
Remember me



Control of haemorrhage is one of the cornerstones of emergency interventional radiology. With ongoing technical improvements in catheter/microcatheter equipment and embolic agents such as coils, vascular plugs and liquids, the means to perform emergency embolisation procedures has never been more available. As the success of embolisation procedures for haemorrhage increases, the demands for the IR service increase both in and out of hours.
Gastrointestinal haemorrhage—In upper gastrointestinal (GI) haemorrhage, IR embolisation plays a key role in treating patients who fail medical and endoscopic intervention. For patients with refractory oesophageal or gastric variceal bleeding, IRs may offer life-saving therapy by performing a transjugular intrahepatic portosystemic shunt (TIPSS). For lower GI haemorrhage, recent guidance from the British Society of Gastroenterology has favoured the use of IR embolisation over surgical intervention in unstable patients with evidence of active bleeding on CT Angiography (1).
Traumatic haemorrhage—The development of major trauma centres (MTCs) for the severely injured trauma patient has led to centralisation of services. NHS guidance indicates that MTCs should have timely access to an interventional radiology consultant who can treat traumatic haemorrhage due to visceral injury (spleen/kidney/liver/etc.) and pelvic trauma by embolisation. Interventional radiologists are also important for the treatment of peripheral vascular injury by embolisation and stent-grafting, and the management of aortic injury by abdominal or thoracic aortic endografts.
Haemoptysis—Bronchial artery embolisation is an important interventional radiological treatment for patients with massive haemoptysis. Recent guidelines produced by CIRSE indicate that following multi-detector CT to identify anatomy, bronchial artery embolisation can be performed by interventional radiologists with sufficient expertise with high technical success rates of > 90% (2).
Obstetric haemorrhage—Obstetric haemorrhage remains one of the major causes of maternal death after delivery. Interventional radiologists are essential in any hospital with a maternity unit as they can perform rapid and emergent embolisation of pelvic arterial branches for post-partum haemorrhage and save maternal lives. Interventional radiologists also play a key role in the management of patients with placental anomalies. For these patients who have been identified as being at high risk prior to delivery, obstetricians may decide in consultation with their IR colleagues for the IRs to place compliant occlusion balloons in both internal iliac arteries before delivery. These can be inflated where required during and immediately following delivery to minimise haemorrhage. If haemorrhage occurs post-balloon deflation, emergent uterine artery embolisation can be performed by the interventional radiologist.
Peripheral Vascular DiseaseOne of the fundamental areas of treatment for interventional radiologists is peripheral vascular disease (PVD), which is one of the most common health issues affecting the UK population. It is estimated that PVD affects approximately 20% of people over the age of 60 (3). Interventional radiology methods for treating peripheral arterial occlusive disease include angioplasty and/or stenting using plain or drug-eluting/coated devices as well as more advanced methods such as atherectomy and intravascular lithotripsy. Compared to surgery, endovascular treatment is cost-effective, often serves as a first line method of treatment, and provides similar results to surgery in patients who lack a suitable venous conduit for bypass (4).
Interventional radiologists also play a key role in the management of patients with acute limb ischaemia using intra-arterial transcatheter thrombolysis and/or percutaneous thrombectomy. These procedures utilise a variety of dedicated devices from straightforward aspiration thrombectomy to mechanical thrombectomy.
Aortic DiseaseInterventional radiologists play an important role in the management of aortic aneurysms, aortic dissection, and aortic trauma. This may involve the insertion of standard or complex aortic endografts, often as a team in collaboration with vascular surgical colleagues. Interventional radiologists also play a key role in the management of complications of aortic endografting such as the embolisation of endoleaks.
