
Remember me



This expert opinion paper aimed to gather insights on the awareness, screening, and management of pDPN across the UK. These insights were derived from an advisory board meeting held on January 8, 2025. Chaired by Kevin Fernando (general practitioner [GP], East Lothian, Scotland), the meeting included six clinicians: five GPs and one lead diabetes specialist nurse (DSN) from different UK regions. Participants included Heather Bell (GP, Greenisland, Northern Ireland), Sarah Davies (GP, Cardiff, Wales), Kevin Fernando (GP, East Lothian, Scotland), Patrick Holmes (GP, County Durham, England), Beth Kelly (DSN, Wiltshire, England), and Samuel Seidu (GP, Leicester, England), all of whom are authors of this paper. The participants represented diverse perspectives informed by varying healthcare practices in England, Scotland, Wales, and Northern Ireland. Discussions during the virtual meeting focused on key areas such as pDPN awareness, current screening practices, and management challenges. Ethics committee approval was not required for this study. No patient data were discussed, and all participants provided consent to share their professional insights for this paper.
Consensus was achieved on all parameters through structured discussions among the expert panel. These discussions were guided by an analysis of clinical practice gaps and a collaborative evaluation of innovative care models across the UK. The findings and consensus reached during the discussions form the basis for this expert opinion paper.
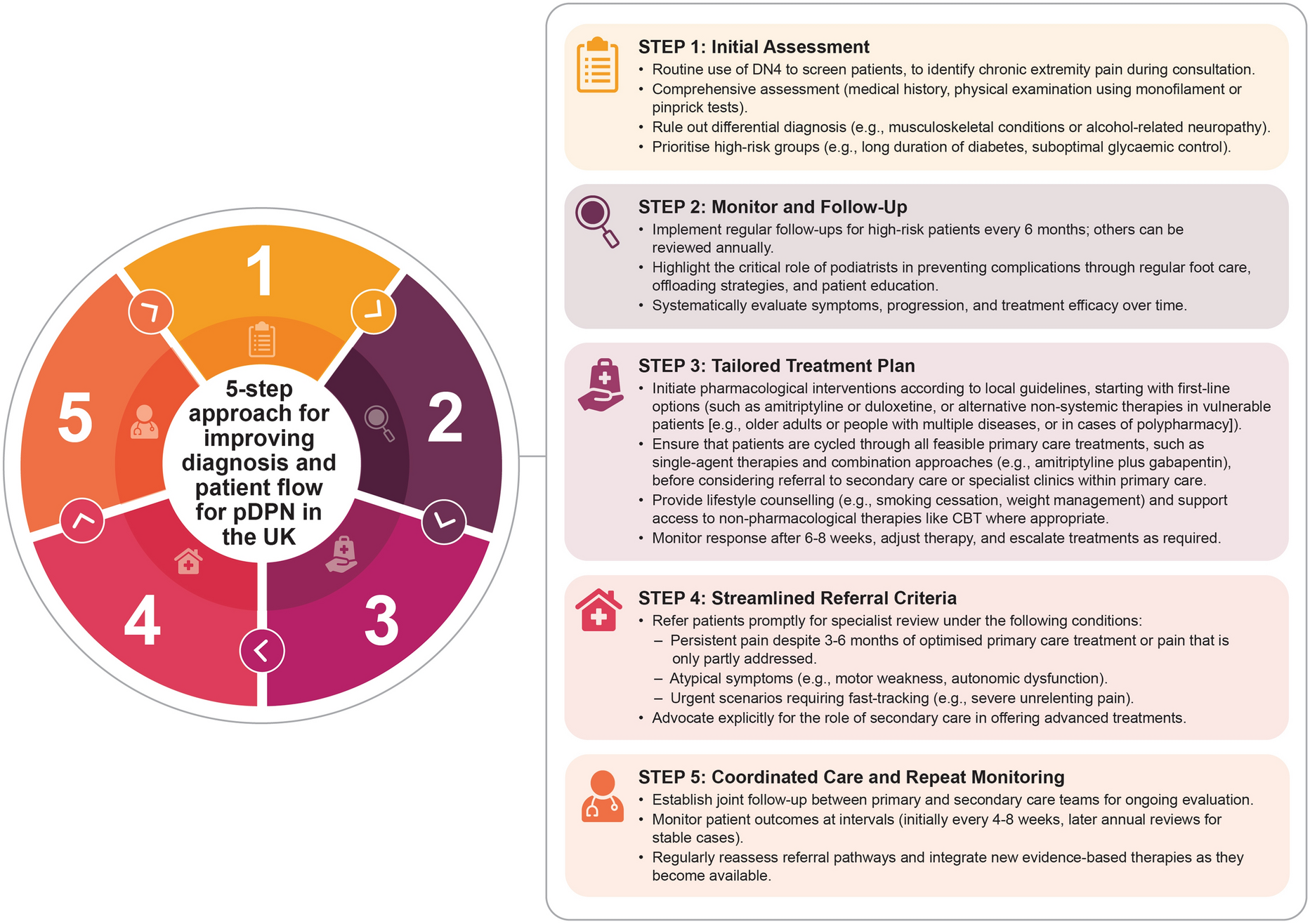
Current Challenges and Pragmatic SolutionsA consensus-based five-step algorithm (Fig. 1) was developed to improve diagnosis and optimise patient flow for pDPN in primary care. Table 1 summarises the challenges faced in UK primary care and practical solutions to strengthen pDPN care nationwide.
Fig. 1
Five-step pragmatic consensus for improving pDPN diagnosis and patient flow in UK primary care. Patients diagnosed with pDPN in step 1 should immediately move to step 3 to initiate treatment. High-risk patients may include individuals with poor HbA1c control, prolonged diabetes duration, advanced age, female gender, diabetic nephropathy, other diabetes-related complications (e.g. retinopathy), and contributing psychological or socioeconomic factors [21]. CBT cognitive behavioural therapy, DN4 Douleur Neuropathique 4 questionnaire, pDPN painful diabetic peripheral neuropathy
Table 1 Challenges and pragmatic solutions for improving pDPN care across the UKScreening and Diagnosis of pDPN in UK Primary CareScreening and diagnosing pDPN in UK primary care is challenging, leading to delays in early intervention and effective management. These challenges directly impact patient outcomes and contribute to disparities in care delivery across regions.
