Data Source
Claims data from January 2011 to June 2022 from the IQVIA PharMetrics® Plus database were used. The IQVIA database includes fully adjudicated medical and pharmacy claims data and is representative of the commercially insured US population under 65 years of age. Information available in the database includes inpatient and outpatient diagnoses and procedures, prescription fills and outpatient-administered treatments, dates of service, costs, demographic variables (i.e., age, gender, geography), plan type, and monthly indicators of health plan enrollment. To protect privacy rights, the database publication guidelines require any cell sizes with N < 5 to be suppressed.
The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514.
Study Design and Patient Selection
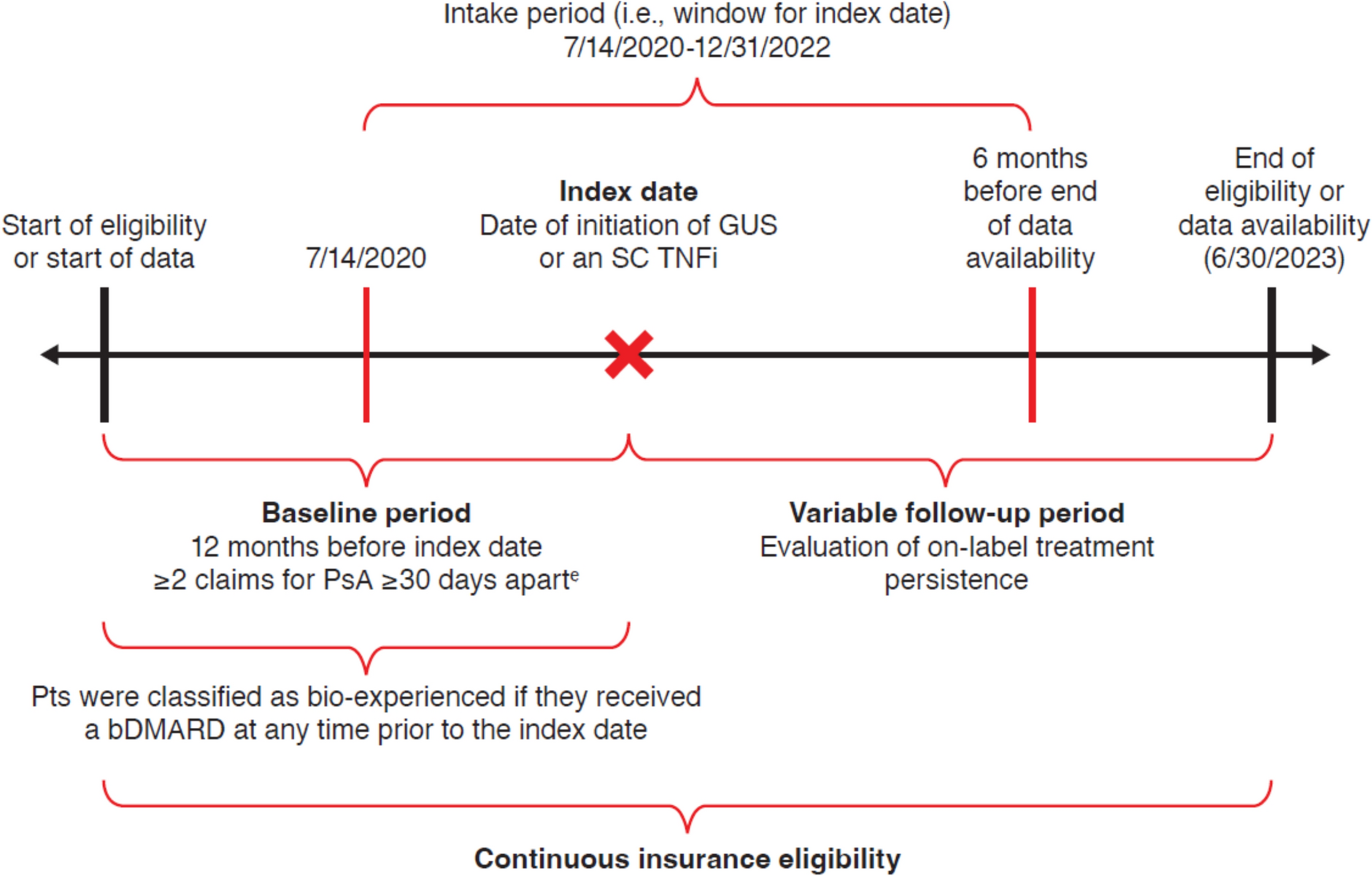
In this retrospective cohort study, commercially insured adults (≥ 18 years) with IgG4-RD were identified using a validated algorithm developed by Wallace et al. [14], since International Classification of Disease (ICD) codes were not available for IgG4-RD at the time of the study. The index date was defined as the first observed IgG4-RD-related diagnosis code used to fulfill the algorithm requirements. The baseline period was defined as the 12 months prior to the index date, and the study period included the 12 months following the index date. Patients were required to have continuous health plan enrolment during both the baseline and study periods.
