
Remember me




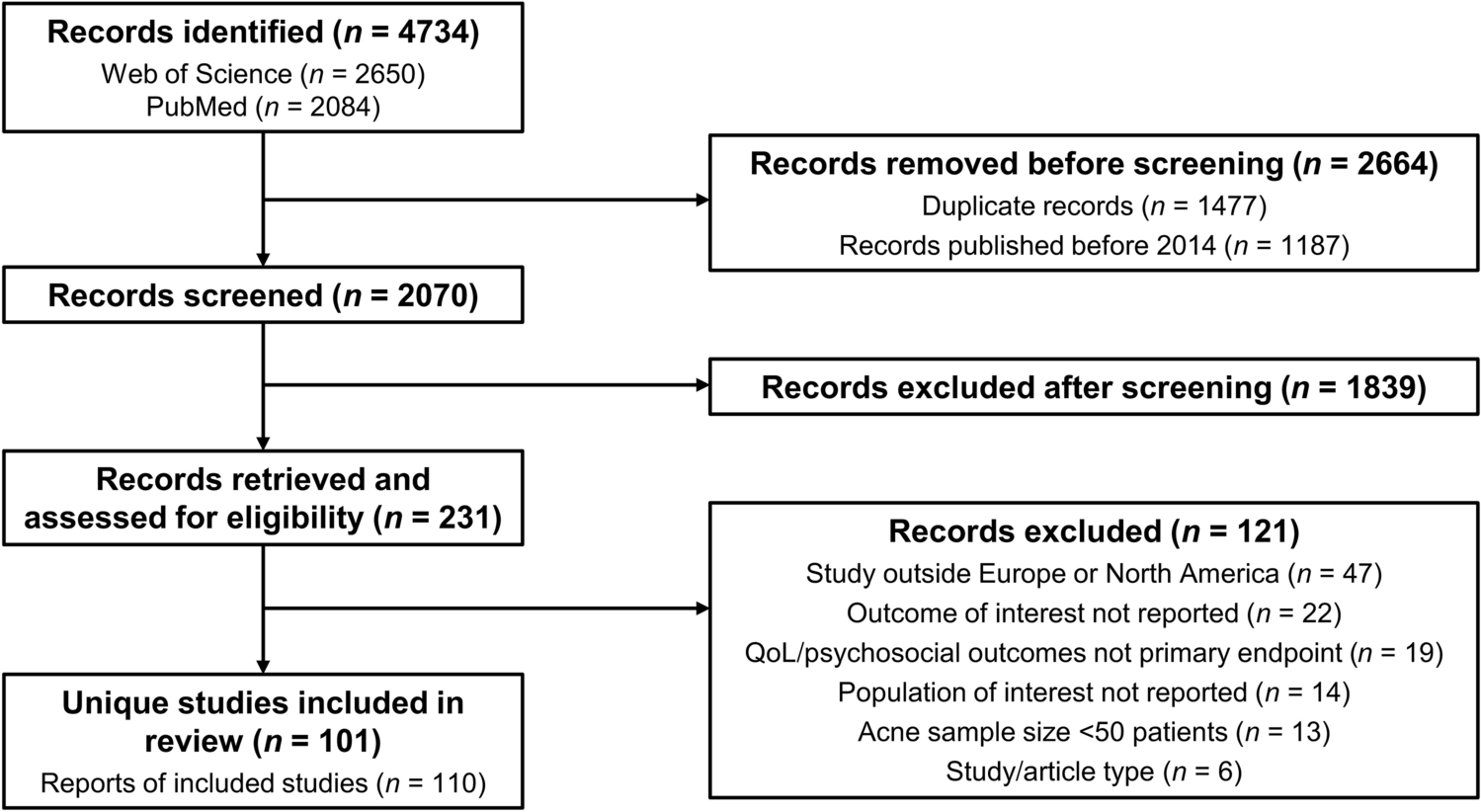
A total of 2594 studies were identified across three databases. After removing duplicates, 1657 studies remained for title and abstract screening. Of these, 514 studies were selected for full-text review. Ultimately, 40 studies met inclusion criteria. The PRISMA flow diagram illustrating the selection process is presented in Fig. 1. Summaries of the included studies evaluating the associations of menopause and MHT with common dermatoses are presented in Tables 2 and 3, respectively.