One major obstacle is the lack of awareness about pDPN among primary care HCPs. Many HCPs do not fully understand neuropathic pain, making it difficult to recognise early symptoms. This issue is exacerbated by time pressures in busy clinical environments, where thorough foot screening is often deprioritised. Although early detection is essential for effective management, it requires dedicated time and focus, resources that are typically in short supply in primary care.
Another challenge is the inconsistency of screening practices across the UK, driven by variations in clinical care models. There is ambiguity regarding who among HCPs—whether GPs, practice nurses (PNs), DSNs, practice/community pharmacists or healthcare assistants—should take responsibility for the screening, diagnosis, and initial management of pDPN. This lack of defined accountability has contributed to inconsistent assessments and suboptimal care for patients.
The underutilisation of diagnostic tools like monofilaments (Fig. 2) and validated questionnaires, such as the Douleur Neuropathique 4 (DN4) [22], is another barrier. These reliable tools are often absent from routine practices. However, incorporating practical steps, like having patients complete DN4 questionnaires electronically before their appointments or while waiting, could streamline initial assessments. Primary care screening can identify high-risk individuals, who can then be quickly referred to PNs, pharmacists, or GPs trained in pDPN for evaluation and treatment planning.
Fig. 2
Note: Although monofilaments are primarily used to predict diabetic foot ulcers, they also assess sensory loss, a key feature of pDPN. Theirinclusion helps evaluate sensory deficits, differentiating pDPN from other pain causes, and aligns with clinical guidelines as part of a broaderdiagnostic strategy for peripheral neuropathy [26]
Monofilament test for neuropathic pain. Adapted from Richardson CR et al. (2021) with permission [34] (released under CreativeCommons Attribution-NonCommercial-ShareAlike 4.0 International License (CC BY-NC-SA 4.0))
Annual diabetes reviews offer an ideal opportunity to standardise screening practices. By integrating consistent workflows during these reviews, podiatrists, nurses, or healthcare assistants (HCAs) could lead the process, tailored to the specific resources and needs of each practice. This would help ensure screening remains practical and reliable across various primary care settings.
