
Remember me
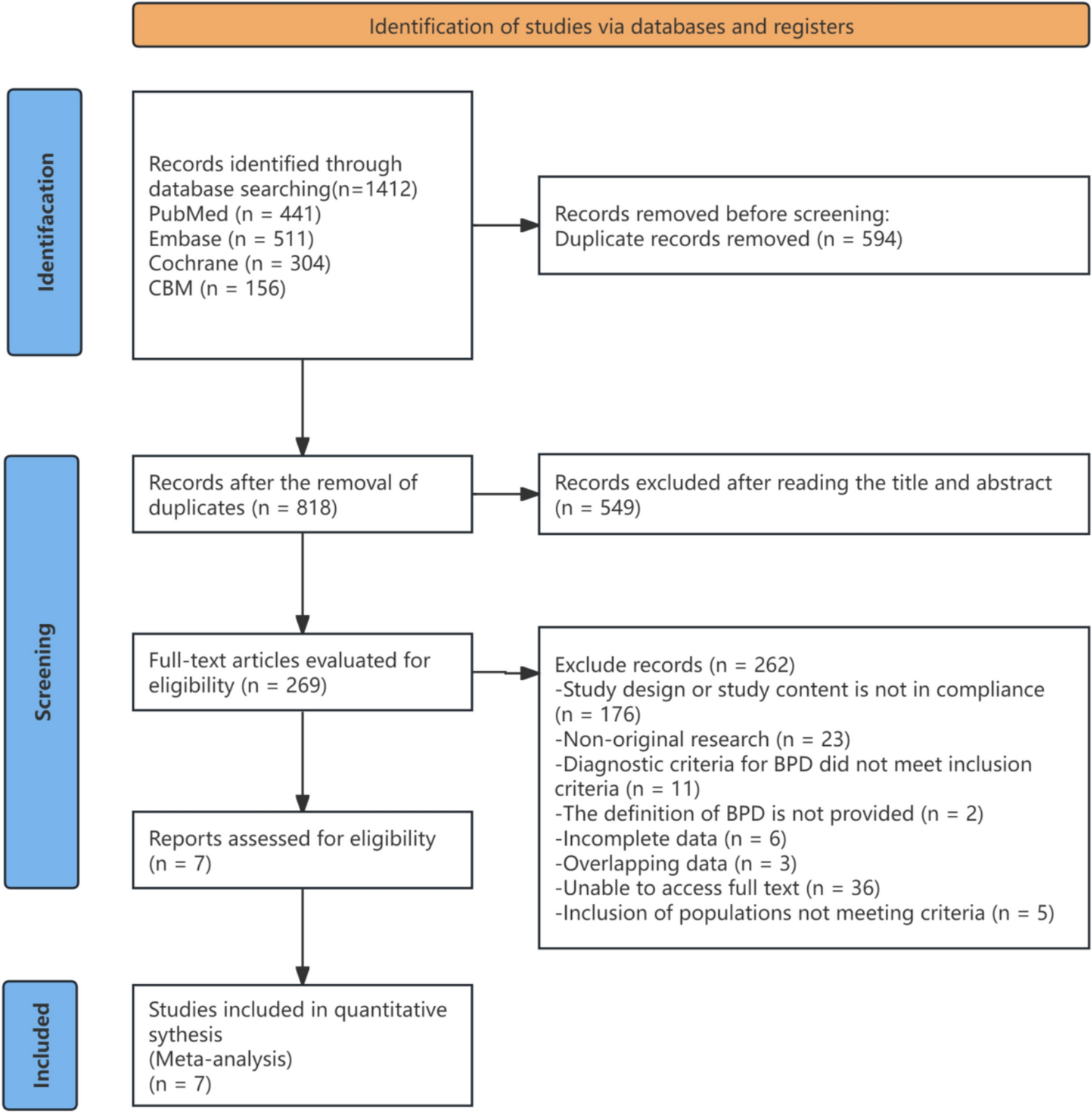
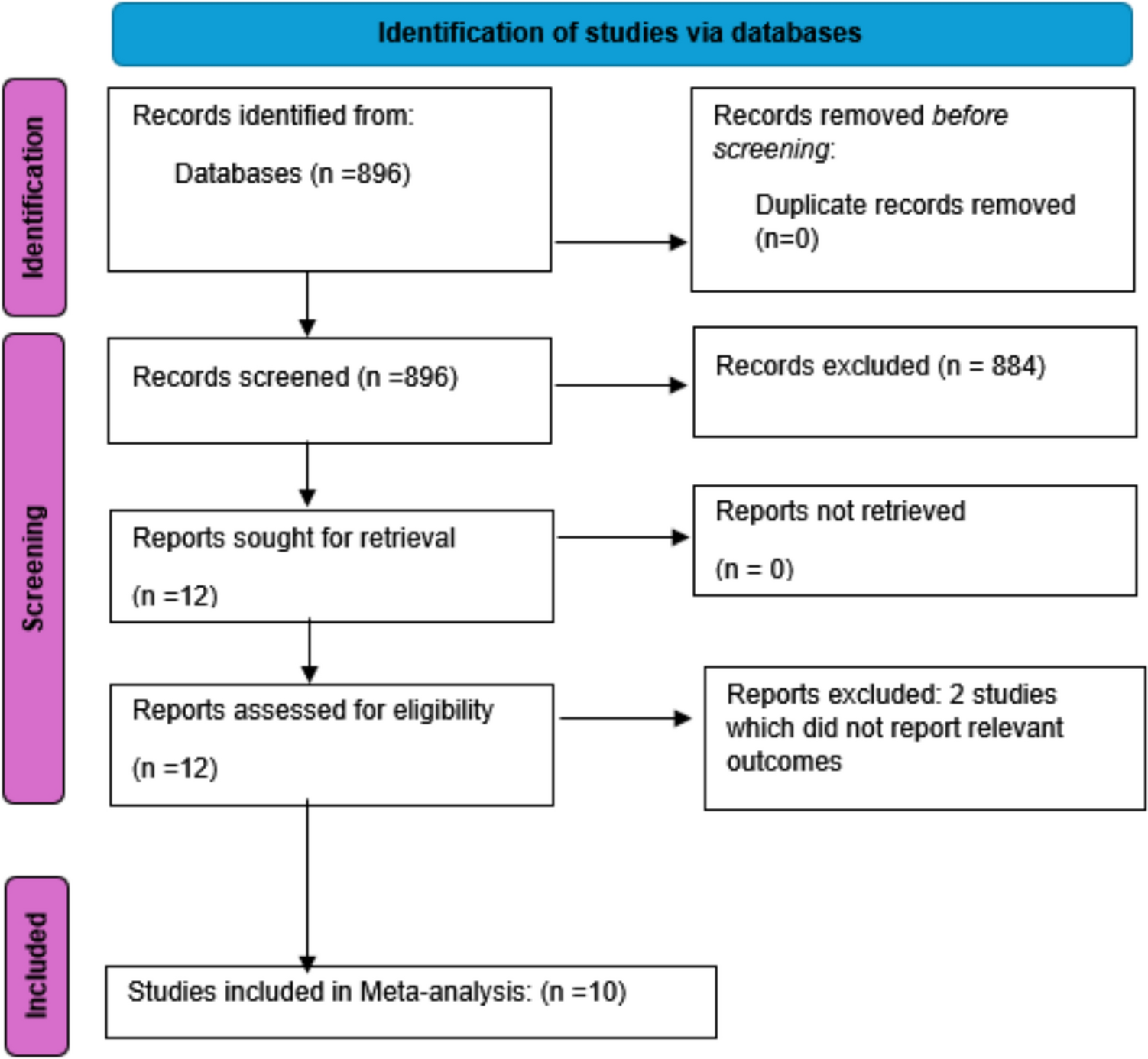
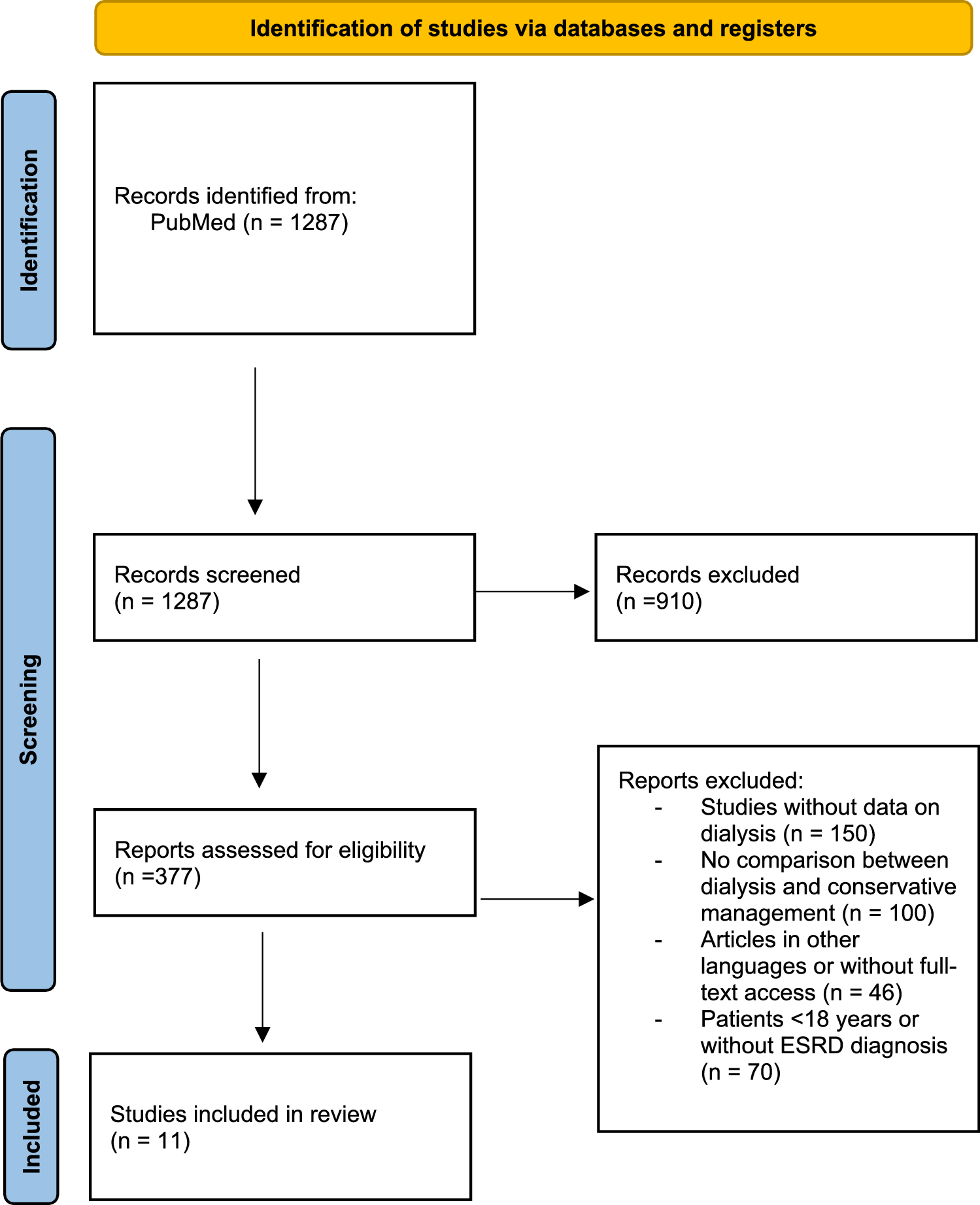


The study selection process is illustrated in Fig. 1. A total of 1,287 records were identified through the PubMed database. After title and abstract screening, 377 full-text articles were assessed for eligibility, of which 11 studies met the inclusion criteria and were included in the qualitative synthesis.
Fig. 1
PRISMA flow diagram of study selection
The reviewed evidence demonstrates that outcomes under dialysis and conservative kidney management (CKM) diverge substantially according to patient frailty, comorbidity, and functional reserve. Across studies, dialysis confers a survival advantage mainly in younger, less comorbid individuals, whereas in frail older adults, CKM often provides comparable, or more favorable, patient-centered outcomes. A total of eleven studies evaluated dialysis versus CKM in older adults with kidney failure, approaching the question from complementary perspectives. Four studies directly compared hemodialysis with CKM in elderly patients [2, 4, 6, 7], while one study developed a prognostic tool to estimate 2-year mortality under both dialysis and conservative pathways [10]. One systematic review assessed health-related quality of life and symptom burden [3], and one survey study explored physician recommendations, revealing marked variability and noting that physicians were often more likely to choose dialysis for themselves than for their patients [5]. Two additional studies focused on dialysis withdrawal and end-of-life patterns [11, 12], and two examined factors influencing treatment choice beyond survival [1, 8]. Collectively, these findings indicate that frailty, age, and comorbidity critically shape both treatment selection and prognosis.
