SWEBIC-I recruitment
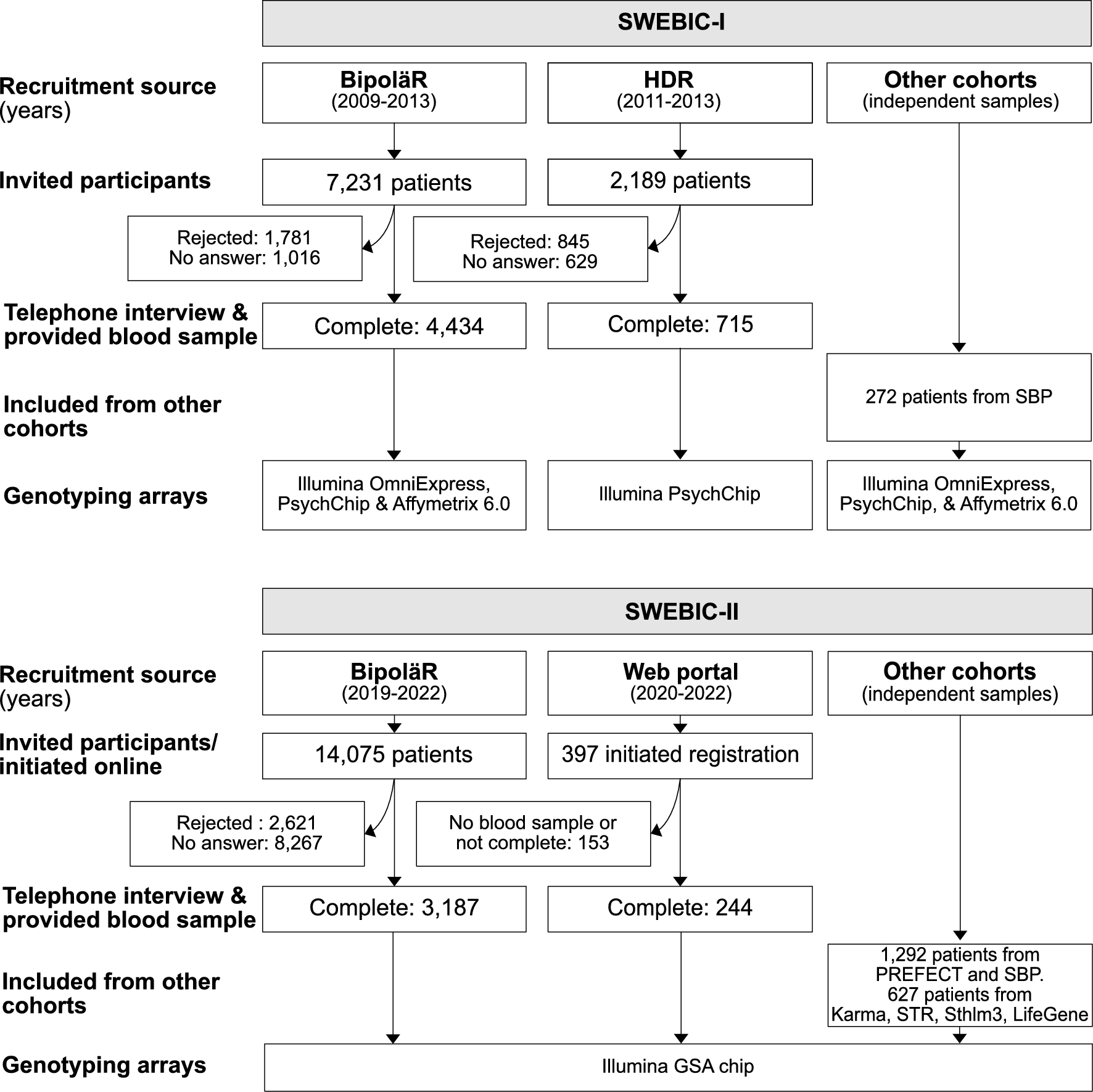
From 2009 to 2013, the first wave of the Swedish bipolar collection (SWEBIC-I, https://ki.se/meb/swebic) recruited participants from two primary sources: (1) the Swedish National Quality Register for bipolar disorder (BipoläR) (Pålsson, et al. 2022), and (2) the Swedish Hospital Discharge Register (HDR). An invitation letter was sent to all individuals in the identified patient groups, followed up by a phone call attempt. Those who agreed to participate were scheduled for a telephone interview and provided a blood sample at their nearest lab. In addition, SWEBIC-I included cases from the St. Göran Bipolar Project (N = 272), a longitudinal clinical cohort of individuals with bipolar disorders (Landén, et al. 2025).
