Study Characteristics
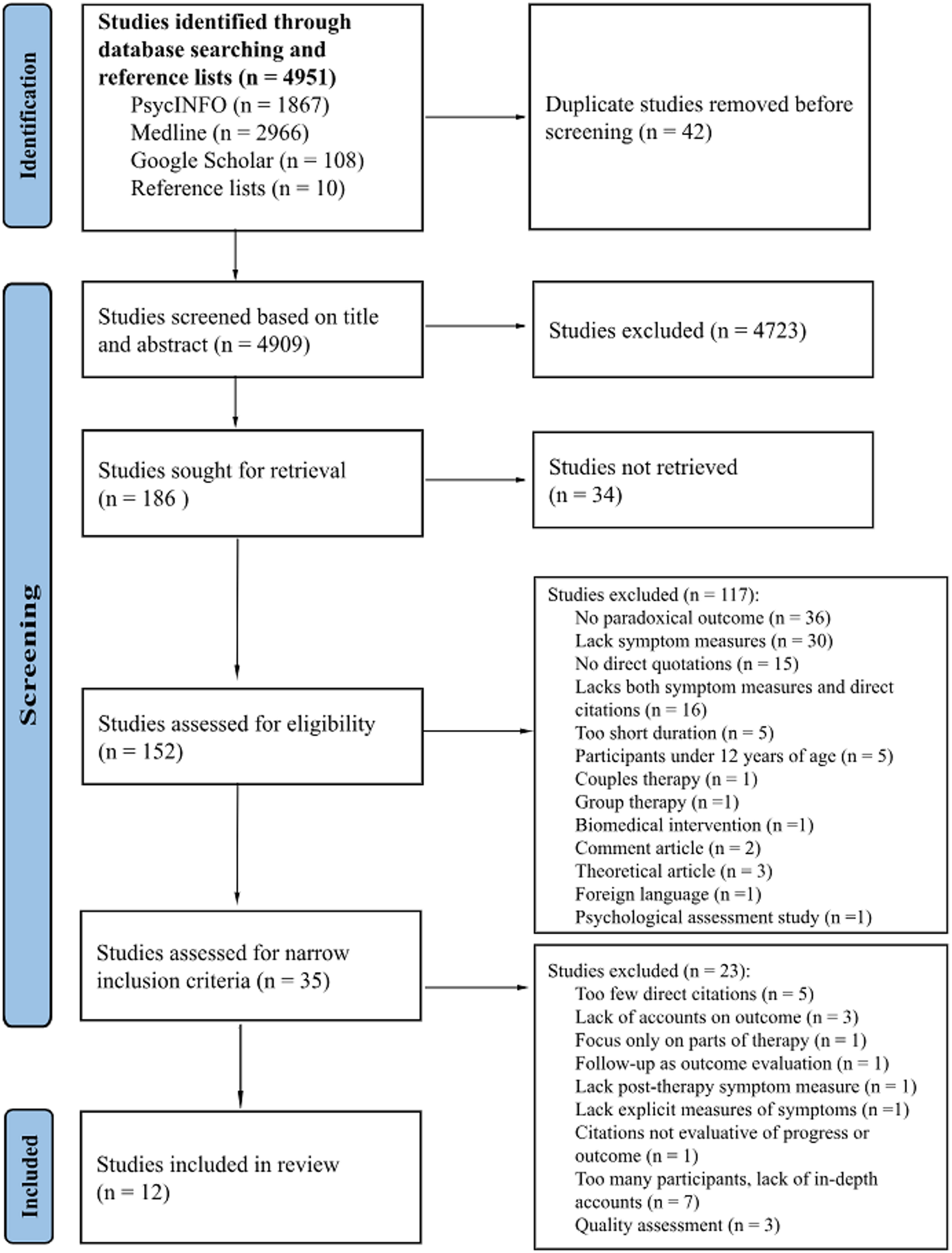
Twelve case studies published between 2011 and 2024 were included, comprising 17 patients in total, though one patient was excluded due to lack of paradoxical outcome and short treatment length. The studies were conducted in Norway (n = 3), Czech Republic (n = 1), Ireland (n = 1), Belgium (n = 3), England (n = 1), Italy (n = 1), Australia (n = 1), and Argentina (n = 1). Therapy modalities included art-based, pluralistic, psychoanalytic, psychodynamic, mentalization-based, cognitive analytic, supportive-expressive, cognitive-behavioral, cognitive-integrative, and transactional analytic therapy. Participants were aged 17–55, mostly women (14) with two men. Therapy duration spanned from 12 to 121 sessions. Quantitative outcomes varied: no change (n = 2), deterioration (n = 1), improvement (n = 5) or mixed results (n = 4).
