
Remember me








Chronic obstructive pulmonary disease (COPD) is a progressive lung disease resulting in persistent respiratory symptoms, such as a chronic productive cough, breathlessness, wheezing, and airflow limitation primarily caused by cigarette smoking and other noxious gases. It is characterized by a chronic decline in lung function with irreversible airflow obstruction and systemic manifestations resulting in frequency and severity of exacerbations. COPD exacerbations are defined as acute events described by a worsening of respiratory symptoms that are beyond normal day-to-day variations [,]. COPD exacerbations are the most frequent presentation in the hospital setting, both nationally and internationally. This accounts for a substantial economic burden [,]; for instance, within the European Union, COPD accounts for 56% of the overall respiratory costs annually []. COPD can negatively impact clinical health outcomes, resulting in frequent exacerbations, increased hospitalizations, reduced physical activity, deteriorating quality of life, and a diminished sense of self-efficacy [,,-].
Self-management programs have been shown to improve individual’s knowledge, confidence, and skills to self-manage their chronic illness [,]. This results in improved clinical health outcomes in terms of enhanced quality of life, improved physical activity, and fewer exacerbations, resulting in reduced hospitalizations, morbidities, and premature death among this cohort [,-]. Successful self-management interventions among adults with COPD result in cost-effectiveness for the health care service [-]. Previous studies using self-management programs through a smartphone app have shown a positive effect on clinical health outcomes among this cohort [-]. However, these studies [-] have issues with heterogeneity among interventions used, consistency of their application, patient population specifics, duration of studies, and outcome measures. In addition, studies have suggested that support from a third party, such as a health care professional may improve engagement levels [,,,,]. However, there is no conclusive evidence to support that a third party, such as a health care professional, has a statistically significant impact on engagement levels among this cohort. Therefore, there is a strong need for more research surrounding smartphone apps delivering a comprehensive self-management program for adults with COPD to better understand its role in health care. Furthermore, there is a need to explore whether the use of a third-party involvement, such as a health care professional, to support trial participants in using the app, has any impact on engagement levels.
The use of smartphone apps, remote monitoring, and telemedicine are more frequently used in the delivery of health care both nationally and internationally than before the COVID-19 pandemic [,]. It has also been reported that the COVID-19 pandemic has positively influenced the older population’s views on technology, resulting in increased use of smartphones following the pandemic [,]. Readily available access to educational resources can be a challenge for participants with COPD due to cost, environmental barriers, timing not being suitable, or a lack of transport to travel to these educational sessions []. Smartphones have many benefits, such as providing convenient communication with the patient and health care professional; they offer portability, Bluetooth, and internet connection, allowing for the use of various smartphone apps to work anywhere at any time. In addition, smartphone apps support behavior changes by providing education, interactive feedback, motivational messages, and access to internet-based resources available at any time. Also, they are generally available at a lower cost in comparison to other digital technologies, such as computers or tablets [,,]. However, technology is still evolving [], and the best practices in relation to smartphone apps supporting a comprehensive self-management program are not yet well established.
We conducted a single-center, 3-arm parallel pilot randomized controlled trial (RCT) to explore the effect of a smartphone app self-management program on clinical health outcomes in adults with COPD on a longitudinal basis of 12 months. The main components of this self-management program were monthly education, symptom tracking, communication with a health care professional, goal setting, and weekly motivational messages from the app. Symptom tracking included monitoring physical activity (step count), breathlessness score (modified Medical Research Council dyspnea scale [mMRC]), and recording of clinical parameters (lung function [forced expiratory volume at 1 second, FEV1] and oxygen saturation [SpO2]) using devices such as a spirometer and pulse oximeter. The measurements obtained from the pulse oximeter and spirometer were downloaded through Bluetooth to the self-management app on the participants’ smartphones. This paper provides data about exacerbation rates, engagement, physical activity, breathlessness, health-related quality of life (HRQoL), and self-efficacy.
ObjectiveThe objective of this study was to explore the effectiveness of a smartphone app self-management program and monthly phone calls compared with standard respiratory outpatient care on clinical health outcomes in adults with COPD.