Despite the availability of resources such as NHS diabetes modules and initiatives such as Think Diabetes, their potential remains underutilised [23]. Increased adoption of these frameworks could promote more uniform practices and bridge care gaps across regions. Socioeconomic barriers, such as transportation costs to and from appointments, further hinder patients’ access to timely care, exacerbating the uneven distribution of services.
Addressing these challenges requires a multifaceted approach. This includes targeted training programmes for HCPs to enhance their understanding of pDPN, wider integration of validated and accessible screening tools, and patient-centred workflows tailored to local needs. Tackling these issues systematically will enable primary care providers to improve early identification of pDPN, ensuring people with pDPN receive timely and effective management.
Treatment and Referral Pathways for pDPN in UK Primary CareManaging pDPN presents significant challenges, primarily due to variations in regional treatment guidelines within the UK. These guidelines often conflict with evidence-based global recommendations that endorse combination therapies and advanced treatments such as capsaicin 179 mg cutaneous patch [16, 24]. Recent Neuropathic Pain Special Interest Group guidelines (2025) now recommend that the locally applied capsaicin 179 mg cutaneous patch can be considered early in the pathway for vulnerable patients (e.g. older adults or people with multiple diseases, or in cases of polypharmacy) [25].
Meanwhile, NICE guidelines, though highly regarded, adopt a more conservative stance [20, 26]. This cautious approach limits access to advanced treatment options and provides minimal guidance on combination therapies, leaving primary care HCPs without clear direction. Consequently, treatment inconsistencies and suboptimal care persist across regions. Evidence suggests that clinical guidelines can significantly impact patient care by influencing treatment decisions and access to therapies [27, 28]. However, rigid adherence to conservative guidelines may inadvertently restrict the use of innovative treatments, leading to delayed or suboptimal outcomes for patients [27, 28].
Further complicating matters, restrictions on therapies and the limited endorsement of combination approaches undermine effective management [10]. Local guidance in certain areas has specifically moved to disincentivise the use of gabapentinoids, such as pregabalin and gabapentin, because of significant concerns about risks of dependence, misuse, and diversion [29]. These drugs were reclassified as schedule 3 controlled substances on 1 April 2019 in Northern Ireland [29]. While these measures aim to mitigate harm, they add complexity to prescribing practices, making it more challenging for HCPs in primary care to deliver comprehensive and tailored solutions to patients.
Moreover, clinician compensation structures add another barrier to effective management. Incentive schemes, such as the Quality Outcomes Framework (QOF) and Pay for Performance (P4P) programmes, prioritise achieving predetermined clinical outcomes, often at the expense of non-incentivised activities, including holistic pDPN care [30, 31]. This checklist-driven focus on measurable targets can undermine patient-centred management and worsen inconsistencies in treatment quality and access [30, 31].
For people with pDPN, the road to effective management is often lengthy and frustrating. Current treatment pathways rely heavily on first-line therapies, including pharmacological treatments, lifestyle modifications, and non-pharmacological interventions. Even at the secondary care level, access to advanced treatments remains limited, further worsening outcomes. Introducing advanced therapies into primary care settings could dramatically improve this process. Streamlining access to these options could spare patients lengthy trial-and-error cycles and enable tailored, timely care.
Referral pathways add another layer of complexity, as primary care HCPs often face uncertainty about when, how, and to whom they should escalate cases requiring specialised care, such as neurologists or pain management teams, which may be further limited by availability of appointments. The timing of referrals to specialists is often inconsistent and delayed, potentially leading to significant or rapid deterioration in the patient’s condition. This ambiguity delays access to expert care and leads to underutilised specialist pathways. Fragmented communication between primary and secondary care compounds these issues, leaving patients caught in cycles of inadequate management.