The Swedish national quality register BipoläR
For a review of Swedish Quality Registers, see Emilsson, et al. (2015). The Quality Register for bipolar disorders—BipoläR—was launched in 2004 with the aim of improving the quality of bipolar disorder care (Pålsson, et al. 2022). Individuals with bipolar disorder treated at psychiatric outpatient clinics in Sweden are eligible for inclusion and annual follow-up in BipoläR. Patients are informed about their registration and have the option to opt-out. It is voluntary for participating outpatient units and treating psychiatrists to contribute data to BipoläR. Data, including diagnoses, registered in BipoläR are entered by the treating psychiatrist, who is usually specialised in the diagnosis and treatment of bipolar disorder and has access to all clinical data. Individuals can be included in BipoläR at any time after their initial bipolar disorder diagnosis. Following initial registration, annual follow-ups are conducted to collect clinical data from the previous 12 months, including occupational status, comorbidities, substance misuse, recurrence of mood episodes, suicide attempts, treatments for bipolar disorder, severity of illness rated with the Clinical Global Impression (CGI-S), health-related quality of life rated with EQ-5D, as well as measurements of lithium serum levels, kidney function, HbA1c, blood pressure, weight and height.
Swedish hospital discharge register (HDR)
The HDR is part of the Swedish National Patient Register, maintained by the National Board of Health and Welfare. HDR is based on mandatory reporting of diagnoses made during inpatient health care contacts in Sweden (Ludvigsson, et al. 2011). The HDR includes hospital discharge diagnoses in accordance with the World Health Organization’s International Classification of Diseases (ICD). Since 1973, the HDR has full coverage of inpatient psychiatric care and diagnoses according to ICD-8 (1973–1986), ICD-9 (1987–1996), or ICD-10 (1997–). We identified individuals with bipolar disorder in HDR using a validated algorithm for register-based identification of bipolar disorder, which has a positive predictive value of 0.92 (Sellgren, et al. 2011). This algorithm requires at least two separate discharge diagnoses of bipolar disorder and allows for a maximum of one lifetime schizophrenia diagnosis to exclude individuals with schizophrenia as their main diagnosis.
SWEBIC-II recruitment
The second wave of recruitment, SWEBIC-II, began in 2017 and concluded in 2022. Bipolar disorder cases were identified and recruited from BipoläR using the same procedure as in SWEBIC-I. We also recruited cases from the general population through an online questionnaire described below. In addition, we used HDR diagnoses to identify individuals with bipolar disorder in other cohort studies not described here: First, from our own PREFECT (Predictors for ECT) study (N = 896) (Clements, et al. 2021; Sigström, et al. 2022, 2020) and the St. Göran Bipolar Project (N = 396) (Landén, et al. 2025). Second, from cohort studies conducted by colleagues, including Karma (a breast cancer study, N = 93) (Gabrielson, et al. 2017), the Swedish Twin Registry (N = 260) (Zagai, et al. 2019), the Stockholm 3 study (a prostate cancer study, N = 74) (Gronberg, et al. 2015), and the LifeGene study (N = 200) (Almqvist, et al. 2011).
Online recruitment
In SWEBIC-II, we additionally used a dedicated web portal and a secure online registration form to recruit individuals with bipolar disorder from the general population. To raise awareness of the web portal, we reached out to patient organizations and used other websites and social media platforms. Participants identified themselves using ‘BankID’, a Swedish service for secure online electronic identification and signature. Instead of being interviewed on the phone by a research nurse, participants completed an online questionnaire containing the same questions as the telephone interview. After submission, they were instructed to provide a blood sample at their nearest hospital or laboratory. We validated the diagnosis in subjects who registered online based on national register data as described in the supplementary methods and results.
