
Remember me








Of the 401 patients enrolled in the study, more than half (51.1%) were male participants, with a mean age of 49 years (standard deviation (SD) ± 19 years), and 8.7% of the participants were younger than 18 years. Regarding the substance use history of the participants, 14.5% of them were smokers, and 41.1% had a history of alcohol use, as shown in Table 1.
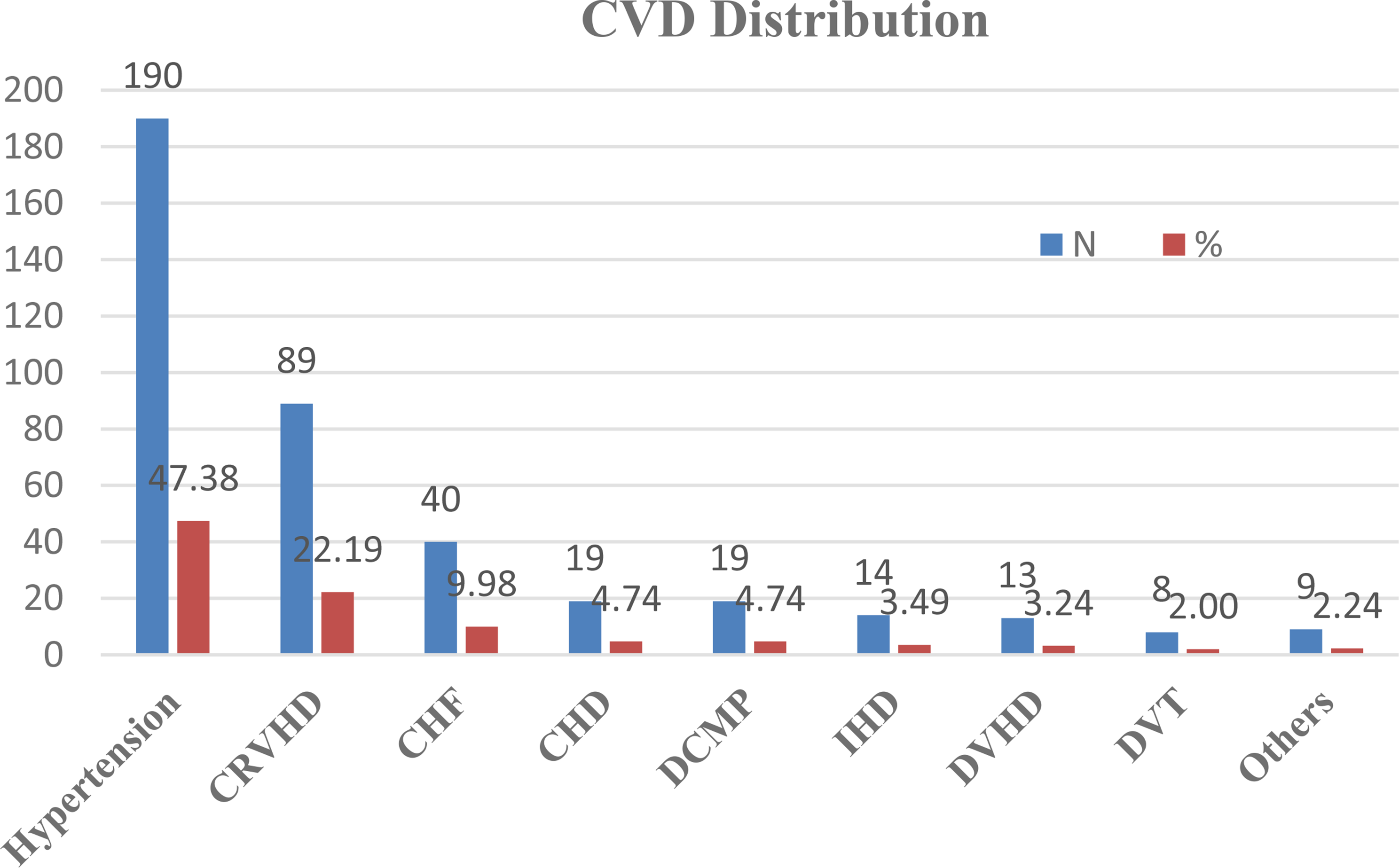
Table 1 Socio-demographic characteristics of patients with CVD admitted to TASH (N = 401)Clinical characteristics of the study participantsPast medical historyAccording to the participants’ medical history, hypertension was the most common initial diagnosis, accounting for 47.4% of cases. This was followed by chronic rheumatic valvular heart disease (CRVHD) (22.2%) and congestive heart failure (CHF) (10%), as shown in Fig. 1.
Fig. 1
The distribution of cardiac disease among the study participants. * Aortic aneurysm, post-TB pericarditis, coarctation of the aorta, arrhythmia CRVHD: chronic rheumatic valvular heart disease, CHF: chronic heart failure, CHD: congenital heart disease, DCMP: decompensated cardiomyopathy, IHD: ischemic heart disease, DVHD: degenerative valvular heart disease, DVT: deep vein thrombosis
Emergency admission diagnosesMost study participants were admitted to the ED with a diagnosis of congestive heart failure (CHF)/acute decompensated heart failure (ADHF), accounting for 37.4% of cases. This was followed by hypertension (26.2%), acute kidney injury/chronic kidney disease (15.5%), and atrial fibrillation (9.5%) (Table 2).