The key characteristics and main findings of the included studies are summarized in Table 1.
Table 1 Comparative summary of key studies comparing dialysis vs. conservative kidney management (CKM) in older adultsPatient characteristics, survival, and prognosisAcross the broader literature synthesis, conservative kidney management cohorts were older on average [CKM: 83 ± 4.43 vs. ITD (intention-to-dialysis): 78 ± 4.38], more likely to have multiple chronic conditions, and frequently functionally impaired, while dialysis cohorts tended to be younger, fitter, and less dependent at baseline. Reported comorbidities spanned cardiovascular disease (ischemic heart disease, heart failure, atrial fibrillation, peripheral vascular disease, stroke), diabetes, cerebrovascular disease/dementia, and depression, with several studies showing a higher overall comorbidity burden in CKM than in dialysis cohorts [3, 8]. Baseline characteristics and survival outcomes of the included cohorts are detailed in Table 1.
In a Spanish geriatric cohort, older age and pre-frailty independently predicted the selection of conservative kidney management, while cognitive impairment and dependence in activities of daily living were also more common. These findings highlight that functional reserve, rather than kidney function alone, often determines treatment choice in late life [8].
Nutritional and comorbidity profiles also shaped modality selection: patients who underwent in-center kidney replacement therapies had lower serum albumin (3.7 ± 0.6 vs. 4.0 ± 0.4 g/dL), reinforcing the observation that both biological vulnerability and functional decline influence decisions regarding dialysis initiation.
SurvivalFour studies directly compared survival between hemodialysis and CKM. Collectively, they indicate that while dialysis can prolong life in selected patients, the benefit is modest and often vanishes with substantial comorbidity. In UK cohorts of patients aged ≥ 75 years, dialysis conferred higher 1- and 2-year survival than CKM, but this advantage was lost among those with high comorbidity, particularly ischemic heart disease [7].
Another analysis showed only a 5-month adjusted survival gain with dialysis in highly comorbid patients and identified the rate of eGFR decline as a stronger mortality predictor for CKM but not for dialysis [2].
Conversely, a Spanish geriatric cohort study found no significant survival difference between conservative kidney management (CKM) and dialysis (log-rank p = 0.098). However, patients managed conservatively experienced more frequent hospitalizations and greater progression to frailty during follow-up, while overall mortality rates were similar between the two groups [8].
A single-center UK cohort of patients ≥ 70 years likewise found longer median survival with dialysis but more hospitalizations, while CKM was associated with a higher chance of dying at home/hospice [4].
Overall, studies show a clear survival benefit of dialysis in patients who are younger and/or with lower comorbidity burden, but this benefit diminishes at older ages (≥ 75–80 years) and is lost in those with high comorbidity. For example, in cohorts over 75 years, dialysis conferred a median survival advantage (36 vs. 25 months), yet among patients with severe comorbidity, the difference was no longer significant (26 vs. 21 months), and in very frail geriatric series, no survival advantage was observed, although hospitalizations were more frequent in the conservative kidney management group. These nuances, advanced age, and comorbidity burden should be considered as central points in therapeutic decision-making at the bedside. The overall survival and hospitalization is presented in Table 2.
Table 2 Summary of survival and hospitalization presented in the studiesAcross included studies, survival outcomes were predominantly reported using Kaplan–Meier survival analysis, with median survival derived from survival curves rather than fixed-time survival rates. Direct numerical survival percentages were inconsistently reported.
PrognosisPrognosis was driven chiefly by patient-level risk rather than modality. The rate of eGFR decline independently predicted mortality in conservative kidney management, but not in those starting dialysis, highlighting disease trajectory as a key prognostic signal in the non-dialysis pathway [2]. Frailty or pre-frailty, cognitive impairment, and ADL dependence not only steered decisions toward conservative kidney management but were also associated with a higher hospitalization burden [8].
A multivariable prediction tool further demonstrated that individualized 2-year mortality estimates differed for the same patient under dialysis versus CKM, based on age, eGFR, cardiovascular disease, and malignancy, with moderate discrimination (C-statistics ~ 0.68–0.75) [10]. Complementary to this, the Multidimensional Prognostic Index (MPI) showed strong associations with hospitalizations and mortality across both pathways. Overall, frailty, comorbidity burden, and renal function trajectory outweighed the dialysis-versus-CKM distinction in shaping outcomes [6], and although physical functioning may initially appear superior in patients preparing for dialysis, health-related quality-of-life trajectories tend to converge over time. Notably, kidney-disease-specific quality of life often favors CKM, reflecting reduced treatment burden and greater autonomy.