Fig. 1
PRISMA flow chart illustrating the study selection process. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Table 2 Studies examining the impact of menopause on common dermatosesTable 3 Studies examining the impact of menopausal hormone therapy on common dermatoses3.2 Menopause, Menopausal Hormone Therapy, and Common Dermatoses3.2.1 AlopeciaAmong the dermatoses analyzed, alopecia emerged as the most studied condition. A strong association was identified between menopause and various forms of alopecia, particularly frontal fibrosing alopecia (FFA) and female pattern hair loss (FPHL). Multiple studies reported that the onset of FFA predominantly occurred after menopause, with postmenopausal women accounting for 84–100% of cases [11,12,13,14]. Notably, early menopause was also frequently linked to FFA. In a case-control study, Buendía-Castaño et al. found the average age of menopause among women with FFA to be 47.7 years, lower than 49.7 years in age-matched controls [15]. Similarly, Vañó-Galván et al. reported that 14% of patients with FFA experienced early menopause, compared to 6% in the general population [16]. Hysterectomy and/or oophorectomy were also associated with FFA, with reported incidences ranging from 3.7 to 13% among affected individuals [14, 17].
In the context of FPHL, both advancing age and the number of years since menopause were associated with increased incidence and severity of symptoms. Özkoca et al. found that menopause was linked to more advanced stages of the condition, although it did not correlate with any particular clinical subtype [18]. Similarly, Venning and Dawber and Chaikittisilpa et al. observed a higher prevalence of pattern hair loss with increasing age, especially after the onset of menopause [19, 20]. Ali and Wojnarowska also reported a clear upward trend in overall hair loss with age among a cohort of postmenopausal females [21]. In contrast, the relationship between age and frontal hair loss was less pronounced, and no association was observed with temporal hair loss [21].
The relationship between MHT and alopecia is complex and remains poorly defined due to limited and sometimes conflicting evidence. Importantly, different types of alopecia appear to respond differently to hormonal influences. In a multicenter case-control study of 335 females with FFA, Moreno-Arrones et al. found a significant association between FFA and various hormonal exposures, including pregnancy, HRT, and raloxifene, with HRT specifically linked to increased odds of FFA (odds ratio [OR] = 1.76, 95% confidence interval [CI] 1.11–2.8) [22]. More recently, a large retrospective study by Singal et al. further supported these findings, showing that females exposed to HRT (OR = 3.87, 95% CI 3.31–4.52), exogenous androgens (OR = 3.72, 95% CI 2.77–5.00), and hormonal contraceptives (OR = 2.92, 95% CI 2.65–3.22) had significantly higher odds of developing lichen planopilaris (LPP) or FFA compared to female controls [23].
In contrast, Endo et al. evaluated 11 females without any hair loss complaints before and after six months of HRT and observed improvement in frontal hairline thinning and increased hair plucking strength at six months [24]. They also noted a transient increase in the telogen hair rate at three months, which normalized by the 6-month mark [24]. Another study by Georgala et al. assessed 75 postmenopausal females with androgenic alopecia (AGA) treated with topical estradiol valerate 0.03% over 12 and 24 weeks. Both treatment groups showed an improved anagen-to-telogen hair ratio compared to placebo [25]. However, two participants developed postmenopausal uterine bleeding, with endometrial findings consistent with estrogen-induced proliferation, raising concerns about the safety of unregulated topical estrogen products. With the growing popularity of over-the-counter topical estrogen formulations marketed for “anti-aging,” there is an urgent need for better long-term safety data and physician oversight in this area [26, 27].
Finally, post-marketing safety data from Estratest® and Estratest® HS (esterified estrogens with methyltestosterone), prescribed for vasomotor symptoms from 1989 to 2002, documented alopecia as an adverse event in 8.8% of reported cases (n = 225) [28, 29]. Although some evidence suggests estrogen may improve hair loss, these findings underscore the potential for hormone-induced alopecia in certain conditions or with specific hormone formulations. Clinically, this highlights the importance of counseling patients that while estrogen therapy may benefit some types of alopecia, research is limited, and androgenic formulations can paradoxically worsen hair loss.
Summary: The evidence demonstrates a robust association between menopause and alopecia, with the overwhelming majority of FFA cases occurring postmenopausally and affected women experiencing menopause earlier than controls. Similarly, FPHL severity correlates with menopausal status, with advancing age and increasing years since menopause associated with more advanced disease stages and greater overall hair loss. The association between MHT and alopecia remains complex and inconsistent, with outcomes varying according to study design, hormone formulation, route of administration, and the specific alopecia subtype examined.