Thematic Synthesis
The synthesis included two analyses, resulting in three meta-themes with 14 subthemes in the first analysis, and one meta-theme with three subthemes in the second. Quotes are from researchers (R), therapists (T), and patients (P). For transparency, the number of studies per theme is included (n = #).
First Analysis: the Types of Paradoxical Outcomes
The first analysis reflects different changes and processes that occurred throughout therapy in light of their quantitative results, thus producing paradoxical outcomes.
Meta-Theme: False Improvement
This theme represents nine patients (Ela, Megan, Jason, Sophia, Rebecca, Paula, Rita, Penelope, Sandra) (n = 6) who showed symptomatic improvement on self-reports while simultaneously indicating negative outcomes.
Patients Were Disappointed or Uncomfortable To Change (n = 5)
Six patients were disappointed or uncomfortable with therapy. Some prematurely dropped out due to wanting more advice, guidance, or deeper explorations (De Smet et al., 2021; Dolezal et al., 2019; Meier et al., 2023). Another patient, Ela, dropped out as therapy had fulfilled its purpose, and avoided talking deeper about her relationships: R: “She was uncomfortable with the realization of how much her life was determined by her parents’ wishes” (Dolezal et al., 2019, p. 156). Similarly, Megan’s therapist interpreted her drop-out as a fear of dependency: T: “I think that’s the really hard thing, to know that … you might need somebody else to kind of work things out a bit” (Meier et al., 2023, p. 404).
No Deeper Change – Having Remaining Issues (n = 6)
Nine patients worsened at follow-up, had remaining issues, uninternalized insights, or inconsistent changes. For instance, despite Penelope improving symptomatically, she stated: P: “I cannot quantify how much my problems are changed … I mean, my entire problems are still there … “(Benelli et al., 2016, p. 30). Similarly, Ela’s therapist considered her improvement as: T: “… premature, unintegrated, and prone to a relapse” (Dolezal et al., 2019, p. 156). While some worsened at follow-up (Benelli et al., 2016; De Smet et al., 2021), Sandra had increased work difficulties following exposure therapy, relating this to her perfectionism (Gomez et al., 2022).
Process: Misunderstandings and Disagreements (n = 5)
Five patients had difficulties in the therapeutic relationship. Such strains were patients feeling pushed or insufficiently challenged by the therapist, and the absence of shared understanding and limited agency: R: “Both Paula and Rebecca seemed mainly displeased with the therapists but did not share this with them” (De Smet et al., 2021, p. 168). In Megan’s case, the therapist became more challenging, while Megan became more rejective. Sandra, on the other hand, worsened after exposure training, where the therapist might have failed to address adverse treatment effects (Gomez et al., 2022).
Process: Patient Avoidance and Struggles (n = 4)
Four patients struggled with difficult topics, manifesting as not talking (Dolezal et al., 2019; Meier et al., 2023), using humor or superficial compliance (Gersh et al., 2017), passiveness (Dolezal et al., 2019) or criticism to one’s progress (Benelli et al., 2016). In Ela and Megan’s case, their core relational patterns of vulnerability manifested, leading to strains by pulling the therapist into unusual actions. The therapists then became inpatient (Dolezal et al., 2019), or increasingly challenging (Meier et al., 2023). Ela’s therapist said: T: “It [her feelings] wasn’t coming, so I began to feel annoyed, as I was struggling to find a way to work with this” (Dolezal et al., 2019, p. 158).
Meta-Theme: False Worsening
Five patients (Maria, Lisa, Mark, Ria, J.J) (n = 4) paradoxically deteriorated on self-reports but expressed satisfaction with therapy and showed other positive changes.