Health-related quality (HRQoL) of life and symptomsIn patients with kidney failure (KF), the focus has increasingly shifted from merely prolonging life to enhancing its health-related quality. While dialysis may extend survival, it is frequently associated with physical discomfort, dietary restrictions, and frequent hospital visits, which can negatively impact daily functioning and social life, especially in older patients. Conservative kidney management has been proposed as an alternative in this category of patients. In a systematic review comprising 11 observational studies and a total of 1,718 patients, the HRQoL of individuals with CKD was evaluated, comparing those who chose conservative kidney management (CKM) with those who opted for dialysis. Physical health outcomes, assessed using validated instruments such as the 36-item Short Form (SF-36) and the 12-item Short Form (SF-12), were found to be lower in patients who selected CKM compared to those who had chosen dialysis but had not yet initiated treatment. These differences were evident in domains such as physical function, general health, and the physical component summary. However, once dialysis was initiated, physical health outcomes between the two groups became comparable, regardless of dialysis modality [3].
The symptom burden, as reflected in mental health outcomes, was found to be similar across both groups. This includes domains such as the mental component summary, vitality, social functioning, emotional role, and overall mental health. Over the long term, based on repeated assessments conducted over 12–36 months, mental health outcomes followed a similar trajectory in both groups, with no significant differences observed.
These findings suggest that while initial physical health may differ, long-term HRQoL trajectories in both physical and mental domains tend to align across treatment pathways. However, three studies that specifically evaluated kidney disease-related quality of life showed that patients who chose conservative kidney management reported better scores than those on dialysis, particularly in domains related to the impact of kidney disease on daily life and perceived burden of illness. Moreover, life satisfaction and general health status were found to decline after the initiation of dialysis, suggesting that starting dialysis may negatively affect certain aspects of well-being.
The questionnaires used in these studies for evaluation of health-related quality of life were SF-36, KDQOL-36, and KDQOL-SF. The SF-36 is a widely used generic health-related quality of life (HRQoL) questionnaire applicable across various medical conditions and populations. It consists of 36 items that assess eight key health domains (physical functioning, role physical, bodily pain, general health perceptions, vitality, social functioning, role emotional, mental health). The KDQOL is a disease-specific HRQoL instrument designed for patients with CKD, incorporating domains that specifically address the impact of kidney disease. There are two main versions: KDQOL-SF—combines SF-36 with kidney-specific items and KDQOL-36—a shorter version with 36 items, widely used in clinical settings.
Use of healthcare services and hospitalization ratesPatterns of healthcare utilization further differentiate CKM and dialysis pathways, particularly in terms of hospitalization frequency and place of death.
Regarding hospitalizations, we identified three studies that investigated this outcome. Two of them reported a higher frequency of hospital admissions among patients undergoing dialysis, while one study found increased hospitalization rates in patients receiving conservative kidney management (CKM). Carson et al. conducted an observational study involving 202 patients with a mean age over 70 years. Of these, 79 received conservative kidney management (CKM), while 123 underwent kidney replacement therapy. The study found a higher rate of hospitalization among patients treated with dialysis (0.069 days per patient versus 0.043 days in the conservatively managed group). This hypothesis, suggesting more frequent hospitalizations among dialysis patients, was further supported by a smaller observational study conducted on 56 patients, which reported similar trends in hospitalization rates favoring conservative kidney management (CKM) [8].
Regarding mortality, patients in the conservative treatment group were 4.5 times more likely to die at home compared to those receiving dialysis. When balancing age and associated comorbidities, death at home may, in some cases, reflect a greater degree of psychological comfort for the patient, potentially translating into a better perceived health-related quality of life.
In a large-scale study conducted in Taiwan involving 5,482 cancer patients, 4,484 undergoing hemodialysis, and 998 managed conservatively, patients receiving dialysis had a higher likelihood of hospitalization, thus supporting findings from previous studies [12].
Overall, dialysis is consistently associated with a higher hospitalization burden, while CKM offers greater potential for end-of-life care congruent with patient preferences. Hospitalization patterns across studies are summarized in Table 1.