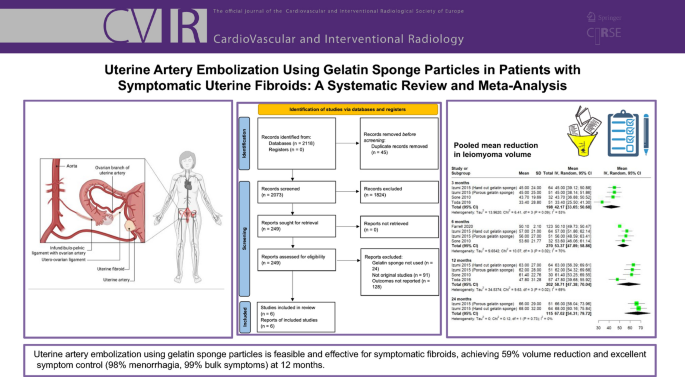
Uterine FibroidsUterine fibroids are the most common type of tumour in women of reproductive age (5). The quality of life of approximately half of these women is adversely affected by significant symptoms (6). These women can be treated with uterine artery embolisation (UAE) by interventional radiologists. Uterine artery embolisation provides a much less invasive alternative to surgery and is often the only option for women who wish to preserve their uterus. There is no significant difference in long-term results between UAE and surgical treatment. Therefore, every female patient who requires treatment for uterine fibroids should be offered UAE if appropriate (7).
Venous Thromboembolic DiseaseInterventional radiologists are essential in the management of patients with venous disease. One of the key roles of IRs in venous disease is in the management of acute and chronic venous occlusive disease.
Venous thromboembolic disease poses a major impact to the healthcare economy not just in terms of mortality but also morbidity. The development of a post-thrombotic limb after ilio-femoral deep vein thrombosis may lead to major and lifelong consequences of chronic venous insufficiency for a group of patients who are often young. More severe cases may present acutely with a threatened limb which requires prompt treatment (8).
Catheter directed thrombolysis may benefit patients with acute ilio-femoral deep vein thrombosis. More recent advances in mechanical thrombectomy technologies have led to an increase in efficiency of thrombus clearance (9). The evidence indicates that young patients with ilio-femoral deep vein thrombosis and low bleeding risk would benefit from thrombus clearance—a position that has been adopted in many national guidelines around the world.
Deep venous stenting is helpful in certain specific situations, both in the acute and the chronic situation. The advent of dedicated venous stent technologies has improved outcomes. Interventional radiologists may use intravascular ultrasound to assist with stent sizing and deployment.
Inferior vena cava (IVC) filters are indicated in specific circumstances to reduce the risk of pulmonary emboli—e.g. when a patient with a deep vein thrombosis cannot be treated by anticoagulant therapy. Once deployed, scheduled removal of the filter should be undertaken at an agreed time interval at a later date. The evidence for pulmonary embolism reduction after IVC filter insertion has been well established for more than 20 years. Recent trends in management have focussed on correct patient selection for filter placement, protocols for removal and adequate follow up arrangements.
The emerging field of pulmonary embolism thrombectomy / catheter directed thrombolysis has led to some potentially promising results but as yet remains limited to certain centres.
Vascular AccessInterventional radiologists perform various vascular access procedures, especially for long-term venous access in both adult and paediatric patients. The most common venous access procedures are peripherally inserted central catheters, tunnelled central venous catheters and tunneled central venous ports. Potential uses of these devices include haemodialysis, chemotherapy, plasmapheresis, parenteral nutrition and long-term antibiotic treatment. With cancer therapy identified as one of the clinical priorities in the NHS long-term plan and a general increase in difficult vascular access patients, interventional radiology services to provide venous access are imperative to assist in improving patient outcomes.
Dialysis Access Insertion and MaintenanceAs of 2020, there were approximately 25,532 adults and 100 children on long term haemodialysis, and more patients are being added every year (10). The scope of interventional radiology includes performing access procedures for dialysis, such as placing tunneled and non-tunneled dialysis lines, creating percutaneous endovascular arteriovenous fistulas, and maintaining surgically created fistulas.
Percutaneous fistuloplasty and stent insertions, and percutaneous thrombectomy procedures are just some of the interventional radiology techniques that are performed to maintain the patency of a malfunctioning dialysis fistula.
Urological ObstructionAn obstructed kidney is a core urgent referral to all IR departments, with an infected obstructed kidney being a medical emergency. Although there is selective evidence that the routes of decompression, i.e. urological retrograde stenting versus radiological percutaneous nephrostomy (PCN) are equivalent (11), a PCN is quicker and has a higher success rate (12), especially with distal obstruction or significant ureteral stone disease. The facility to perform PCN must be available at all times (24/7) to all acute hospitals either onsite or at a neighbouring hospital through a prearranged formal agreement via a network arrangement.
