367 did not meet eligibility criteria. Reasons for exclusion included clinical signs or symptoms of CVD, diabetes mellitus or fasting serum glucose ≥ 126 mg/dL, triglyceride (TG) levels ≥ 500 mg/dL, hypertension [systolic blood pressure (SBP) ≥ 160 mmHg and/or diastolic blood pressure (DBP) ≥ 100 mmHg)], untreated thyroid disease, creatinine clearance < 70 ml/min or serum creatinine > 2.0 mg/dL, a life threatening disease with prognosis < 5 years, alcohol intake > 5 drinks per day/substance abuse, unwillingness to stop taking B-vitamin supplements (BVAIT), current use of hormone therapy (WISH or ELITE), hysterectomy and no oophorectomy (ELITE), or 6–9 years postmenopausal (ELITE). Of the 1509 subjects who were randomized, 13 did not have data on air pollution exposure (n = 9) or depression symptoms (n = 4) leaving 1496 (99.1%) participants included in this study.
All human research was approved by the USC Institutional Review Board (WISH Approval#: HS-035001; BVAIT Approval#: HS-98B012; ELITE Approval#: HS-04A024), and all participants provided written informed consent.
MeasurementsAssessment of air pollution exposure
Air pollution exposure assignments were derived from measured ambient air quality data spatially mapped to participants’ geocoded residence addresses using a geographic information system (GIS). These data were initially automatically geocoded to TigerLine files (Navteq, 2006), then manually resolved in a multi-step process similar to that described by McElroy (McElroy et al. 2003). Ambient air quality data were primarily extracted from the Air Quality System (AQS), maintained by the US Environmental Protection Agency (http://www.epa.gov/ttn/airs/airsaqs/). A database of O3 [8-h maximum, in parts per billion (ppb)], NO2 (24 h, in ppb) and PM2.5 (24 h, in µg/m3) concentrations at monitoring stations was compiled from a June 2008 AQS version. Measurements obtained using Federal Reference Methods and Federal Equivalent Methods were included and supplemented with monthly average O3, NO2, and PM2.5 concentrations measured in the Southern California Children’s Health Study (Peters et al. 2004). Daily, monthly, and annual average concentrations were calculated using a 75% data completeness criterion. The database included measurements from California and border areas of nearby states for calendar years 2000–2006. The density of measurement stations in this regional air monitoring network was every 20–40 km in urban areas and 50 to 150 km in rural areas (ARB 2008).
Annual daily average concentrations of air pollutants from monitoring stations during 2000–2006 were spatially interpolated to participants’ residential addresses using inverse-distance-squared weighting. Specifically, if one or more stations with valid data for a specific year were located within 5 km of a residence, the air pollutant assignment was based solely on local data. If there were no stations within 5 km, air pollutant assignments were calculated from the three closest stations with valid data located within 100 km of the residence. Historical address data were not available for participants for years prior to their enrollment in the RCTs. To derive measures of long-term residential exposure to O3, NO2, and PM2.5, we averaged estimated air pollution exposure at the residential address where the participant lived at enrollment in the RCT and at that address for the prior year. Air pollution exposure was scaled to 10 parts per billion (ppb) for O3 and NO2, and to 10 ug/m3 for PM2.5.
Depressive symptoms
The Center for Epidemiological Studies-Depression scale (CES-D) (Radloff 1977) is a 20-item measure of current depressive symptomatology. The CES-D queries the frequency of symptoms such as restless sleep, poor appetite, and feeling lonely over the previous week. Response options range from 0 to 3 for each item (0 = Rarely or None of the Time, 1 = Some or Little of the Time, 2 = Moderately or Much of the time, 3 = Most or Almost All the Time). Total CES-D scores range from 0 to 60, with higher scores indicating greater risk for depression. We used the CES-D assessment obtained at the baseline visit for each participant. Participants were also categorized in two groups using a score of ≥ 16 following commonly recommended practices to identify individuals with suspected prevalent clinical depression (Lewinsohn et al. 1997; Vilagut et al. 2016; Weissman et al. 1977).
Antidepressant medications
Information on current medication use was self-reported by participants on questionnaires prior to trial randomization and administration of the CES-D. All records were reviewed by one research assistant (MR) for reports of drugs used to treat the symptoms of clinical depression as defined by Anatomical Therapeutic Chemical (WHO 1993) classification code N06A including non-selective monoamine reuptake inhibitors, selective serotonin reuptake inhibitors, non-selective monoamine oxidase inhibitors, monoamine oxidase A inhibitors, and other antidepressants. We considered participants to have antidepressant medication use if they reported one or more of the medications from the listed classes.
