Through our study, we aimed to identify non-invasive predictors of variceal etiology in patients with UGIH presenting to ED. We found that spleen diameter on POCUS, PC/SD ratio, PT, and PVFV could help us rapidly identify patients with variceal hemorrhage and initiate appropriate management with vasoactive agents, antibiotics and timely endoscopy. Additionally, fibrosis scores, which are traditionally used for identifying advanced liver disease in patients, were also found to be useful in patients with UGIH to predict variceal etiology. The newly developed SCoPE score, integrating spleen diameter, PT, and PVFV, showed strong predictive ability for identifying variceal etiology in UGIH. With an AUC of 0.843 and an overall diagnostic accuracy of 78.2%, the score provides a simple, ED-applicable tool for early risk stratification.
In our patient population, esophageal varices (58.6%) were the most common cause of UGIH, followed by Peptic Ulcer disease (25.97%). In previous decades, UGIH was the most frequently attributed to peptic ulcer disease [1, 12]. However, with the widespread use of proton pump inhibitors and H2 receptor antagonists for treatment and prophylaxis of peptic ulcers, there has been a notable shift in the etiology of UGIH. Recent studies suggest that variceal bleeding may have become the predominant cause of UGIH [2, 3, 13], although regional variations may exist [1]. Variceal UGIH has a higher mortality than peptic ulcer disease-related bleed [2, 13], highlighting the need for prompt recognition and swift management.
Moreover, variceal hemorrhage requires tailored treatment, including vasoactive agents, such as somatostatin analogs, antibiotic administration, and early endoscopic management. However, often there is a delay in the diagnosis of the variceal etiology of UGIH due to a delay in endoscopy [5]. Recent 2024 guidance document from the AASLD emphasizes the role of non-invasive assessment in the risk stratification of portal hypertension and varices, using liver stiffness measurement and platelet count to identify clinically significant portal hypertension, in alignment with the Baveno VII consensus [4]. However, liver stiffness measurement requires patient stability, fasting, and dedicated equipment. Immediate availability of transient elastography to assess liver stiffness in the ED when a patient comes with UGIH is a challenge. POCUS-based parameters and composite scores such as SCoPE score offer a pragmatic alternative in an actively bleeding patient, especially when the diagnosis of CLD is uncertain. POCUS can be performed immediately at the bedside during active resuscitation, and hence can be a complementary addition to the algorithm, in patients with UGIH.
Among the studied POCUS parameters, spleen diameter had the highest AUC of 0.808 for predicting variceal etiology. We assessed the spleen diameter using POCUS, as previous studies have emphasized addition of POCUS to traditional physical examination improves the diagnostic accuracy of detecting splenomegaly [14]. In patients with liver cirrhosis, spleen size has been found to be a predictor of varices [8, 15,16,17,18]. Various cut-offs considered in these studies have been summarized in the supplementary table 7. As our study population was UGIH, we found that spleen length > 12 cm, which is consistent with splenomegaly cut-off, would be appropriate for identifying varices.
Our study found that thrombocytopenia supported the diagnosis of variceal etiology of UGIH. Although 25.4% of our study participants had history of antiplatelet use, this may not directly decrease the platelet count and needs to be assessed using platelet function studies. Additionally, PC/SD ratio was a useful predictor for the cause of UGIH, as well as could reliably predict presence of large varices. Among the patients with CLD, previous studies have found platelet count to be a useful hematologic marker to predict presence of varices [6, 18, 19]. Combining the platelet count with the spleen diameter considers two significant predictors to form a useful ratio, which can help in our rapid decision-making at the ED, which was also underlined in the previous studies by Nouh et al. and Cherian et al. [8, 20,21,22]. Although the focus of earlier studies have been on patients with CLD, we find platelet count and PC/SD ratio to be important markers in UGIH patients, which can inform treatment strategies, rendering them an essential tool in clinical practice.