Table 2 Study participants’ admission diagnosis (n = 401)Medication characteristics of the study participantsPast medication historyPatients were taking 1 1 10 medications before the current emergency admission, with a median of two (IQR: 2–4). The most common number was two (26.4%), while 8.5% had unspecified numbers (Table 3).
Table 3 Number of participants’ past medicationsMedication during emergency department admissionDuring ED admission, all participants were taking a minimum of one medication and a maximum of 11 medications per patient, with a median of four (IQR: 3–5). The most commonly used drug classes were diuretics (70%), beta-blockers (36%), and calcium channel blockers (29.4%). Specifically, furosemide was the most frequently prescribed medication, used by 63.3% of the participants, followed by spironolactone (27.7%), amlodipine (24%), metoprolol and enalapril (22.6% each), digoxin (20%), and atorvastatin (18%) (Table 4).
Table 4 Study participants’ medication characteristics during ED admissionLength of ED stay and duration of CVDsThe median length of ED stay for the study participants was five days (IQR: 4–6 days), ranging from a minimum of one day to a maximum of 13 days. The median duration of CVD was four years (IQR: 2–6 years), with a minimum of three months and a maximum of 30 years. The majority of participants (> 50%) had a CVD duration of one - five years (Table 5).
Table 5 Length of ED stay and duration of CVD for patients admitted to the ED of TASHOutcomes of emergency department admissionDuring the study period, 9.5% (n = 38) of patients with CVD admitted to the ED died. Of these, 23.7% (n = 9) of deaths were secondary to DRPs. The leading cause of death was acute decompensated heart failure (ADHF), accounting for 50% of deaths, followed by hypertension (23.7%) and atrial fibrillation (18.4%), as shown in Fig. 2.
Fig. 2
Causes of Death among study participants. ADHF: acute decompensated heart failure, AKI: acute kidney injury, CKD: chronic kidney disease, DVT: deep vein thrombosis, MI: myocardial infarction, PHTN: pulmonary hypertension
Predictors of poor outcomes in patients with CVD during ED admissionVariables with a p-value less than 0.25 in the bivariate Cox regression analysis were included in the multivariate Cox regression analysis. Factors associated with a higher risk of early death in the bivariate analysis included marital status, rural residence, smoking history, primary cardiac disease, dilated cardiomyopathy (DCMP), ischemic heart disease (IHD) as initial diagnosis, comorbid gastrointestinal (GI) disease, polypharmacy, and admission diagnosis of acute decompensated heart failure (ADHF)/congestive heart failure (CHF) and atrial fibrillation. In the multivariate Cox regression analysis, smoking history (AHR = 3.71, 95% CI: 1.54–8.94, p = 0.002), dilated cardiomyopathy (AHR = 8.26, 95% CI: 2.43–28.04, p = 0.001), gastrointestinal comorbidity (AHR = 8.57, 95% CI: 2.09–35.12, p = 0.003), atrial fibrillation (AHR = 3.50, 95% CI: 1.32–9.28, p = 0.01), and polypharmacy (AHR = 2.68, 95% CI: 1.11–6.46, p = 0.03) were significantly associated with reduced ED survival time (Table 6).
Table 6 Bivariate and multivariate COX regression analysisPrevalence of drug-related emergency admissionsThe study identified 125 DRPs in 92 patients, with an average of 1.36 DRPs per patient. The prevalence of DREA was 23%. Of the patients with drug-related admissions, 9.8% (n = 9) died.
Characteristics of drug-related emergency admissionsOf the 125 identified DREAs, 58.4% (n = 73) were attributed to non-adherence, 12.8% (n = 16) were ADRs, with hyperkalemia being the most common (31.2%). Drug-drug interactions (DDIs) were identified in 5.6% (n = 7) of patients, and inappropriate drug selection, indication, and dosing were found in 8.0%, 8.0%, and 7.2% of patients, respectively (Fig. 3).
Fig. 3
Types of DREAs identified
Among 73 non-adherent patients, the main reasons were treatment fatigue (27%), high medication cost (19%), perceived recovery (18%), lack of knowledge (14%), fear of side effects (11%), and forgetfulness (11%). These findings highlight both patient-related and system-related barriers to adherence.
Determinant factors affecting DREAsBivariate logistic regression analysis showed that age, education level, marital status, monthly income, smoking history, duration of CVD, tuberculosis (TB) comorbidity, electrolyte disturbance, and polypharmacy were associated with DREAs (p < 0.25). These variables were included in the multivariate logistic regression analysis. Multivariate analysis found that marital status, age < 18 years, longer duration of CVD, smoking history, and polypharmacy were significantly associated with DREA (p < 0.05). Smokers had a 2-fold increased risk of DREA compared to non-smokers (adjusted odds ratio [AOR] = 2.47, 95% CI: [1.07, 5.70], p = 0.034). Patients on polypharmacy had an 8-fold increased risk of DREA (AOR = 8.54, 95% CI: [3.73, 19.53], p < 0.001) (Table 7).
Table 7 Factors associated with DREA using bivariate and multivariate regression
Comments (0)