3.2.2 PsoriasisFour studies investigated the relationship between menopause and psoriasis. In a prospective cohort study of postmenopausal women using UK Biobank data, Xiao et al. found that later age at natural menopause (ANM) and longer reproductive years were significantly associated with decreased risks of late-onset psoriasis and psoriatic arthritis [30]. Specifically, ANM after 55 years was inversely associated with the risk of late-onset psoriasis (34% reduction) and psoriatic arthritis (46% reduction) compared with ANM before 45 years (p < 0.001). The protective effect of later menopause on psoriasis risk exceeded that of established risk factors, including smoking and obesity [30]. Reciprocally, in a large population-based cohort of 1.7 million reproductive-age women, psoriasis was associated with an increased relative risk (RR) of early menopause (<45 years; RR 2.21, 95% CI 2.02–2.42, p < 0.01) and premature ovarian failure (<40 years; RR 2.35, 95% CI 2.03–2.72, p < 0.01) [31]. Xhaja et al. found that 36% of females with psoriasis reported a worsening of their condition due to hormonal changes, including menopause (p < 0.05) [32]. Similarly, Mowad et al. observed that 48% of females experienced exacerbation of psoriasis symptoms during menopause (p = 0.001), while 50% noted no change and only 2% reported improvement. The study found no meaningful differences between natural and surgical menopause [33]. In a large prospective cohort of 163,763 women from the Nurses’ Health Study I and II, Wu et al. observed a modestly increased risk of psoriasis with surgical menopause compared to natural menopause (hazard ratio [HR] = 1.19, 95% CI 1.01–1.40), although this association did not remain significant after correction for multiple testing [34]. Additionally, in contrast to Xiao et al. [30], Wu et al. [34] found no statistically significant association between age at menopause and psoriasis risk.
Four studies investigated the relationship between psoriasis and MHT. In a large population- based study of 1,130,741 postmenopausal females Gang Min Go et al. reported that MHT at all time points (<2 years, 2–5 years, and >5 years) increases risk of psoriasis compared to no MHT (HR = 1.13, 1.21, 1.22, respectively; 95% CI 1.09–1.17, 1.15–1.26, and 1.16–1.29, respectively) [35]. In contrast, Chan et al. demonstrated that postmenopausal females with an intact uterus using conjugated estrogen with medroxyprogesterone acetate (MPA) (n = 11,734) had a decreased risk of psoriasis (HR = 0.77, 95% CI 0.60–0.98, p = 0.04), whereas there was not a significant difference in the conjugated estrogen alone group (females with prior hysterectomy, n = 7577) [36]. Mowad et al. reported that among 63 females with psoriasis during menopause, the majority noted no improvement in their symptoms with MHT use [31]. Lastly, Wu et al. reported that current MHT users had a slightly increased risk of psoriasis, but these data were not statistically significant [34]. Clinically, this highlights the need for dermatologists to monitor psoriasis activity in women starting MHT, recognizing that certain formulations may exacerbate disease while others appear neutral, and to individualize management accordingly.
Importantly, psoriasis and menopause each independently increase risks for cardiovascular disease, metabolic syndrome, and mood disorders such as depression [37]. The combined burden of these overlapping risks remains underrecognized and underscores the need for coordinated prevention strategies. Additionally, we have identified no clinical trials evaluating whether long-term psoriasis therapies require dose adjustments as estrogen levels decline with menopause. In practice, treatments such as tumor necrosis factor inhibitors, interleukin-17 blockers, and methotrexate are generally maintained at the same doses, with modifications made only in response to disease activity.
Summary: Evidence on the relationship between menopause and psoriasis is mixed. Later menopause may reduce the risk of psoriasis and psoriatic arthritis, but other large cohorts show no clear association. Smaller survey studies consistently report that a substantial proportion of women perceive worsening or persistent symptoms during menopause, though objective assessment is lacking. Both conditions independently increase risks for cardiovascular disease, metabolic syndrome, and depression, yet this overlap is underrecognized and understudied. Data on MHT and psoriasis remain inconclusive.
3.2.3 AcneThree studies explored the relationship between acne and menopause. In a survey study, Perkins et al. found that postmenopausal females reported less acne than age-matched controls, with acne severity showing a negative correlation with the number of years since menopause [38]. Similarly, Collier et al. observed a decline in acne prevalence with age, affecting 26.3% of females aged 40–49 and 15.3% of those aged 50 and above [39]. Cunliffe and colleagues also noted reduced acne in females over 40, underscoring the inherent challenge of distinguishing menopausal effects from those of natural aging, which reduces sebum output associated with acne pathogenesis [40,41,42].
