
Remember me





Adult non-trauma patients (≥ 18 years of age) who presented at the ED of the University Medical Center Groningen (UMCG) between December 4, 2023, and January 22, 2024, with a suspected infection (as determined by the treating physician upon initial contact based on focal symptoms suggestive of an infection (e.g., productive cough, dyspnea, dysuria, pollakiuria, abdominal pain, erythema) and/or fever (≥ 38 °C, either at home or upon triage at the ED) and presented for internal medicine (i.e., general medicine, immunology, oncology, vascular medicine, hematology, nephrology, infectiology), gastroenterology, urology, non-trauma emergency medicine, pulmonology, or rheumatology. Patients who were transferred to our ED from another hospital after the initiation of therapy were excluded from the study.
Data and samples were prospectively collected by Acutelines, a data, image, and biobank at the emergency department of the University Medical Center Groningen (UMCG). To allow collection of data and biomaterials when applicable, primary screening of patients for eligibility is performed upon arrival in the ED by the ED-nurse together with a trained research team. For this study, blood samples were drawn into PAXgene® Blood RNA tubes at triage, prior to treatment initiation, from patients presenting to the ED between 11:00 and 20:00 h. Patients were then examined, diagnosed, and treated according to the standard of care.
A deferred consent procedure (by proxy) is in place to allow the collection of data and biomaterials prior to obtaining written consent. If the patient or proxy could not reasonably be reached, an opt-out procedure was followed. A detailed description of the design, inclusion and exclusion criteria of Acutelines has been published previously [18].
TriVerity testThe investigational use only (IUO) TriVerity Test (Inflammatix, Sunnyvale, CA, USA), performed on the IUO Myrna Instrument (Inflammatix, Sunnyvale, CA, USA), was performed on blood samples (2.5 mL) collected in PAXgene Blood RNA tubes within one hour of collection. The tubes were gently inverted 10 times to ensure thorough mixing of the PAXgene medium with the blood promoting lysis and RNA preservation, while avoiding foam formation. Following mixing, the samples were processed using a new TriVerity test cartridge and the Myrna instrument for subsequent testing.
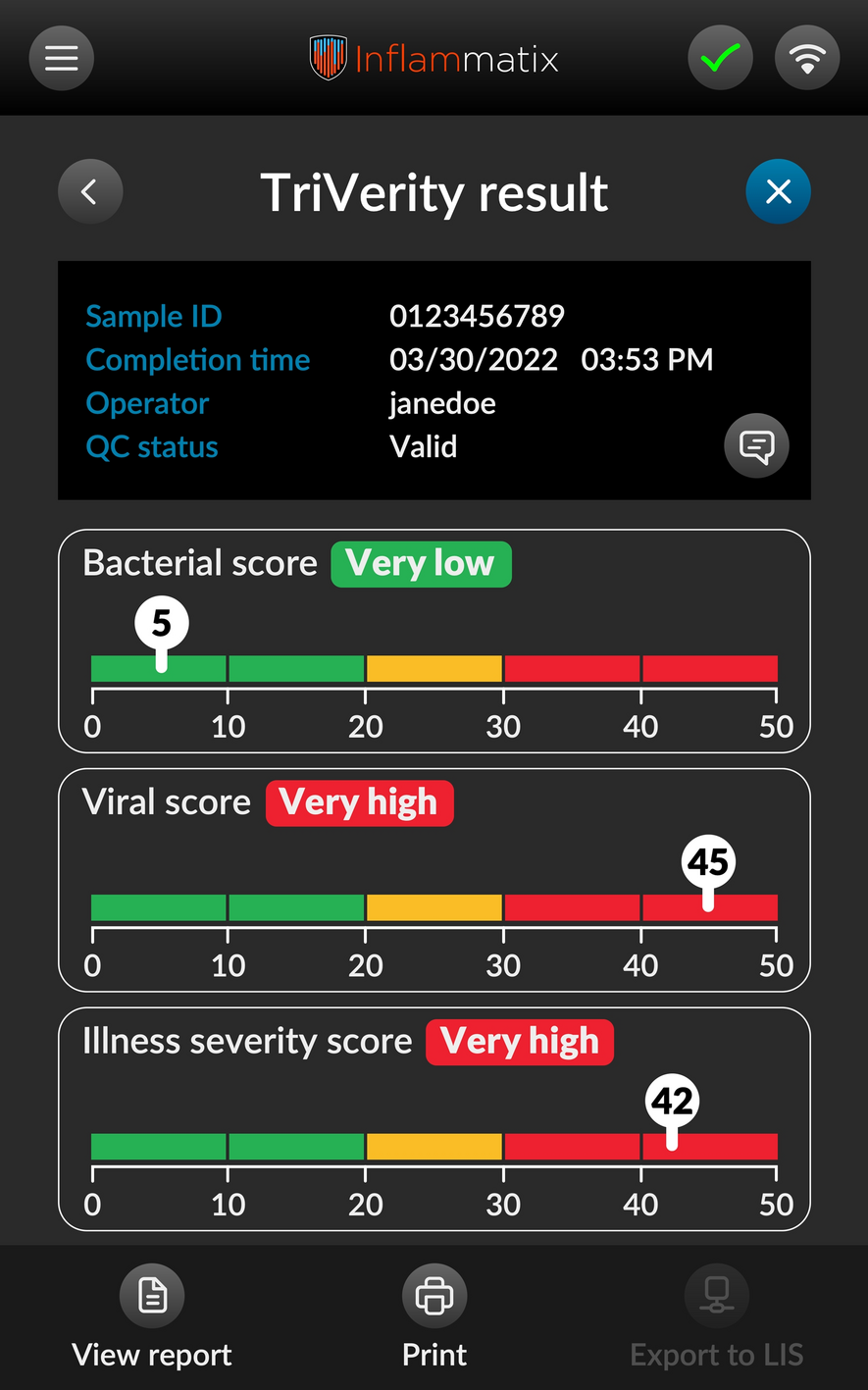
After approximately 30 min, The TriVerity Test, which involves RNA extraction, host gene amplification [19] and machine learning classifiers reading the gene expression, generates three distinct scores in approximately 30 min: likelihood of bacterial infection, viral infection, and illness severity (Fig. 1). These scores are presented in five discrete interpretation bands—very low, low, moderate, high, and very high. Each band offers an indication of the probability and severity of the infection, which may assist clinicians in making informed decisions about patient management.
Fig. 1
TriVerity results output image. The TriVerity Test System is not for sale. It is currently pending FDA clearance and has not received marketing approval or clearance from regulatory authorities in any jurisdiction