Telephone interviewDescription
Individuals with bipolar disorder recruited from BipoläR and HDR completed a structured telephone interview conducted by trained research nurses (see supplement for data dictionary). Since not all information in BipoläR is available in HDR, the interviews were tailored based on mode of ascertainment. For instance, the interview with participants recruited from HDR included additional questions to determine the subtype of bipolar disorder, which cannot be reliably extracted from ICD-10 codes available in the HDR.
The interview collected information about (1) the study participants’ place of birth, as well as the birthplaces of their parents and grandparents, (2) selected somatic diseases as well as height and weight, (3) nicotine, alcohol, and illicit drug use, and (4) disease course and outcomes, history of psychotic symptoms, comorbid psychiatric conditions, pharmacological treatment responses and side effects, as well as family history of psychiatric disorders.
In SWEBIC-II, we added questions regarding response lithium treatment response (detailed below), questions regarding response and side effects from electroconvulsive treatment, and the Montgomery-Åsberg Depression Rating Scale (MADRS) to the telephone interview.
Treatment response and adverse effects
Participants who had used a mood stabilizer (lithium, valproate, lamotrigine, and carbamazepine) were asked to evaluate its effectiveness. The question posed was: “What do you think about its effect? Do not consider any potential side effects.” Based on participant’s responses, the research nurses categorized the answers into one of three predefined response options: (1) Complete treatment response. Mainly free from episodes during treatment. Essentially healthy. “I recovered, it helped me.”; (2) Clearly improved, but suffered continued mood episodes, or needed temporary/continuous additional treatment; and (3) No, or very uncertain treatment effect. From 2018 onwards in SWEBIC-II, the Retrospective Criteria of Long-Term Treatment Response in Research Subjects with Bipolar Disorder (Duffy, et al. 2007; Garnham, et al. 2007; Manchia, et al. 2013), also known as the Alda scale, was added to the questionnaire for participants who had used lithium for at least 6 months. The Alda scale is designed to measure lithium treatment response specifically in individuals on lithium monotherapy. The scale was modified for individuals treated with a combination of lithium and lamotrigine so that they were first asked if they previously had been on lithium monotherapy. If they had, the Alda scale was conducted for the period during which they were on lithium monotherapy. If they had not, we conducted the Alda scale but deducted two points on question B5 to account for the combination therapy.
There is a risk for treatment emergent switch to mania when antidepressants are used in bipolar disorder (Viktorin, et al. 2014). Therefore, participants were asked if they had experienced a switch to (hypo-)mania within 12 weeks of starting an antidepressant treatment. As weight gain is a common side effect of antipsychotics, participants were also asked whether they had experienced significant weight gain—defined as an increase of at least 7%—within 3 months of starting atypical antipsychotic treatment. Response options included ‘Yes’ or ‘No, or less than 7%’.
Data completeness and missingness
Overall, the level of missing data in the structured telephone interviews was low, as the interviews were conducted by trained research nurses using standardized protocols with predefined response options. However, some variability in completeness exists across recruitment waves. For example, variables such as lithium treatment response rated by the Alda scale were introduced during SWEBIC-II and are missing for participants recruited in SWEBIC-I. Moreover, participants recruited from external cohorts (e.g., Karma, STR, Sthlm3, LifeGene) did not complete the telephone interview and therefore lack corresponding interview-based phenotypic data. Annual follow-up data in BipoläR are collected as part of routine clinical care, not specifically for this study, and their completion is not mandatory for either clinicians or patients. Consequently, the completeness of these data may vary across individuals and over time.
Bipolar disorder subtypes
We used information from the quality registry BipoläR to identify bipolar disorder subtypes. For individuals without BipoläR data, we determined the subtype based on responses from the telephone interview and the online questionnaire. For subjects recruited from PREFECT, we used BipoläR data when available. For subjects recruited from the Swedish Twin Register, the Stockholm 3 study, and Karma, no direct information on bipolar disorder subtype was available. In these cohorts, subtypes were classified based on ICD-10 diagnoses as follows: bipolar disorder subtype 1 (F30.1, F30.2, F31.1, F31.2, F31.6, and F31.7), bipolar disorder subtype 2 (F31.8), and bipolar disorder not otherwise specified (NOS, F31.9).