As the concept of this trial was the first of its kind in Ireland, it was important to assess its feasibility; therefore, a single-center pilot trial was conducted. Pilot trials are typically not powered studies as they explore a new concept or intervention or, indeed, a trial design where more data is required before progressing to a larger study []. A statistical package [] was used to calculate the number of participants required for a larger national study that resulted in 1888 participants. A CONSORT (Consolidated Standards of Reporting Trials) checklist was completed to guide the design, analysis, and reporting of trial findings (see ). This trial compared patient outcomes across three arms of the intervention (all in addition to standard respiratory outpatient care): (1) a smartphone app self-management program and monthly phone calls, (2) the smartphone app self-management program alone, and (3) no additional outpatient care. In addition, this trial provides information on the effect size, refusal rates, and attrition rates that will aid in recalculation of the sample size required for the larger multicenter trial.
RecruitmentParticipants who attended the respiratory outpatient department (OPD) and met the inclusion criteria were invited to participate in this study by telephone.
Participants were eligible if they (1) were aged 18 years or older, (2) had a confirmed COPD diagnosis defined as the presence of post-bronchodilator FEV1/FVC<0.70 [], (3) had COPD whose severity was defined by the Global Initiative for Chronic Obstructive Lung Disease guidelines (2023) [] were included, (4) were able to give informed consent, (5) had a smartphone and were able to use it, and (6) had good dexterity to use devices such as a handheld spirometer and pulse oximeter.
Eligible participants were provided with a hard copy of the study information pack, which included a cover letter, an information leaflet outlining the study, an informed consent form, and a returning stamped envelope. Participation in this study was completely voluntary. No financial incentives were offered to participate in this study.
Once written consent was received, a trial register form was completed, and the participant was assigned an ID number. Participants were randomized into each arm using a random allocation computer software package called Random Allocation Software 2.0 []. Given the nature of the trial, it was not feasible to blind participants and the researchers involved, given the type of intervention, a smartphone app. However, the research team was blinded to the allocation of participants to each arm by using allocation concealment. Allocation concealment was achieved using an independent health care worker who retained the random allocation sequence. This guaranteed adequate allocation concealment by preventing those recruiting and entering participants into the study from knowing the next assignment. The researcher gave the independent health care worker the participant ID, which was then recorded to the next randomization sequence number. Permuted block randomization, block sizes of three (allocation ratio of 1:1:1), was used in this study to ensure equilibrium. Participants were randomized into intervention arm 1, which included the smartphone app self-management program and monthly phone calls (n=31), intervention arm 2 included the smartphone app self-management program (n=31), and arm 3 was standard respiratory outpatient care (n=30). Furthermore, outcome assessors were blinded using an independent advanced nurse practitioner who reviewed and confirmed whether the outcome assessment met the primary case definition.
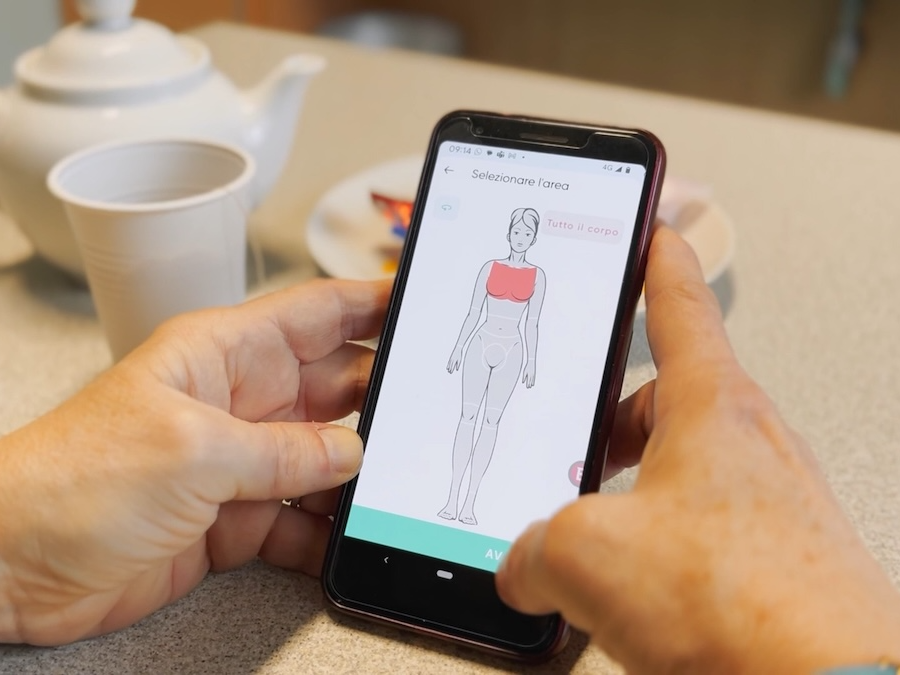
ProceduresThe intervention in this trial was a comprehensive self-management program through a smartphone app (). The main components of this self-management program were monthly education, symptom tracking, communication with a health care professional, goal setting, and weekly motivational messages from the app. Symptom tracking included monitoring physical activity (step count), breathlessness score (mMRC), recording of clinical parameters (lung function [FEV1]), and oxygen saturation (SpO2) using devices such as a Spirobank smart spirometer (), and a Nonin pulse oximeter () that downloaded via Bluetooth to the self-management program app on the participants' smartphone. In addition, 2 educational videos were uploaded to the self-management app each month for 12 months. Educational videos included features relating to self-management, maintaining a healthy lifestyle, and national support available to participants with COPD.