Unless severe urosepsis is present at the time of nephrostomy, a ureteric stent should be inserted at the same time as drainage of the pelvicalyceal system.
Percutaneous nephrostomy is also required in non-obstructed scenarios when trying to divert urine away from the renal pelvis if there is a renal or ureteric leak or a ureteric fistula.
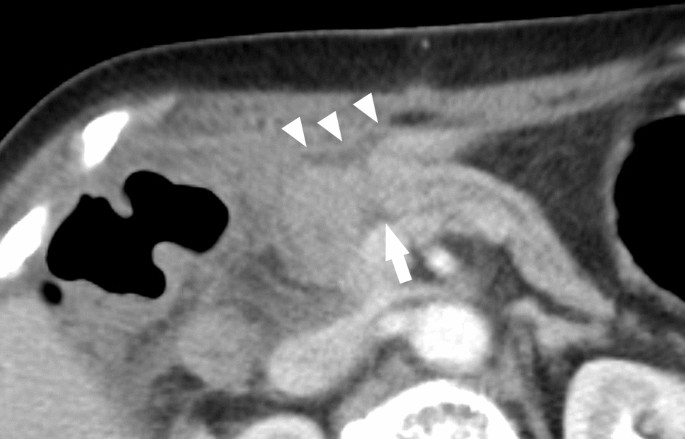
Biliary ObstructionPercutaneous biliary drainage and stenting may provide prompt drainage of an obstructed biliary tract. Relief of bile duct obstruction is required urgently if there is a suspicion of biliary sepsis in the presence of bile duct obstruction.
Although percutaneous biliary drainage (PBD) with a metallic or plastic stent has a higher technical success rate, endoscopic retrograde cholangiopancreatography (ERCP) has become the first line management of biliary obstruction outside of the liver transplant population (13). As a result, the number of PBDs performed has fallen over the last two or three decades and is today reserved for failed ERCP or for complications after liver transplantation. The provision of PBD should ideally only be performed by high volume upper GI centres or hepatobiliary centres with prearranged referral agreements from neighbouring units. The requirement of emergency out of hours PTC is rare.
Nutrition and Feeding TubesPatients who are not able to eat or drink either because of neurological disorders or obstructing lesions of the oesophagus can receive nutrition via a variety of feeding tubes that can be inserted by interventional radiologists.
These vary from per-oral or per-nasal tubes, e.g. nasogastric and nasojejunal tubes to percutaneous gastrostomy and gastrojejunostomy tubes. Interventional radiologists play a major role in assisting nutrition for many patients with severe disease that prevents them from eating and drinking via the normal route.
Cancer Treatment: Interventional OncologyInterventional radiologists have developed many techniques to treat and palliate cancer. As a result, IRs have created the specific entity of interventional oncology. Interventional oncology is increasingly regarded as the 4th pillar of cancer care alongside surgery, radiotherapy and chemotherapy. The main interventional oncology techniques are percutaneous tumour ablation and transcatheter tumour embolisation.
Tumour ablation—Since the first case reports of chemical ablation of hepatocellular carcinoma (14) and radiofrequency ablation of renal cell carcinoma (15) were published as far back as 1993, image-guided percutaneous ablation of malignant tumours has become an established, effective treatment especially in the liver, kidney, and other organs. The indication, method and choice of cytotoxic energy deposition continues to develop. The main methods of ablation are radiofrequency ablation, microwave ablation, irreversible electroporation and cryotherapy. The choice of ablation treatment is multifactorial including anatomy, comorbidity and patient and physician preference.
Tumour embolisation—Interventional radiologists play a major role in the treatment of many cancers by transarterial embolisation. The liver is the organ that is most frequently targeted for transarterial embolisation. Either primary liver tumours (hepatocellular carcinoma—HCC) or secondary liver tumours (e.g. colorectal metastases) can be treated by embolisation with or without a chemotherapeutic drug (chemoembolisation). The dual blood supply of the liver makes it an ideal target for intra-arterial embolotherapy. Standardisation of embolisation techniques and chemotherapeutic agents, and ongoing technical improvements have led to improved outcomes in patients with primary liver cancer.