Adding to this challenge is the lack of support for continuing professional development (CPD) training. Many primary care HCPs feel underprepared for managing the complexities of pDPN as a result of limited time and resources for ongoing education. Without up-to-date knowledge of emerging treatments and best practices, HCPs are at a disadvantage.
Addressing these challenges requires a multifaceted approach. Reducing regional disparities in treatment guidelines is a critical first step. Aligning UK practices with global, evidence-based recommendations will foster consistent, advanced care for patients. This may include revisiting NICE guidelines to integrate advanced therapies and clarify combination treatments [20]. Clearer referral criteria must also be established. Defining when and how to escalate cases to specialists can reduce delays and ensure timely, appropriate care. Additionally, stronger communication frameworks between primary and secondary care can enhance coordination and make referral pathways more efficient. Lastly, significant investment in CPD opportunities is vital. Equipping primary care HCPs with updated knowledge on treatments and management strategies will enhance their confidence and ability to handle pDPN effectively.
By addressing these barriers systematically, the UK primary care system can improve treatment consistency, streamline referrals, and ultimately enhance patient outcomes in managing pDPN.
Innovative Approaches to MDT IntegrationIntegrating multidisciplinary teams (MDTs) in primary care ensures comprehensive and coordinated care for people with diabetes. These teams typically include GPs, nurses, practice/community pharmacists, podiatrists, and diabetes specialists [20, 35]. Several innovative care models highlight the potential of MDTs in improving pDPN care. One notable example is the use of retinal screening clinics as dual-purpose appointments. These clinics combine eye examinations with foot checks, addressing multiple diabetes-related complications in a single visit. This approach not only improves efficiency but also reduces the burden on patients while increasing diagnostic opportunities. Another promising initiative is embedding community podiatrists or community diabetes nurse specialist teams within primary care practices [36]. This model fosters closer collaboration between primary care HCPs and community specialists, enhances patient accessibility, and facilitates seamless sharing of expertise [36]. Additionally, the Sheffield One-Stop Microvascular Screening Service demonstrates the feasibility and effectiveness of a holistic approach to annual diabetes health checks [37]. By integrating modern point-of-care devices to diagnose DPN and other complications early, this model not only improves screening uptake but also enables timely management, reducing the risk of severe outcomes [37].
Addressing Systemic Barriers to Collaborative CareDespite its potential, several systemic barriers hinder effective MDT integration in pDPN care [15, 38, 39]. Key challenges include insufficient funding for the recruitment and training of MDT members, as well as limited resources to support collaborative care. These gaps restrict the broader implementation of MDT-based models [15]. Additionally, variations in referral criteria and processes across regions lead to delays, miscommunication, and fragmented person-centred care [40].
High workloads for primary care HCPs, coupled with inconsistent support for CPD, further limit their ability to engage fully with MDT initiatives [39, 41, 42]. Overcoming these issues requires continued investment in multidisciplinary care frameworks, standardising referral pathways, and increasing funding to bolster MDT collaboration. Building on successful examples, like dual-purpose screening clinics and in-house specialist integration, can offer scalable models for wider adoption. By prioritising MDT integration, primary care systems can enable earlier diagnosis, patient-centred care, and the prevention of complications, ultimately delivering a more cohesive and effective approach to pDPN management.
Case Examples: How to Improve Patient Flow in pDPN Primary Care Using the Five-Step ApproachPatient cases provide valuable insights into the challenges and opportunities of managing pDPN in UK primary care. The following fictitious scenarios highlight common issues, such as missed diagnoses, ineffective treatment strategies, and the impact of excluding MDTs. These examples also demonstrate the practical application of improved workflows using the five-step pragmatic consensus approach. By integrating case-driven workflows, such as standardised screenings, combination therapies, and MDT collaboration, primary care MDTs can significantly enhance pDPN care, ultimately improving patient outcomes.