Participants in the intervention arms were sent an email inviting them to download and activate the self-management program app on their smartphones. This email provided participants with a unique username and password. Education in using the app and devices was provided by the research team and the company patientMpower (pMp). Participants in the intervention arms were provided with a hardback intervention study pack that reiterated the information on how to use the smartphone self-management app and the devices (see ). Technical support was provided 5 days a week by pMp, and their contact details were displayed in the app and were provided in the intervention study pack. Participants in the intervention arms were advised to use the app by viewing the educational content, input their mMRC score, and use the devices weekly or more times if they wished for 12 months. The smartphone app self-management program sent a motivational message to the participants twice a week, prompting them to use the app. Participants were informed at the recruitment stage that data were collected retrospectively and was not monitored daily. Data were reviewed during the scheduled visits at 6 and 12 months. Participants were informed that the smartphone self-management app was not a replacement for their standard medical care, and in the event of a deterioration in their health status, they should contact their general practitioner (GP) or hospital for medical attention. On completion of the trial, app usage was analyzed to determine participants’ engagement with the app over the 12 months.
Participants allocated to arm 1 received the self-management app along with monthly phone calls from a health care professional and standard respiratory outpatient care. The aim of the monthly phone calls was to provide support to participants using the app. Participants assigned to arm 2 received the self-management app and standard respiratory outpatient care. Participants in arm 3 received standard respiratory outpatient care.
Participants in all the arms of this trial received standard respiratory outpatient care, which consisted of routine visits by telephone at 6 and 12 months from the respiratory OPD at the research site. During these visits, participants informed the research team of any GP and or hospital visits as a result of an exacerbation of COPD. In addition, they informed the team of their physical activity (exercise behavior, capacity, and step count), breathlessness score (mMRC), nutritional intake, pulmonary rehabilitation, medication adherence, smoking status, vaccinations, and if they had contracted the COVID-19 virus. Finally, they completed questionnaires on the burden of symptoms, quality of life, self-efficacy, and user engagement scale (arm 1 and arm 2 only). Participants were also given self-management education and advice during these visits.
It was anticipated that using the self-management app that provided monthly education, motivation, support from a health care professional, and objective data would enhance participants’ knowledge and self-care skills to better manage their chronic illness. This may improve clinical health outcomes, reduce hospitalizations and hospital-associated complications, thereby reducing morbidity, mortality, and overall health care costs among this cohort. The clinical outcomes evaluated in this trial were exacerbation rates, levels of engagement, physical activity, breathlessness, quality of life, and self-efficacy.
 Figure 1. Smartphone self-management app. FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; mMRC: modified Medical Research Council Dyspnea Scale.
Figure 1. Smartphone self-management app. FEV1: forced expiratory volume at 1 second; FVC: forced vital capacity; mMRC: modified Medical Research Council Dyspnea Scale.  Figure 2. Spirobank smart spirometer.
Figure 2. Spirobank smart spirometer.  Figure 3. Nonin pulse oximeter. Primary Outcomes
Figure 3. Nonin pulse oximeter. Primary OutcomesThe primary outcome was a binary indicator equal to 1 if participants reported attendance to a GP and or a hospital setting as a result of an exacerbation and 0 otherwise. This indicator was recorded at 6 months and 12 months from the baseline.
Secondary OutcomesThe first secondary outcome was engagement, which measured viewing the activation rates of the app and devices over 12 months and through the use of a user engagement scale. Also, participants were contacted by phone at 3, 6, and 12 months to complete the refined user engagement scale [].
Second, physical activity was measured at baseline, 6, and 12 months as the participant reported exercise capacity (participant reported) and step count.
Third, breathlessness was measured using the mMRC scale [] at baseline, 6, and 12 months. Higher scores represent the severity of breathlessness.