Bland embolisation of hepatocellular carcinoma with particles or microspheres is still performed, although increasingly units have moved towards mixing the embolic agent with a chemotherapeutic drug such as Doxorubicin (transarterial chemoembolisation—TACE). Transarterial (chemo)embolisation is less commonly performed for secondary liver tumours although it remains an option in certain selected cases, e.g. symptomatic neuroendocrine tumour metastases.
More recently, NICE guidance has approved the use of Selective Internal Radioembolisation therapies (SIRT), typically using microspheres bound with Yttrium-90, which are injected into the arteries supplying the tumour. This treatment is available for patients with colorectal liver metastases as well as those with HCC. MDT discussion is required as well as close collaboration with nuclear medicine colleagues.
For intermediate stage HCC, survival with TACE could be expected to be greater than 2.5 years. The success of this therapy and subsequently SIRT has led to a defined clear role for these treatments within most national and international guidelines (16).
Embolisation outside the liver is less often performed for oncological control, but may be helpful in specific symptomatic situations (e.g. relief of haematuria in renal cell carcinoma -RCC) or as an adjunct to other treatments, e.g. RCC bone metastasis embolisation to reduce haemorrhage during subsequent orthopaedic fixation.
Palliation of advanced cancer—Interventional radiologists play a crucial role in improving the quality of life of patients with incurable malignancy. This can range from simple procedures (e.g. rapid transfer of patient to and from a hospice for paracentesis during end-of-life care) to more complex procedures (e.g. thermal ablation of painful skeletal metastatic disease). Each cancer unit IR department may not offer the full spectrum of interventions, but must have arrangements in place with neighbouring hospitals if there is a clinical need that they cannot meet. This can be facilitated via the regional Cancer Alliance.
The decision to not intervene in a palliative setting is an important choice for patients when quality of life is the primary outcome.
StrokeApproximately 20% of stroke survivors die within the first year and over 50% are left with long term disability. This costs the NHS and the wider economy approximately £7billion per year (17). The highest degree of disability occurs in patients with a proximal large artery occlusion (40% of strokes), who may not respond well to thrombolytic agents. Approximately 10–12% of these patients are suitable for mechanical thrombectomy. Mechanical thrombectomy for proximal intracerebral artery occlusion can prevent irreversible cerebral ischaemia and prevent or limit long term disability (18). Mechanical thrombectomy is possibly one of the most significant interventions to be developed since acute coronary intervention.
Stroke thrombectomy is undertaken using stent-retrievers, sometimes with supplemental thrombus aspiration. This technique has been shown to produce the best outcomes (19).
The procedure is performed by clinicians trained in vascular minimally invasive procedures with specific training in mechanical stroke thrombectomy. In the UK this is predominantly interventional neuroradiologists and interventional radiologists.
The GMC have provided specifications for a credential in stroke thrombectomy, which clinicians from other specialties will have to complete in order to undertake this procedure.

The DAWN and DEFUSE-3 (20, 21) studies revealed that mechanical thrombectomy was more effective than standard care alone for specific individuals with large vessel ischaemic stroke, who presented with symptoms within 24 h of onset. As a result, the current guidelines have expanded the window for thrombectomy to 24 h after the onset of symptoms.
An efficient stroke thrombectomy service requires clinicians who are trained in stroke thrombectomy. The service should ideally be funded and staffed to provide a 24-h service. The procedure should be performed in a centre with dedicated neuroradiological imaging and stroke physicians, to enable the correct patients to be selected for treatment.
References
13.1.:Diagnosis and management of acute lower gastrointestinal bleeding: guidelines from the British Society of Gastroenterology. Oakland K, et al. Gut 2019;0:1–14. https://doi.org/10.1136/gutjnl-2018-317807
13.2.:CIRSE Standards of Practice on Bronchial Artery Embolisation. Kettenbach et al. Cardiovasc Intervent Radiol. 2022; 45(6): 721–732.
13.3.:Prevalence | Background information | Peripheral arterial disease | CKS | NICE [Internet]. [cited 2023 Mar 26]. Available from: https://cks.nice.org.uk/topics/peripheral-arterial-disease/background-information/prevalence/
13.4.:Farber A, Menard MT, Conte MS, Kaufman JA, Powell RJ, Choudhry NK, et al. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N Engl J Med. 2022 Dec 22;387(25):2305–16.