There is a notable lack of research examining the impact of MHT on acne development. However, adverse event data from Phillips et al., evaluating females treated with esterified estrogens combined with methyltestosterone for vasomotor symptoms between 1989 and 2002, reported acne as an adverse effect in 5.6% (n = 142) of cases [28, 29]. This finding suggests that while menopause may be associated with a decreased risk of acne due to declining estrogen levels, certain MHT formulations—particularly those containing androgenic components like methyltestosterone—may reintroduce or exacerbate acne in susceptible individuals. Clinically, this highlights the importance of inquiring about MHT use, especially androgenic or testosterone-containing regimens, in postmenopausal women presenting with new-onset or worsening acne.
Although testosterone is not conventionally considered part of MHT, it is increasingly prescribed off label for the management of hypoactive sexual desire disorder (HSDD) in postmenopausal women [43]. With this rise in off-label testosterone use, dermatologists should be aware of its potential role in new-onset acne among menopausal women. Nonetheless, research directly evaluating the dermatological effects of exogenous testosterone in this population remains lacking.
Summary: Acne generally decreases after menopause due to hormonal changes and age-related declines in sebaceous activity. However, evidence on the effects of MHT is limited, with no studies evaluating conventional estrogen ± progestogen regimens. The growing off-label use of testosterone in menopause—typically through dose-adjusted male products prescribed for HSDD—may increase acne risk, but its impact in this population has not yet been studied.
3.2.4 RosaceaTwo studies examined the relationship between menopause and rosacea. In a large retrospective analysis of 5248 rosacea cases, Wu et al. found that postmenopausal females had a lower risk of developing rosacea compared to premenopausal females (HR = 0.73, 95% CI 0.58–0.92) [44]. However, a small prospective cohort study by Yang et al., involving 59 perimenopausal females with erythematotelangiectatic rosacea (ETR) identified an inverse association between estradiol levels and rosacea severity [45]. Females with moderate to severe ETR had significantly lower estradiol levels compared to those with mild disease [45]. Based on these findings, the authors proposed an “estradiol protective hypothesis,” suggesting that higher estrogen levels may enhance skin barrier function and reduce the likelihood of cutaneous disease, potentially lowering the risk of rosacea. However, this hypothesis is challenged by Wu et al.'s significantly larger trial, which showed a decreased incidence of rosacea in the postmenopausal period—which is characterized by reduced estrogen levels. Wu et al. also reported that MHT use among postmenopausal females was associated with an increased risk of rosacea (HR = 1.32, 95% CI 1.08–1.61) compared to non-users, with a non-significant trend toward higher risk with longer use (p = 0.26). Although, it is notable that Wu et al.’s cohort consisted of only White females, which limits its generalizability [45]. Clinically, this highlights the importance of recognizing MHT as a potential contributing factor in new or worsening rosacea.
Summary: Menopause appears to lower the risk of rosacea, as large cohort data show postmenopausal women have reduced incidence compared to premenopausal women. Notably, MHT use has been associated with increased rosacea risk, highlighting exogenous hormones as a potential modifiable factor. Dermatologists should consider both menopausal status and MHT exposure when evaluating new or worsening rosacea in midlife women.
3.2.5 MelasmaHigh-estrogen states such as pregnancy are well-established risk factors for the development of melasma [46]. Estrogen is believed to stimulate melanocyte activity, increasing melanin production—particularly when combined with ultraviolet (UV) exposure [46, 47]. Oral contraceptive pills (OCPs) containing both estrogen and progestin have also been linked to the onset and worsening of melasma [46]. As a result, discontinuation of hormonal contraceptives can be recommended as part of melasma management, with patients experiencing improvement over time.
Given this hormonal link, it would be reasonable to hypothesize that the menopausal period—characterized by a significant decline in estrogen and progesterone levels—might lead to an improvement in melasma. However, a case-control study by Handel et al. found no significant association between menopause and melasma [48]. In a large cross-sectional multicenter study in Brazil, Hexsel et al. reported varying effects of menopause on melasma, including improvement (29.4%), worsening (38%), and no change (30.1%) [49]. Interestingly, they noted a higher proportion of extra-facial melasma in postmenopausal females (14.2%) versus non-menopausal females (3.5%) (p < 0.0001).
This finding was echoed by Ritter et al., whose case-control study found that extra-facial melasma appeared to be associated with menopause, a family history of melasma, and a personal history of facial involvement. Notably, the study found no significant difference in hormone therapy use between melasma and non-melasma groups [50]. Finally, Mpofana et. al noted that melasma had less of a negative impact on quality of life after menopause as compared with prior to menopause [51]. Although these data found no clear overall association between menopause and melasma, two studies reported a higher prevalence of extra-facial melasma in postmenopausal females. Clinically, this highlights the importance of counseling that while high-estrogen states clearly drive melasma, the effects of menopause and MHT remain uncertain, and management should continue to focus on photoprotection and standard therapies.