Therapeutic decisions and predictive factorsThe decision to pursue dialysis or conservative kidney management (CKM) appears to be influenced by multiple factors, ranging from patient frailty and social status to the presence of comorbid conditions.
Beyond patient-level characteristics, physician perception and prognostic uncertainty also shape treatment recommendations.
In a small study involving 56 patients from nephrology centers in Madrid, Spain, the choice of conservative kidney management (CKM) over hemodialysis was more likely among elderly, frail individuals who were dependent on assistance and exhibited cognitive impairment. The presence of cardiovascular comorbidities did not appear to influence the treatment decision. However, patients with diabetes mellitus were more frequently found in the dialysis group. Based on this study, we conclude that patients who are older, more dependent for ADL (activities of daily living), and have more cognitive deficits are more likely to opt for conservative kidney management (CKM) over dialysis [8].
Further analysis of an observational study conducted in a UK renal center (Lister Hospital, Stevenage, United Kingdom) highlighted the importance of kidney function decline, measured by time-dependent estimated glomerular filtration rate (eGFR td), in predicting survival among CKM patients. In patients with high comorbidity, dialysis was associated with a non-significant adjusted survival advantage of 5 months. However, among CKM patients, those at the 25th percentile of eGFR td had an adjusted survival of just 7 months, compared to 63 months for those at the 75th percentile. This suggests that the rate of kidney function decline is a critical determinant of both treatment choice and mortality risk in conservatively managed patients [2].
Given the trust patients often place in their physicians, medical advice frequently plays a significant role in shaping treatment decisions. Building on this premise, Eric A. Finkelstein et al. conducted an interesting study in which they surveyed physicians attending the 9th Asian Forum of the Chronic Kidney Disease Initiative conference. The study used vignettes that vary by age and comorbidity status, and asked physicians to recommend dialysis or conservative kidney management (CKM) for a hypothetical patient with that profile and to predict survival with both treatment options. The physicians were predominantly mid-career clinicians (mean age 45, 60% male), representing a mix of internists, general practitioners, and nephrologists, with about half affiliated with public hospitals and an average of 8 years’ ESRD experience.
Physicians generally believe that dialysis offers greater survival benefits than conservative kidney management (CKM), regardless of patient profile. However, a notable proportion of physicians (up to 50% in some scenarios) believed CKM could offer better survival than dialysis, especially in cases involving advanced cancer. Surprisingly, 25% of physicians still recommended dialysis for patients with advanced cancer. Even in scenarios where dialysis is expected to be most beneficial (e.g., younger patients with diabetes), only 62% of physicians recommended it. As age and comorbidities increase, the percentage recommending dialysis drops significantly (e.g., 34% for an 85-year-old with diabetes and CHF). Taken together, older age (85 years), advanced cancer, and low socioeconomic status decreased the likelihood of recommending dialysis [5].
These findings underline how personal beliefs and risk interpretation among clinicians contribute to treatment variability, underscoring the need for standardized CKM prognostic tools.
Physicians who were more optimistic about dialysis outcomes were more likely to recommend it, even in poor-prognosis cases. This highlights the role of personal beliefs and biases in clinical decision-making. When considering treatment for themselves, physicians were less likely to choose dialysis if they had advanced cancer, but more likely if they were 75 years old or middle-class. Thus, when physicians are asked what treatment they would choose for their patients, it becomes evident that the decision to opt for conservative kidney management (CKM) is primarily influenced by factors such as older age (85 years), low socioeconomic status, and advanced cancer [5].
Although conservative kidney management (CKM) may be an appropriate option for certain categories of patients, the challenge remains: how can we determine the most suitable treatment approach for each individual? An observational, retrospective study conducted at a single center in the Netherlands aimed to address this question by analyzing 366 patients aged ≥ 70 years with stage 4 or 5 chronic kidney disease (CKD), treated between 2004 and 2016. The objective was to identify predictors of 2-year mortality based on the initial treatment decision, dialysis or conservative kidney management. Predictors included age, eGFR, presence of malignancy, and cardiovascular disease. Separate logistic regression models were developed for each treatment group and internally validated using bootstrapping techniques. Model performance showed moderate discrimination, with optimism-corrected C-statistics ranging from 0.675 to 0.750, and good calibration, indicating reliable prediction of outcomes. [10].