Case 1: Missed diagnosis leading to complications
Patient profile: Male, 58 years old, living with type 2 diabetes for 12 years. Complaints of intermittent pain and tingling in feet; thought to be ‘age-related’ by GP, who prescribed a standard painkiller
Key challenges: This patient’s symptoms were missed during multiple annual diabetes reviews as a result of a lack of standardised screening protocols in the clinic. No formal neuropathic pain assessment tool, such as the DN4, was utilised. By the time of diagnosis, the patient had developed foot ulcers, significantly impacting his daily life
Intervention and workflow improvement: A new practice workflow was implemented, mandating DN4 questionnaires for all patients with diabetes during annual reviews. This flagged similar symptoms in newly presenting patients, enabling earlier diagnosis and timely management. The clinic also introduced regular podiatrist visits to monitor foot health and provide preventive care
Outcome: Standardised screenings reduced the rate of delayed diagnoses, and the patient showed improved outcomes with a tailored combination of pregabalin for neuropathic pain and wound care provided by the podiatry team
Case 2: Effective treatment combinations
Patient profile: Female, 65 years old, living with type 1 diabetes since age 25. Diagnosed with pDPN several years ago but discontinued single-drug therapy because of side effects
Key challenges: Treatment was delayed as a result of reliance on overly conservative guidelines, with limited options discussed during primary care consultations. A fragmented system made access to advanced treatments challenging within her region
Intervention and workflow improvement: A diabetes specialist nurse in the region introduced combination therapy protocols, working closely with primary care providers. The patient was prescribed a complementary regimen of duloxetine and pregabalin, which reduced her pain significantly with manageable side effects. Regular follow-ups and patient input guided adjustments to the treatment plan
Outcome: The patient experienced a substantial improvement in quality of life and was able to resume daily activities with minimal disruptions. The clinic also adopted a streamlined treatment pathway to ensure similar cases received timely access to advanced therapies
Case 3: Escalation to secondary care with capsaicin 179 mg cutaneous patch
Patient profile: Male, 54 years old, living with type 2 diabetes for 15 years. Initially managed with first-line treatments, but pain persisted as a result of suboptimal symptom control
Key challenges: Despite early identification of pDPN, the patient’s pain management was inadequate with multiple different oral therapies such as gabapentin, many of which he struggled to tolerate as a result of side effects. Secondary issues, including suboptimal glycaemic control, exacerbated neuropathy, leading to foot complications
Intervention and workflow improvement: The patient was referred to a secondary care pain management clinic, where he was evaluated for advanced therapies. After a thorough assessment, he was treated with capsaicin 179 mg cutaneous patch to target localised neuropathic pain. This locally applied treatment was particularly suitable given the patient’s vulnerability due to polypharmacy and intolerance to systemic therapies [25]. The patch provided sustained relief by desensitising overactive pain fibres, while the secondary care team collaborated with podiatrists. The patient was also placed on an ongoing treatment plan, with regular reviews to monitor efficacy and adjust the course of therapy as needed
Outcome: The patient achieved significant pain relief, with fewer episodes of breakthrough pain. Ongoing collaboration between secondary care specialists, the patient’s GP, and a podiatrist ensured consistent follow-up care. Educational sessions also improved the patient’s understanding of diabetes management, reducing the risk of further complications
Case 4: Successful MDT intervention enhancing care
Patient profile: Male, 52 years old, newly diagnosed with diabetes and experiencing neuropathic symptoms
Key challenges: The patient’s local healthcare setup lacked integration among primary care providers, podiatrists, and diabetes specialists. The patient’s neuropathic pain management and diabetes care were delayed, increasing the risk of complications
Intervention and workflow improvement: The region piloted a collaborative model where retinal screening clinics also included pDPN assessments and foot checks. This model identified the patient’s pDPN early. A podiatrist immediately addressed his foot health needs, while a diabetes specialist nurse adjusted his management plan to include neuropathic treatment
Outcome: The integrated system facilitated early diagnosis, ensured timely referrals, and provided coordinated long-term care. This proactive approach reduced the patient’s risk of ulcers and other severe complications
The current study is based on expert opinions and consensus derived from a small group of healthcare professionals, which may not comprehensively reflect the diversity of clinical practices or patient experiences across the UK. Furthermore, while the proposed five-step framework offers a structured approach to improving pDPN care, further research is essential to validate its effectiveness and assess its real-world impact on patient outcomes in varied healthcare settings.
Comments (0)