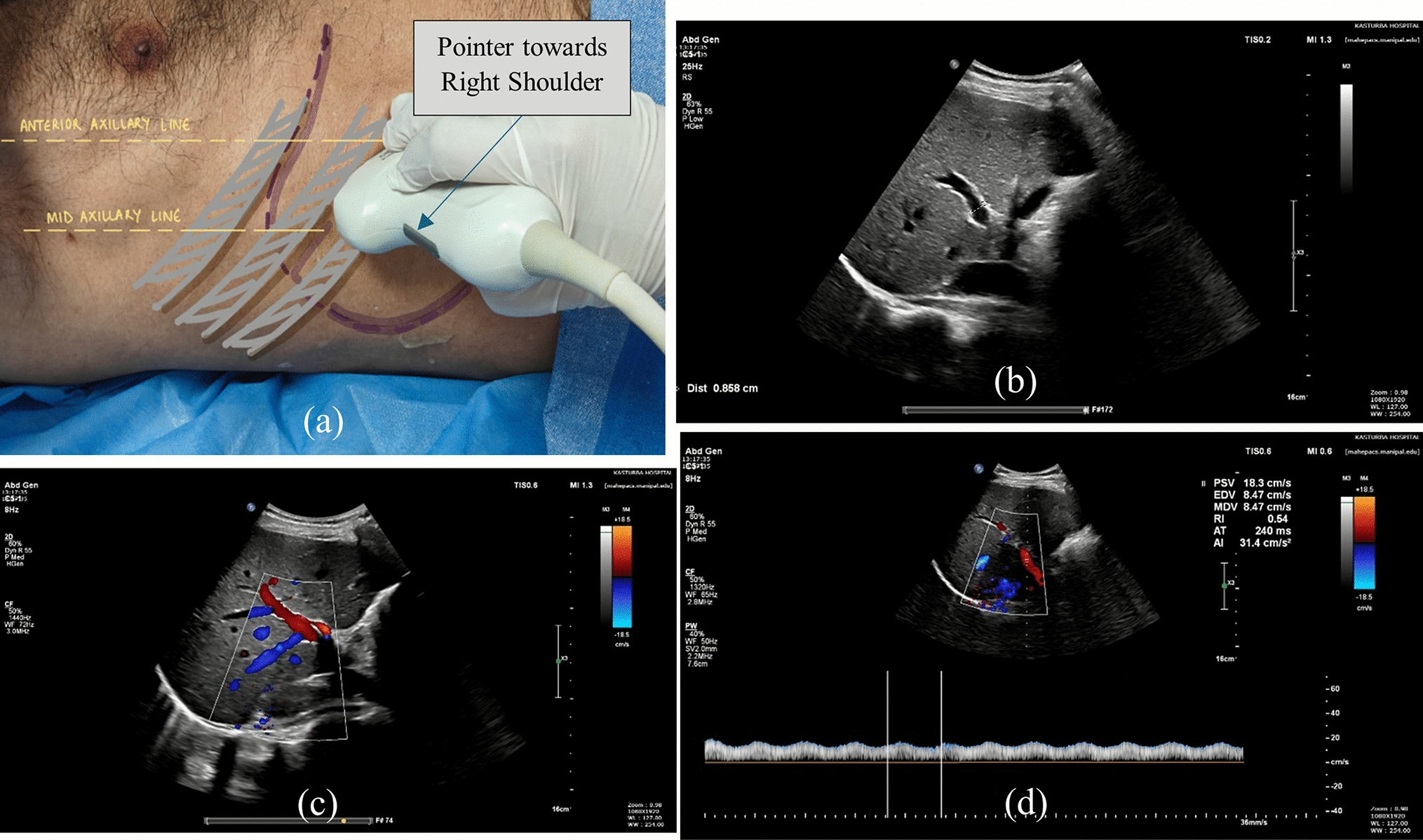
Portal hypertension causes a reduction in PVFV, which was found to be a useful portal vein index to differentiate variceal from non-variceal cause of UGIH, as well as predict large varices, in our study. Ultrasound done in the radiology suite, in CLD patients has been previously used to predict varices [6, 7, 10, 16, 20, 23, 24]. We found that bedside PVFV, done by the emergency physician, in an active UGIH patient was useful in etiology identification in the ED.
Other portal vein indices, such as PVD [7, 8, 15,16,17, 20, 23] and PCI [7, 20, 23], have also been used in CLD patients without active bleeding as varices predictor. On multivariate logistic regression analysis, we did not find a significant association between these parameters and varices in our patients. However, PCI was found to be a significant parameter for predicting grade of varices. Active hemorrhage, unstable hemodynamics, and ongoing resuscitation may impact the PVD, which needs to be studied further.
Variceal hemorrhage is a well-recognized and frequent complication of chronic liver disease, and our findings reaffirm this, with prior CLD showing a strong association with the presence of varices (Cramer’s V = 0.612). Clinically, this supports the principle that any patient with CLD presenting with UGIH should be treated as variceal until proven otherwise, with early initiation of vasoactive agents, antibiotics, and timely endoscopy. However, a substantial proportion of patients present to the ED with UGIH without a prior diagnosis of CLD, and in these individuals, the variceal etiology may not be immediately apparent. In this subgroup as well, spleen diameter, PT, PC/SD ratio and PVFV showed good discriminatory performance, highlighting their value in identifying previously unrecognized portal hypertension.