The cohort was stratified into two mutually exclusive groups based on glucocorticoid use during the study period: (1) “low glucocorticoid use” group, consisting of patients with a mean prednisone equivalent daily dose (PEDD) of < 5 mg, including patients with no glucocorticoid use; and (2) “high glucocorticoid use” group, consisting of patients with a mean PEDD of ≥ 5 mg. PEDD was assessed based on observed prescription fills of all relevant systemic (i.e., oral, intravenous, injected) glucocorticoids (i.e., prednisone, prednisolone, methylprednisolone, and dexamethasone). Only glucocorticoids received in a pharmacy setting (i.e., prescription fills) were included in the analysis because pharmacy data contain the necessary information to assess PEDD (i.e., quantity and strength). Glucocorticoids received in a medical setting (i.e., outpatient, inpatient, or emergency department) were not included in the analysis since PEDD could not be reliably assessed without complete data on dosage [15,16,17]. PEDD was calculated per patient as cumulative prednisone equivalent dose during the study period divided by 365 days [15,16,17]. The daily threshold of 5 mg was based on prior literature assessing glucocorticoid burden and toxicity in rheumatic conditions and discussions with experts [15, 16].
Study Measures and Statistical Analysis
Patient demographic characteristics (i.e., age, sex, region of residence, primary health plan type) were described on the index date and clinical characteristics (i.e., glucocorticoid use, IgG4-RD-related treatments, manifestations of IgG4-RD, specialists involved in care, Charlson Comorbidity Index [CCI], IgG4-RD-related comorbidities) were assessed during the study period. IgG4-RD-related treatments included the glucocorticoids described above and non-steroidal immunosuppressants (i.e., azathioprine, methotrexate, mycophenolic acid, mycophenolate mofetil, rituximab, and its biosimilars). National Drug Codes were used to identify all treatments, and Healthcare Common Procedure Coding System codes were also used to identify rituximab and its biosimilars. Patients were considered to have a manifestation of IgG4-RD (i.e., pancreatic, biliary, sialadenitis, lacrimal, retroperitoneum, mesenteritis, orbit, aortitis) if they had ≥ 1 corresponding ICD-9/10 code for that manifestation during the study period, as previously defined by Wallace et al. [14] Billing provider codes for medical services were used to identify specialists involved in care. Patients were considered to have an IgG4-RD-related comorbidity if they had ≥ 2 corresponding ICD-9/10 codes on different dates at least 30 days apart.
Incident glucocorticoid-related toxicities were described separately for each group during the study period and were defined as toxicities with ≥ 1 diagnosis code during the study period and no diagnosis during the baseline period. Glucocorticoid-related toxicities were reported individually and by organ system (i.e., cardiovascular, gastrointestinal, infections, metabolic/endocrine, musculoskeletal, neuropsychiatric, ophthalmologic) and were informed by prior literature and discussions with experts [9, 18].
Means, medians, and standard deviations (SDs) were reported for all continuous variables; frequency counts and percentages were reported for all categorical variables. The rates of incident glucocorticoid-related toxicities were compared between the low and high glucocorticoid use groups using Chi-square tests, with unadjusted p values reported. All analyses were conducted using the Statistical Analysis System (SAS) Enterprise Guide, Version 7.1 (SAS, Cary, NC, USA).
Subgroup Analysis
All analyses were replicated among a subgroup of the overall cohort of patients with IgG4-RD that had ≥ 1 diagnosis for a pancreatic and/or biliary manifestation during the study period, as defined above.


Comments (0)