Blood sampling and genotyping
Kits for blood sampling were sent to participants, who were asked to have their blood drawn at their nearest hospital or laboratory. Blood samples were collected in EDTA tubes and sent via overnight mail to the Karolinska Institutet Biobank. Upon arrival, the samples were centrifuged for 10 min at 2000 g. Plasma was then apportioned into 225 µl aliquots and stored at − 80 °C. DNA was extracted from whole blood and subsequently stored at − 20 °C.
DNA samples were subsequently sent to the Broad Institute (Massachusetts, US) for genotyping. Individuals in SWEBIC-I ascertained from BipoläR were genotyped using Affymetrix 6.0 (Affymetrix, Santa Clara, CA, USA), Illumina’s OmniExpress and Infinium PsychArray-24 v1.2 BeadChip (Illumina, San Diego, CA, USA), while individuals ascertained from HDR were genotyped using PsychArray. In SWEBIC-II, genotyping was carried out using Illumina Infinium Global Screening Array (GSA). SWEBIC has also been whole exome sequenced (Illumina, San Diego, CA, USA) in collaboration with the Bipolar Sequencing Consortium.
Diagnostic validity of diagnoses in BipoläR
As most individuals included in SWEBIC were ascertained from the quality register BipoläR, we analysed the validity of the registered bipolar disorder diagnoses in BipoläR.
Population for validation study
To select a representative sample for validation of bipolar disorder diagnoses, every 50 th participant consecutively ascertained from BipoläR in SWEBIC-I was selected for validation, up to a total sample of 150 patients. We requested the medical records of these patients from the psychiatric clinics where they had received their care.
Clinical assessment
Three board certified psychiatrists (A.K., O.Z., and L.M.) independently reviewed the medical records. The raters were blinded to the diagnoses in BipoläR. The raters first assessed whether patients met criteria for any bipolar spectrum disorder. Second, patients were classified according to the bipolar subtypes: type 1, 2, NOS, cyclothymia, or schizoaffective disorder. If the medical records did not provide sufficient information to determine a specific subtype diagnosis, the raters could select from broader categories coded as “subtype 1 or schizoaffective disorder”, “subtype 1 or 2”, “subtype 2 or NOS” or “other combinations”.
After each rater had classified patients individually, cases were reviewed at consensus meetings attended by the three raters and an additional blinded board-certified psychiatrist (M.L.). In instances where the three raters did not concur, discrepancies were discussed by the group and medical records were re-evaluated. Finally, a consensus diagnosis was reached.
Statistical analyses
The validity of diagnoses in BipoläR and the inter-rater agreement for the consensus diagnoses were examined as follows. Diagnostic validity was assessed using positive predictive value (PPV). The board consensus diagnosis agreed upon by our three raters was regarded as the “true positive” value. The diagnoses in BipoläR included both “true” and “false” diagnostic values. We then calculated the proportion of individuals where the diagnosis in BipoläR matched the rater’s consensus diagnoses.
In the first PPV calculations, we included all individuals and the broader diagnosis categories described above were counted as a ‘hit’. In the second PPV calculations, we included only individuals with a non-ambiguous consensus diagnosis. We also assessed the overall reliability and agreement between the consensus diagnoses and the diagnoses recorded in BipoläR using Kappa measurements. Finally, we used Fleiss’ kappa for more than two raters to test the inter-rater reliability for the diagnoses across the board.
Clopper-Pearson exact confidence intervals and P-values were calculated using the R packages PropCI and irr (the kappam.fleiss function), respectively.
Comparison of participants and non-participants
To evaluate potential differences between SWEBIC participants and the broader BipoläR cohort, we compared the groups with respect to sex, bipolar disorder subtype, medication use, employment status, and global assessment of functioning (GAF) scores using logistic regression (Table S1).
Ethical considerations
The SWEBIC study was approved by the Regional Ethical Review Board in Stockholm, Sweden (DNR:2008/2009-31/2 and 2016/1363-32). All participants provided written informed consent in accordance with the Declaration of Helsinki.





Comments (0)