Among patients with known CLD, while the majority had variceal bleeding, not all UGIH was variceal. In this subgroup, spleen diameter and PVFV remained useful markers for distinguishing variceal from non-variceal sources, underscoring the clinical utility of POCUS-based hemodynamic assessment even when CLD status is already known. These POCUS parameters were particularly useful in patients with Child–Pugh Class A and B.
Fibrosis scores are predictive models developed to assess the likelihood of liver cirrhosis and severe disease based on laboratory markers. Patients with advanced CLD, are likely to have portal hypertension complications. Hence, these scores have been used to predict presence of varices and need for UGI endoscopy in CLD patients [9, 23, 25,26,27,28]. We found these scoring systems, namely AAR, APRI, FIB-4, King, and Lok scores, when used in UGIH patients had AUC > 0.7 for predicting varices. Civan et al. used APRI score to predict varices among patients presenting to the emergency department with UGIH. By applying this retrospectively to their cohort, they determined that adherence to established guidelines for administering octreotide and antibiotics would have increased from 56 to 91% if the APRI score had been utilized [5].
FIB-4 is one of the most widely validated non-invasive fibrosis scores and is routinely used to stratify the severity of chronic liver disease, with established thresholds of < 1.3 for ruling out and > 2.67 for ruling in advanced fibrosis [29]. Because it relies solely on laboratory parameters available early in the ED work-up, such as AST, ALT, and platelet count, FIB-4 can be calculated at presentation and may assist clinicians in recognizing previously undiagnosed liver disease. This is clinically important because a significant proportion of patients with variceal hemorrhage present without a documented diagnosis of CLD, and early identification of portal hypertension may influence timely interventions. Several previous studies have evaluated cut-offs for FIB-4 scores in predicting varices and although thresholds vary across cohorts (from 2.8 to 6.4), higher fibrosis scores consistently correlate with advanced portal hypertension and increased likelihood of varices [9, 26, 28]. The cut-offs for the various studied parameters and fibrosis scores are compiled in the supplementary material (Supplementary Tables 7 and 8).
Although fibrosis scores were useful in predicting variceal etiology in our UGIH cohort, the SCoPE score demonstrated superior discriminatory ability, with an AUC of 0.843. This is likely because SCoPE incorporates POCUS-derived spleen diameter and PVFV—parameters that directly reflect the hemodynamic physiology of portal hypertension—while fibrosis scores primarily capture hepatic dysfunction rather than portal flow dynamics.
Our research steps into a newer realm of POCUS by ED physicians and highlights the use of portal vein indices in guided management of UGIH. Additionally, laboratory markers and fibrosis scores could be useful adjuncts. The novel SCoPE score could be an important tool for ED physicians to identify variceal bleeds. Further research would be needed to standardize protocols and establish robust predictive models for variceal etiology of UGIH.
Limitations
Inter-observer variability is a challenge in POCUS-based assessment, particularly for Doppler measurements such as PVFV. Ultrasound measurements can vary with operator technique, probe positioning, Doppler angle optimization, and overall experience. Reliable estimation of reproducibility ideally requires independent repeat measurements on the same patients by multiple operators, with agreement quantified using statistics such as the Intraclass Correlation Coefficient (ICC) for continuous variables or Cohen’s kappa for categorical parameters. As duplicate blinded assessments were not performed in our study, inter-observer reliability could not be quantified. However, to minimize operator-related variability, all POCUS examinations were performed by the same two investigators, both of whom underwent structured training in portal ultrasound under a radiologist. Prior to patient enrollment, each completed 25 supervised portal vein ultrasound examinations to achieve competence in image acquisition and interpretation. These measures helped standardize technique although formal reproducibility testing remains an important area for future research.
Second, although the operator performing the POCUS examination was blinded to patients’ comorbidities, including prior diagnosis of CLD, physical examination findings such as jaundice, stigmata of chronic liver disease, or visible ascites may inadvertently influence operator perception and could introduce subtle bias during image acquisition or interpretation. We attempted to minimize this effect through blinding to history of comorbidities and structured training for image acquisition. Additionally, obesity and bowel gas may obscure visualization in some patients. The preload on the heart and interplay of other factors, such as increased intra-thoracic or intra-abdominal pressures, may influence portal hemodynamic indices. These factors may cause subtle changes in the portal vein indices during active resuscitation and needs further research.



Comments (0)