Data collection and processingPatient data, including demographics, use of antibiotics and immunosuppressive drugs, and comorbidities were collected at baseline. Bedside monitoring data (i.e., vital parameters) were automatically captured and stored, and information from other data sources (such as the electronic health records) was securely imported. Study data were collected and managed using REDCap electronic data capture tools [20], hosted at the UMCG. The complete Acutelines protocol and a full data dictionary overview are available at www.acutelines.nl.
Clinical adjudication of infection and severity endpointsPost hoc chart reviews were conducted by two independent physicians to determine the adjudicated status of bacterial and viral infections for each case. Each case was assigned to one of four predefined categories—ruled out, unlikely, probable, or rule in—separately for bacterial and viral infections [21]. The detailed definition of the adjudication categories can be found in Supplemental Table 1. In instances where the two adjudicators disagreed, a third reviewer made the final determination. All adjudicators were blinded to the TriVerity bacterial and viral results.
Table 1 Patient demographics segmented by adjudicated infection status established using forced adjudicationThe dataset was used in two ways to convert the four original adjudication categories into a single binary classification for each infection type (i.e., bacterial or viral infection present or absent). To create a unified 'ground truth' label with three possible outcomes (bacterial infection, viral infection, or non-infected), we applied two distinct classifications to the data: 'consensus adjudication' (CA) and 'forced adjudication' (FA).
In the CA approach, only cases classified as 'Rule In' were deemed positive for bacterial or viral infection, while cases marked as 'Ruled Out' were considered absent of the infection. Cases classified as 'Unlikely' or 'Probable' were treated as inconclusive and excluded from further analysis. In contrast, the FA approach required that all cases be classified into binary categories. Here, cases adjudicated as either 'Probable' or 'Rule In' were labeled as positive for bacterial or viral infection, while cases rated as 'Unlikely' or 'Ruled Out' were considered absent of the infection. This provided a broader interpretation to allow analysis of all cases in the dataset.
The primary endpoint of severity was defined as ICU admission and/or mortality due to infection within 7 days of ED presentation. In addition to the patients that were admitted to the ICU or died of an infection, two patients were admitted to the ICU for a non-infectious reason (cardiac arrest secondary to hypoxemia following an allergic reaction to CT-contrast, and ICU admission because of shortage of high-flow oxygen bed at the regular ward) and one patient with advanced esophageal cancer died due to a perforated esophagus. These patients were not labeled as meeting the “severity endpoint”, which concerned only ICU admission or death due to an infection. Physicians were blinded to the TriVerity results.