More Self-Understanding (n = 4)
Five patients experienced increased self-awareness. Some shifted from a somatic to a psychological understanding of their issues (Gullestad & Wilberg, 2011; Thoresen et al., 2021). J.J described how therapy led to an awareness that she cannot change other people: P: “ I am trying to learn to accept things now. That things just are what they are; they are not going to change; I can only change myself” (Ward & McLeod, 2021, p. 217).
Becoming Agentic (n = 4)
Four patients reported increased agency, manifesting in diverse ways: increased energy to face challenges (Thoresen et al., 2021), improving communication, entering a loving relationship (Ward & McLeod, 2021), and obtaining employment (De Smet et al., 2024). Additionally, Maria achieved autonomy through independent working and living (Gullestad & Wilberg, 2011).
Changing Stance Towards Symptoms (n = 4)
Four patients gained a more flexible attitude towards their distress. Lisa became able to eat with friends, and her mother remarked on positive changes: P: “It is so nice to get a comment like that … that comments on the symptoms of the eating disorder, so it might have had an effect on me without me noticing” (Thoresen et al., 2021, p. 191).
Other patients became more able to cope by increased reflection (Gullestad & Wilberg, 2011), insight (Ward & McLeod, 2021), or reframing distress as necessary (De Smet et al., 2024).
Process: Helpful Therapeutic Activities (n = 4, Four patients)
Helpful therapists actively facilitated exploration by constructing timelines (Ward & McLeod, 2021), using directive questions (Gullestad & Wilberg, 2011), facilitating dialogue between inner voices (Thoresen et al., 2021), or providing feedback that reframed perspectives (De Smet et al., 2024). Two cases explored emotions through drawing and using toy figures, described as helpful for J.J: P: “I don’t know … why I drew an eye. It was so emotional; it was probably one of the best sessions I ever had” (Ward & McLeod, 2021, p. 216).
Process: Necessary Difficult (n = 4)
Five patients reported bringing up painful memories and affects as necessary, involving them to step out of their “comfort zone” (Ward & McLeod, 2021, p. 216) and open up about vulnerability (Thoresen et al., 2021). Similarly, Ria expressed that worsening was essential: P: “(…) I believe I really have to experience this now in order to slowly crawl back up again” (De Smet et al., 2024, p. 8). Despite feeling scared, Maria experienced a broader range of emotions and recalled more positive memories (Gullestad & Wilberg, 2011).
Meta-theme: Invisible Changes – Positive or Negative
This analytic theme represents two cases that had no clinically reliable change on symptom inventories but showed changes indicating improvement, stabilization or deterioration.
Increased Distress (n = 2)
Both patients worsened with either increased epileptic seizures (Van Nieuwenhove et al., 2020) or suicidal behavior (Halvorsen et al., 2016) After disclosing about fear of rejection, Cora cancelled a session, which the therapist interpreted as being on track: T: “About owning oneself. I think she is back on the field in her own process” (Halvorsen et al., 2016, p. 172). Pam’s depression eventually stabilized, and she remained ambivalent to treatment and reluctant to delve into her family relationship (Van Nieuwenhove et al., 2020).
Understanding Self and Others (n = 2)
Both patients changed in self-understanding, reflecting on how earlier relationships impacted them. Cora, who experienced childhood abuse, worked to understand her mother’s intentions and her own emotions: T: “To make connections between affects and what has happened previously in her life. There are good reasons for feeling anger, anxiety and sorrow. She showed a growing understanding of her own affective reactions” (Halvorsen et al., 2016, p. 173). Pam increasingly articulated wishes towards others: R: “Whereas before, her wishes were formulated in terms of wanting to avoid the negative anticipated reactions of others, she now seems to articulate her own desire, stemming from what she misses in relation to others” (Van Nieuwenhove et al., 2020, p. 369).
Exploring, Tolerating and Expressing Emotions (n = 2)
By the end of therapy, Cora exhibited a better tolerance of distress by not becoming as overwhelmed as before (Halvorsen et al., 2016), and frequently explored difficult topics:
P: Well, it is clear that when I look back, I have … achieved some very big changes. (…) I also have the right to … (inhales) rejoice at things … without immediately feeling guilty about it or put it aside. (Halvorsen et al., 2016, p. 173)
Pam remained ambivalent, interpreted as difficulty in connecting her suffering to trauma, but wanted to open up: P: “It is always tough to let other people in. I want to change that and start confiding in my sister more” (Van Nieuwenhove et al., 2020, p. 372).