Sociodemographic and covariate data
All participants completed a questionnaire regarding sociodemographic factors, smoking status, and a 7-day physical activity recall that elicited number of hours spent in different activities including sleep. Each reported physical activity was converted to metabolic equivalents (METs) and MET-hours (METs times duration of activity); a summary variable accumulated MET-hours over all reported activities. Physical exam measures included blood pressure, body height and weight; body mass index (BMI) was calculated (weight in kg/height in m2). Blood samples were drawn after a minimum 8-h fasting period. Total cholesterol, high-density lipoprotein cholesterol (HDL- cholesterol) and low-density lipoprotein cholesterol (LDL- cholesterol, calculated) were measured by standardized enzymatic assay methodology (Lipid Clinics Research Program, 1974). Fasting serum glucose levels were measured using the glucose oxidase technique on a Beckman Glucose II analyzer (Beckman Instruments, Brea, CA, USA).
Carotid artery intima-media thickness (CIMT) is a measure of subclinical atherosclerosis and an independent predictor of cardiovascular risk (Bauer et al. 2012). The right common carotid artery was imaged using high resolution B-mode ultrasound with simultaneously recorded single-lead electrocardiogram for cardiac gating (Hodis et al. 2001, 2009a, 2011). For the primary trial outcome, CIMT was measured at the distal common carotid artery far wall during minimum lumen diameter (approximate diastole) with in-house developed automated computerized edge detection software (patents 2005, 2006, 2011) (Hodis et al. 2001; Selzer et al. 2001). CIMT was determined as the average of approximately 70–100 individual measurements between the intima–lumen and media–adventitia interfaces along a 1-cm length just proximal to the carotid artery bulb. This method standardizes the location, distance, and timing over which CIMT is measured and ensures that the same portion of arterial wall is measured in each image and compared within and across all participants. The coefficient of variation for repeated baseline CIMT measurements is < 1% (Hodis et al. 2009b). Using the mean for the study population, we classified participants as having average and higher (≥ 0.77 mm) or lower than average (< 0.77 mm) CIMT levels.
Statistical analysis
We examined two outcomes in regression models (1) total CES-D score as a measure of prevalent depressive symptoms, and (2) suspected prevalent clinical depression indicated by a CES-D score ≥ 16. Linear regression methods with continuous scaled terms for individual air pollution measures were used to estimate cross-sectional associations with total CES-D score. Because CES-D scores were positively skewed in the study population, we applied a log transformation of the total CES-D score in the linear models and back transformed results for interpretation. We used robust Poisson regression models (Barros and Hirakata 2003; Zou 2004) to estimate cross-sectional associations with air pollution exposures and suspected prevalent clinical depression (yes, no).
Model covariables were selected a priori based on findings from previous studies (Kioumourtzoglou et al. 2017; Pun et al. 2017; Qiu et al. 2023; Wang et al. 2014b). Simple models were adjusted for sociodemographic characteristics including age (continuous), race/ethnicity (Asian, Pacific Islander, Native American; Black; Hispanic/Latino; non-Hispanic White), sex, educational level (high school or less, some college, Bachelor’s degree, graduate/professional degree), household income (< 30,000, 30,000–49,999, 50,000–69,999, 70,000–99,999 and ≥ 100,000 US dollars/year), and indicator variables for year and study (BVAIT, WISH, ELITE). Multivariable models were adjusted for covariables from simple models plus BMI (< 25, 25–29.9, ≥ 30 kg/m2), smoking status [ever (former/current), never], physical activity (total MET-hours), fasting glucose, systolic blood pressure, LDL-cholesterol, HDL-cholesterol and anti-depressant medication use (yes, no).
We tested interaction terms individually for O3, NO2, and PM2.5 by sex and CIMT level (continuous) in multivariable models using a threshold of p-value < 0.05 for effect modification. We used the categorized CIMT variable (< 0.77 mm, ≥ 0.77 mm) in stratified models to estimate air pollution-depression associations by CIMT level. Because air pollutants share common sources, we conducted two-pollutant multivariable models for O3 and NO2, or O3 and PM2.5 in order to explore the joint effects and contributions of individual pollutants in combination with one other pollutant on symptoms of depression. Because NO2 and PM2.5 exposures were highly correlated in our study population (Supplemental Table 2), we did not estimate a joint effects model for these two pollutants. In sensitivity analyses, we expanded the grouping of participants with suspected prevalent clinical depression to include those using medications prescribed for depression or having a total CES-D score ≥ 16. In additional sensitivity analyses, we included an indicator variable for annual unemployment rate for Los Angeles County to examine the effect of controlling for a macro-level economic factor in the multivariable models of CES-D total score. The annual unemployment rate for Los Angeles County between 2000 and 2006 was categorized as low (≤ 5.3%), average (5.4–5.8%) or high (≥ 5.9%) unemployment. We report beta coefficients (β) with 95% confidence intervals (CI) from linear regression models, and risk ratios (RRs) with 95% CIs from Poisson regression models per 10 units of the air pollutants.
All analyses used SAS version 9.4 (SAS Institute Inc., Cary, NC, USA.).





Comments (0)