Fourth, the chronic obstructive pulmonary disease assessment test (CAT) [] score was measured at baseline, 6, and 12 months. Higher scores signified the greater burden of COPD had on the participants’ overall health and well-being.
Fifth, the HRQoL was measured using the clinical COPD questionnaire [] at baseline, 6, and 12 months. Higher scores illustrated poorer HRQoL.
Sixth, self-efficacy was measured using the Self-Efficacy for Managing Chronic Disease 6-Item Scale at baseline, 6, and 12 months []. Higher scores resulted in greater self-efficacy.
Statistical AnalysisThe change in an outcome was considered statistically significant when P<.05. All data were analyzed using an intention-to-treat analysis (ITT), resulting in all participants in their allocated arm being followed up to trial completion (12 months). To correlate with the principle of ITT analysis, all participants in this trial were kept in their assigned arms, and sensitivity analysis was conducted. Sensitivity analysis was performed by using the negative outcome for participant attrition (loss of participants to follow up) in the intervention arms (exacerbation of COPD) and participant attrition in the control arm to have the best outcome (no exacerbation of COPD), and this was repeated vice versa. Sensitivity analysis results were compared with the original analysis. This assessed the probable impact of participant attrition, resulting in an unbiased estimate of the true effect of the intervention.
Summary statistics were calculated, with the frequency and the percentages being reported for categorical variables. Continuous variables are presented as mean (SD). Finally, for ordinal variables, median and IQR were reported since they were not normally distributed as determined by the Shapiro-Wilk test. To test for significance between baseline and intervention effectiveness using categorical data, the chi-square, and Fisher exact test were used. Fisher exact test is often used for smaller sample sizes. Independent t tests were used to compare the mean difference of continuous outcomes between the intervention (arms 1 and 2) versus the control arm (arm 3). Furthermore, the relative risk and absolute risk reduction, along with the associated 95% CI, were used on all outcomes of this study. The ANOVA test was used for continuous variables (dependent variable) to investigate for a significant difference. In relation to the ordinal variables, the Mann-Whitney U test was completed to compare differences between arm 1 and arm 2. The Kruskal Wallis test was completed for ordinal variables to determine a statistically significant difference between the three arms, arm 1, arm 2, and arm 3. The logistic model was used to explore the disparities between the three arms in relation to the primary outcome over time. This provided estimates of the probability of developing a COPD exacerbation over time in each arm, resulting in a GP or hospital visit. The possible influencing factors in developing an exacerbation were included, such as age, gender, time, severity of disease, comorbidities, and smoking history. This data was presented as both adjusted and unadjusted odds ratios (OR) and their corresponding 95% CIs for each variable. In addition, the generalized linear mixed model (GLMM) was used as participants were measured at two different time points, 6 and 12 months. This model is an extension of the logistic regression model, which identifies the correlation exhibited by longitudinal data. The GLMM was used because there were categorical outcomes measured over time resulting in correlated data. The logistic regression model ignores the fact that this data is correlated, thereby ignoring this correlation.
Ethical ConsiderationsThis study was approved by the St James' Hospital and Tallaght University Hospital Joint Research Ethics Committee, Dublin, Ireland on July 02, 2021. This trial adhered to the rights of the persons, and each participant had the right to make an informed, voluntary decision to participate in this trial. Eligible participants were provided with verbal and written study information packs. Participants had the right to withdraw from this trial at any stage. To adhere to privacy and confidentiality, each participant was assigned a trial identification number and this number was used on all trial documentation. The pseudoanonymized data were stored in a password-protected shared folder at the study center, which was only accessed by the research team. In addition, monetary rewards were not offered for participation in the trial. The ClinicalTrial.gov ID assigned to this study was NCT05061810.
A total of 234 participants were assessed for eligibility from August 2021 to February 2022. From this sample, 202 participants were eligible, and 32 participants were not eligible as they did not meet the inclusion criteria. The main reasons for ineligibility were no smartphone, digital literacy, reduced dexterity, therefore, unable to use the devices, dementia, and blindness. From the sample of 202 eligible participants, 110 participants refused to participate in the trial for various reasons such as “not interested,” “had no time” (n=90), or “ongoing medical investigations” (n=20; see for the CONSORT flow diagram).