Process: Helpful and Facilitating Aspects (n = 2)
Exploration of past experiences, identifying treatment goals, resolving internal conflicts, and engaging in distressing topics facilitated change for both patients. This involved exploring the patients’ wishes, defenses, and forbidden feelings (Halvorsen et al., 2016) or showing a validating stance during stress (Van Nieuwenhove et al., 2020). Cora experienced this as facilitating to building trust: P: “For me, it was essential that he accepted my ultimatum and my right to kill myself” (Halvorsen et al., 2016, p. 177).
Process: Strains and struggles – Dare to Do the Dishes (n = 2)
Both patients described relational difficulties, marked by struggles to open up or to maintain control. The fear of rejection from the therapist may have acted as a barrier to change. Cora stated:
P: I realize that I have to open those rooms and to clear up in there. Yes, that has been very hard. It goes so slowly. And then earlier this spring I decided that now … I have to dare … to do the dishes. (Halvorsen et al., 2016, p. 171)
In Pam’s case, the therapist decided not to address topics in therapy that could worsen her, such as her family relationship. Consequently, her relational patterns “slipped into” therapy (Van Nieuwenhove et al., 2020, p. 377) causing a shared avoidance, leading her to remain unaware of her pattern of distrustfulness towards others.
Second Analysis: Researchers’ Interpretations of Paradoxical Outcomes
One meta-theme and three subthemes were identified across cases that showed how the researchers attempted to explain the contradictions.
Meta-theme: the Uncaptured Aspects of Psychotherapy Outcomes
This meta-theme (n = 12) reflects aspects not captured by quantitative measures, questioning validity of outcome assessments, and showing that self-reports assessments were shaped by personality and situational factors.
Questioning the Validity (n = 9)
Several researchers reported that self-reports were often not sensitive enough to capture critical changes, raising questions regarding validity. Two studies highlighted missed improvements, such as reduced self-harm and increased affect awareness (Halvorsen et al., 2016; Thoresen et al., 2021), while one study showed how global scores could mask remaining difficulties (Gullestad & Wilberg, 2011). Three studies focused on how the patient’s latent need for control, or actual severity of distress were not addressed by the assessments (Benelli et al., 2016; De Smet et al., 2021; Ward & McLeod, 2021).
The Influence of Social Context (n = 8)
Outcomes can occur because of situational aspects and social dynamics. Researchers discussed whether patients underreported their distress (Dolezal et al., 2019; Ward & McLeod, 2021) to please the therapist, due to a lack of agency (De Smet et al., 2021), or to give an impression of treatment success (Gomez et al., 2022). Paradoxical outcome was also thought to occur because the therapist minimized disappointing self-report scores (Halvorsen et al., 2016). Other factors were getting a romantic partner (Benelli et al., 2016), work issues or school exams (Dolezal et al., 2019; Gomez et al., 2022), or the timing of the assessments, reporting different outcomes during therapy and at follow-up (De Smet et al., 2021).
The Effects of Inner Changes (n = 10)
Researchers explained the discrepancies in relation to patients’ personality dispositions. One patient had no change in alliance ratings, but expressed trust towards the therapist in an interview, which was interpreted as the patient’s core relational issue of distrust (Halvorsen et al., 2016). In another study, researchers proposed that the patient’s perfectionism influenced her work functioning, leading to worsening OCD symptoms (Gomez et al., 2022).
Four articles explained paradoxical outcomes as resulting from illusory mental health. Patients’ underlying issues influenced how outcomes manifested, initially presenting themselves as emotionally well-adjusted, minimizing or denying distress by underreporting (e.g., Gullestad & Wilberg, 2011; Benelli et al., 2016; Ward & McLeod, 2021; Thoresen et al., 2021). Worsening was thus described as progress toward greater authenticity: R: “The scales might assess defensiveness rather than health. The result of a successful psychotherapy could then be to raise scores on measures of distress, at least temporarily” (Gullestad & Wilberg, 2011, p. 108).





Comments (0)