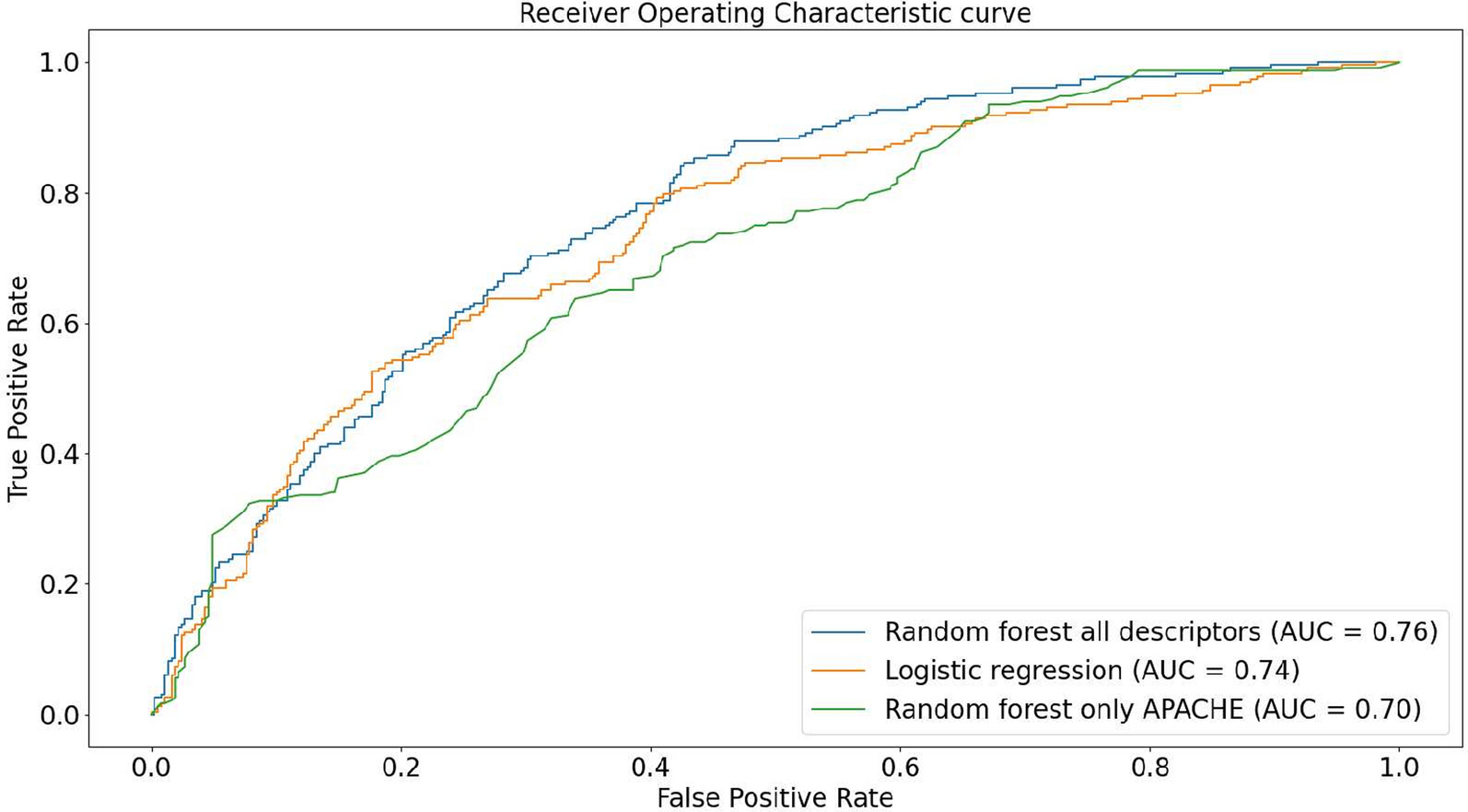
Statistical analysisContinuous variables are expressed as median with interquartile range (IQR). Categorical variables are represented as proportions. A p-value of < 0.05 was considered statistically significant. The performance of TriVerity test was evaluated in two ways: [1] using TriVerity scores through the area under the receiver operating characteristics (AUROCs) and [2] using TriVerity interpretation bands to calculate sensitivity, specificity, likelihood ratios, and positive and negative predictive values [22]. The calculation basis of TriVerity bands performance is demonstrated in Supplemental Table 2. Statistical analyses and figures generation were conducted using R version 4.3.3.
Table 2 Performance of TriVerity results after applying previously established cutoffs to segment scores into clinically interpretable bands
Comments (0)