13.5.:Stewart E, Cookson C, Gandolfo R, Schulze-Rath R. Epidemiology of uterine fibroids: a systematic review. BJOG Int J Obstet Gynaecol. 2017;124(10):1501–12.
13.6.:Borah BJ, Nicholson WK, Bradley L, Stewart EA. The Impact of Uterine Leiomyomas: A National Survey of Affected Women. Am J Obstet Gynecol. 2013 Oct;209(4):319.e1-319.e20.
13.7.:Daniels J, Middleton LJ, Cheed V, McKinnon W, Sirkeci F, Manyonda I, et al. Uterine artery embolization or myomectomy for women with uterine fibroids: Four-year follow-up of a randomised controlled trial. Eur J Obstet Gynecol Reprod Biol X. 2021 Nov 20;13:100139.
13.8.:NICE guideline NG158 - Venous thromboembolic diseases: diagnosis, management and thrombophilia testing
13.9.:European Society for Vascular Surgery (ESVS) 2022 Clinical Practice Guidelines on the Management of Chronic Venous Disease of the Lower Limbs – De Maessneer et al. EJVS 63;2: 184–267
13.10.:24th Annual Report - data to 31/12/2020 | The UK Kidney Association [Internet]. [cited 26]. Available from: https://ukkidney.org/audit-research/annual-report/24th-annual-report-data-31122020
13.11.:Pearle MS, Pierce HL, Miller GL, Summa JA, Mutz JM, Petty BA, Roehrborn CG, Kryger JV, Nakada SY. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998 Oct;160(4):1260–1264. PMID: 9751331.
13.12.:Mokhmalji H, Braun PM, Martinez Portillo FJ, Siegsmund M, Alken P, Köhrmann KU. Percutaneous nephrostomy versus ureteral stents for diversion of hydronephrosis caused by stones: a prospective, randomized clinical trial. J Urol. 2001 Apr;165(4):1088–92. PMID: 11257644.
13.13.:Van Eecke E, Degroote H, Vanlander A, Hindryckx P. Outcome of primary ERCP versus primary PTC for biliary drainage in malignant hilar biliary strictures: a systematic review and meta-analysis. Surg Endosc. 2022 Oct;36(10):7160–7170. https://doi.org/10.1007/s00464-022-09413-5. Epub 2022 Aug 8. PMID: 35941311.
13.14.:Castells A, Bruix J, Bru C, Fuster J, Vilana R, Navasa M, Ayuso C, Boix L, Visa J, Rodés J. Treatment of small hepatocellular carcinoma in cirrhotic patients: a cohort study comparing surgical resection and percutaneous ethanol injection. Hepatology. 1993 Nov;18(5):1121–1126. PMID: 8225217.
13.15.:Gervais DA, McGovern FJ, Wood BJ, Goldberg SN, McDougal WS, Mueller PR. Radio-frequency ablation of renal cell carcinoma: early clinical experience. Radiology. 2000 Dec;217(3):665–672. https://doi.org/10.1148/radiology.217.3.r00dc39665. PMID: 11110926.
13.16.:BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. Reig et al Journal of Hepatology 2022 vol. 76 j 681–693
13.17.:NHS England Evidence review: Mechanical thrombectomy for acute ischaemic stroke in the anterior cerebral circulation (2023 draft)
13.18.:Berkhemer OA, Fransen PS, Beumer D,et al; MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015 Jan 1;372(1):11–20. https://doi.org/10.1056/NEJMoa1411587.
13.19.:Nogueira RG, Lutsep HL, Gupta R, et al; 2012. Results from the TREVO 2 Study (Thrombectomy REvascularization of large Vessel Occlusions in acute ischemic stroke): Randomized data comparing Trevo with Merci for thrombectomy in acute stroke. Cerebrovascular Diseases, 33, 57.
13.20.:Nogueira RG, Jadhav AP, Haussen DC, et al; DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med. 2018 Jan 4;378(1):11–21. https://doi.org/10.1056/NEJMoa1706442. Epub 2017 Nov 11. PMID: 29129157.
13.21.:Albers GW, Marks MP, Kemp S, et al; DEFUSE 3 Investigators. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med. 2018 Feb 13.22;378(8):708–718. https://doi.org/10.1056/NEJMoa1713973. Epub 2018 Jan 24. PMID: 29364767; PMCID: PMC6590673.
Comments (0)