Summary: While high-estrogen states such as pregnancy and oral contraceptives are recognized triggers for melasma, findings regarding menopause are inconsistent. Most studies do not demonstrate a definitive association, although some suggest greater extra-facial involvement in postmenopausal women. Evidence on MHT remains scarce, with no clear indication of its impact on melasma risk or severity.
3.2.6 Hidradenitis SuppurativaThree studies examined the impact of menopause on HS, revealing variable and at times contradictory findings. Fernandez et al. reported that in most patients, HS symptoms either worsened or remained unchanged during menopause [52]. Notably, the study found a statistically significant inverse relationship between the severity of HS symptoms during menstruation and after the onset of menopause, suggesting that hormonal fluctuations may play a key role in symptom expression. Similarly, Barth et al. observed that HS symptoms persisted into menopause and afterward among a small cohort, further supporting the idea that menopause does not alleviate disease activity [53]. In contrast, Kromann et al. conducted a survey-based study in which 48% of participants reported an improvement in HS symptoms following menopause, while 38% experienced no change and 15% noted worsening, indicating a more favorable response in some individuals [54].
Emerging evidence points to the potential influence of hormonal therapies on HS outcomes. Studies have shown that combined oral contraceptives containing both estrogen and progesterone may delay the onset or reduce the severity of HS [5, 55]. These findings carry important implications for the use of MHT, suggesting that the hormonal environment may be modifiable in ways that benefit disease control. However, research examining the impact of MHT on the presentation and severity of HS is conspicuously lacking. More research is needed to clarify the role of estrogen and progesterone in HS pathogenesis, and to determine whether MHT could be a viable therapeutic adjunct in postmenopausal females with HS.
Critically, both HS and menopause are independently associated with increased metabolic risk. Women with HS have higher rates of metabolic syndrome and diabetes compared with controls, while the menopausal transition is linked to central adiposity, worsening insulin sensitivity, and elevated cardiovascular risk [56, 57]. Despite these overlapping burdens, no studies have specifically examined how menopause modifies metabolic comorbidities in HS, mirroring gaps seen in psoriasis research. Addressing this intersection is critical for improving long-term outcomes in affected women. Clinically, this highlights the importance of recognizing that while OCPs may influence HS premenopausally, there are no data to guide MHT use after menopause, and management should therefore prioritize guideline-based dermatological therapies while coordinating care for comorbid risks.
Summary: Findings on the impact of menopause on HS are inconsistent, with studies reporting persistence, worsening or improvement of symptoms. Hormonal therapies such as combined oral contraceptives may benefit disease control, but the role of MHT remains unstudied. Both HS and menopause independently increase metabolic risks, yet their combined impact has not been evaluated. Dermatologists should be aware of these overlapping burdens and coordinate care with other specialties to optimize outcomes.
3.2.7 Prevalence of DermatosesThe literature on the prevalence of dermatoses in menopausal females remains limited, with only a handful of studies providing direct insight. The most comprehensive data come from Aboobacker et al., a large retrospective study involving over 8000 perimenopausal females, which identified eczematous disorders as the most common dermatoses (23.6%), followed by urticaria (12.4%) and papulosquamous disorders (10.7%) [58]. These findings are echoed by two smaller studies in postmenopausal females—Wai (n = 84) and Pariath and Nair (n = 150)—which also reported eczema as one of the most frequently observed conditions. Pariath and Nair found that genital dermatoses were present in 60% of participants, with atrophic vaginitis being the most prevalent (33.33%), followed by lichen sclerosus et atrophicus and lichen simplex chronicus (each at 15.55%) [59, 60]. Melasma was comparatively uncommon, reported in just 1.1–8.3% of females across the three studies. Additionally, among those with hair disorders in Pariath and Nair’s cohort, FPHL accounted for 34.24% [52]. In a more recent cohort, Jha and Selvaraj observed xerosis in 78% and pruritus in 46% of 150 postmenopausal women, supporting the view that dryness and itch are among the most frequently encountered findings in menopause [61]. Notably, 92% exhibited at least one dermatological manifestation ,with pigmentary changes reported in 64%, and hair thinning in 58%. All studies were conducted in India, limiting generalizability to other populations.
Summary: Evidence on dermatoses in menopause is limited to Indian cohorts. Eczema, genital dermatoses, and hair loss were common. Xerosis and pruritus were also highly prevalent, making dryness and itch leading complaints.
Comments (0)