A total of 92 participants were randomized to each arm, 31 participants were allocated to arm 1, 31 participants were allocated to arm 2, and 30 participants were allocated to arm 3 (). There were 8 participants who were lost to follow-up. Data were collected at the following time points: baseline, 3 (user engagement only), 6, and 12 months. The mean age of participants was 66.8 (SD 7.9) years, ranging from 45 to 81 years of age. There were 57% (52/92) females in the study, with most participants having moderate airway obstruction (43/92, 47%), see . There were no significant differences in the distribution of baseline characteristics across the three arms except for the variable pulmonary rehabilitation (). A substantial proportion (84/92, 91%) of the participants reported not engaging with pulmonary rehabilitation at baseline. As this study was conducted during a respiratory pandemic, COVID-19, routine face-to-face pulmonary rehabilitation was not operating due to the Government imposed lockdown restrictions. There was a statistically significant difference, P=.01, among the three arms concerning the participants who underwent pulmonary rehabilitation engagement and those who did not (). Post hoc pairwise comparisons with Bonferroni correction indicated that arm 1 and arm 2 were different from each other with a P=.02, with more participants in arm 2 participating in pulmonary rehab in comparison with arm 1. No adverse events were reported during this trial.
 Figure 4. CONSORT flow diagram. ITT: intention-to-treat analysis. Table 1. Baseline characteristics of trial participants (N=92).
Figure 4. CONSORT flow diagram. ITT: intention-to-treat analysis. Table 1. Baseline characteristics of trial participants (N=92).aCCI: Charlson Comorbidity Index.
bCAT: chronic obstructive pulmonary disease assessment test.
cmMRC: modified Medical Research Council Dyspnea Scale.
Table 2. Baseline characteristics by the randomized arm.VariableArm 1 (n=31)aArm 2 (n=31)bArm 3 (n=30)cP valueSex, n (%).63aArm 1 includes a self-management app, monthly phone calls, and standard respiratory outpatient care.
bArm 2 is the self-management app and standard respiratory outpatient care.
cArm 3 is standard respiratory outpatient care, the control group.
dCCI: Charlson Comorbidity Index.
emMRC: modified Medical Research Council Dyspnea Scale.
fCAT: chronic obstructive pulmonary disease.
COPD Exacerbations Reviewed in the GP and Hospital SettingsThe proportion of participants in each arm that experienced exacerbations in the hospital and GP setting is reported in . There was a statistically significant difference in the proportion of participants who had a COPD exacerbation versus those who did not have an exacerbation at 6 months in the hospital setting across the three arms, P=.03 (). Post hoc pairwise comparisons (P=.02) revealed that intervention arm 2 experienced fewer exacerbations reviewed in the hospital setting than those in the control arm. The intervention arms had significantly lower odds of developing a COPD exacerbation in both the GP (with an adjusted OR of 0.20 (95% CI 0.06-0.61; P=.005) and hospital (OR 0.26, 95% CI 0.07-0.99; P=.049 and OR 0.18, 95% CI 0.04-0.78, P=.02) setting compared with the control arm (). The probability of developing a COPD exacerbation for participants with severe severity is 6.55 times significantly higher than for participants with moderate severity, with P=.009 (). There was a statistically significant difference (P=.01) at 6 months in the GP setting, indicating that the intervention arm had a lower risk of developing an exacerbation than the control arm (). The control arm had the highest estimated probability of having a COPD exacerbation over time, see . At 6 months, in the hospital setting, there was a statistically significant difference (P=.01 and P=.006), indicating the intervention arms had a significantly lower risk of developing a COPD exacerbation compared with the control arm (). However, after 6 months of follow-up, there was a sharp increase in all the arms, with the control arm having the highest and the intervention arms having the lowest estimated probabilities of developing an exacerbation (). The risk of developing an exacerbation was 0.04 times lower for participants with mild severity compared with participants with severe severity, with a statistically significant (P=.02; ). Sensitivity analysis indicated a significant difference at 12 months (P=.02), where the intervention arms experienced fewer exacerbations than the control arm at 12 months (see ). Participants with missing data in the control arm were assumed to have experienced an exacerbation (negative outcome), while participants with missing data in the intervention arms (arms 1 and 2) were considered to have experienced no exacerbation (best outcome). However, these results may not accurately reflect the true outcomes of participants with missing data, leading to differences in statistical significance.
Table 3. Comparison of proportions of participants with and without an exacerbation in the general practitioner (GP) and hospital settings across arms.VariableArm 1 (n=31)Arm 2 (n=31)Arm 3 (n=30)P valueHospitalaOR: odds ratio.
bArm 1 includes a self-management app, monthly phone calls, and standard respiratory outpatient care.
cArm 2 is the self-management app and standard respiratory outpatient care.
dNot applicable.
Table 5. Logistic model results for general practitioner (GP) setting.VariableBaseline6 months12 months
Comments (0)