These findings suggest that simple clinical variables (age, eGFR, presence of malignancy, and cardiovascular disease) available at the time of treatment decision can be used to estimate short-term survival and may support shared decision-making in elderly CKD patients [10].
In another observational study conducted on 211 patients with chronic kidney disease (CKD stage 4–5) from a multidisciplinary KF unit at Hospital Universitario de la Princesa in Madrid, Spain, the decision regarding the modality of kidney replacement therapy (KRT) was significantly influenced by clinical, nutritional, and inflammatory parameters. In-center hemodialysis patients had higher Charlson Comorbidity Index (CCI) scores and less favorable biochemical profiles, including lower serum albumin, prealbumin, transferrin, hemoglobin, and eGFR, and higher CRP levels, compared with those on home-based KRT [1].
Taken together, the included studies, originating from diverse settings such as Spain, the United Kingdom, and the Netherlands, suggest that acceptance of conservative kidney management likely varies substantially across regions, influenced by cultural norms, ethnic composition, healthcare system structure, and broader geographic factors. Although none of the included studies were designed to compare cultural or geographic differences, the fact that decision-making around CKM is shaped by patient preferences, social support, and local clinical practice—as described across cohorts from Spain, the UK, and the Netherlands—suggests that substantial global variation in the acceptance of CKM is likely.
Taken together, these factors highlight the need for a structured, patient-centered approach that integrates age, frailty, comorbidity burden, and patient preferences when considering dialysis versus conservative kidney management. To facilitate this process in clinical practice, a treatment decision guide is proposed, illustrated in Fig. 2.
Fig. 2
Treatment decision guide for older adults with kidney failure
This schematic illustrates a stepwise, patient-centered framework for treatment decision-making in older adults with kidney failure. The process begins with identification of the patient group and early elicitation of patient goals, values, and preferences, emphasizing shared decision-making throughout. Subsequent stratification is based on age (< 75 vs. ≥ 75 years), comorbidity burden, and degree of frailty or functional impairment. Patients with absent or mild comorbidities and minimal frailty may be considered for dialysis, while conservative kidney management is favored in those with advanced comorbidities or significant frailty. In intermediate clinical scenarios, individualized assessment of dialysis-related risks and discussion of conservative kidney management as an alternative are recommended. Shared decision-making with the patient and their support network is integral at every stage of the process.
Withdrawal from dialysisIn incident hemodialysis patients aged 80 years and older, treatment withdrawal represents a frequent and clinically consequential outcome. Evidence from Ko et al. indicates that approximately 10% of these very elderly patients discontinued dialysis, rendering withdrawal the second leading cause of death within this subgroup. The median interval between the last dialysis session and death was 10 days, reflecting the close temporal association of withdrawal with end-of-life. Compared with younger counterparts, patients ≥ 80 years had more than a threefold higher incidence of withdrawal. Determinants of this outcome included advanced age, non-Hispanic white race (in contrast to African American, Hispanic, and Asian patients, who were significantly less likely to withdraw), the presence of dementia, and initiation of hemodialysis with a central venous catheter rather than an arteriovenous fistula [11].
In addition, laboratory and clinical indicators consistent with the malnutrition–inflammation–cachexia syndrome—such as low body mass index, hypoalbuminemia, reduced normalized protein catabolic rate, and elevated leukocyte counts—were strongly associated with dialysis discontinuation, suggesting that frailty and nutritional compromise play central roles in this decision. Notably, even patients who ultimately withdrew had functional and clinical status sufficient to attend thrice-weekly in-center dialysis sessions, underscoring the complexity of decision-making beyond mere treatment feasibility. Geographic variation further influenced outcomes, with patients in certain Midwestern KF networks exhibiting higher odds of withdrawal, while those in New York demonstrated substantially lower rates [12].
Collectively, these findings highlight that dialysis withdrawal in the very elderly is shaped by an interplay of clinical vulnerability, sociodemographic characteristics, and regional practice patterns. The authors also acknowledged several limitations, including the absence of detailed data on symptom burden, functional status, and patient–provider decision-making processes, which may have further informed the context of dialysis withdrawal in this population. [11, 12].
Taken together, these studies consistently demonstrate that while dialysis may extend survival in selected, less comorbid patients, this benefit diminishes in the presence of frailty and multimorbidity. Conservative kidney management, by contrast, offers comparable health-related quality of life and lower hospitalization burden, particularly among the very elderly.
Comments (0)