
Remember me
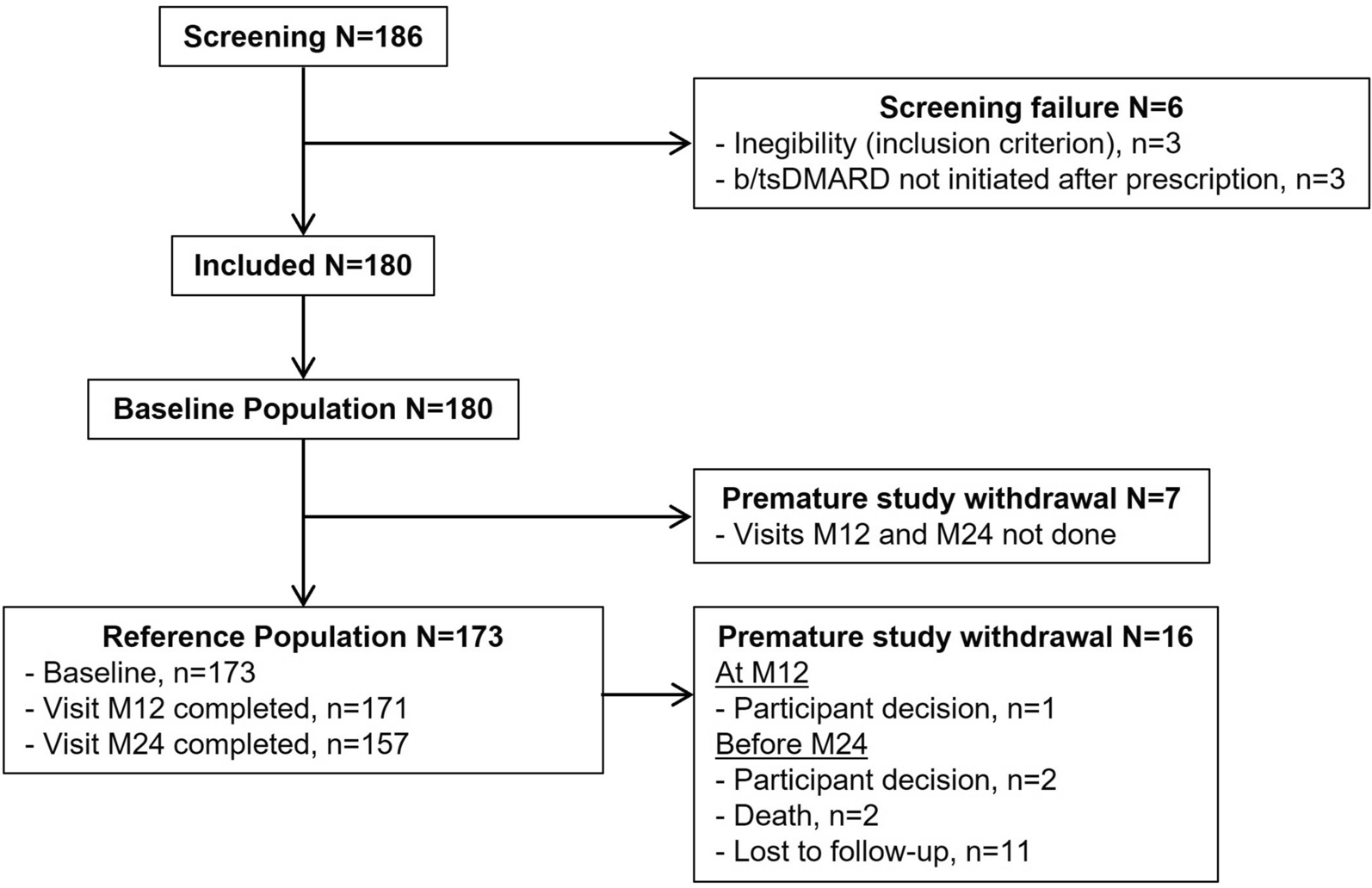

A total of 170 patients were registered for the study, of whom 41 were in the registration-only cohort for whom no CRFs were submitted. Of the remaining 129 patients, four were excluded (1 patient had no available CRF and 3 were off-label users), resulting in 125 patients from 58 sites included in the safety analysis population. Eleven patients previously treated with canakinumab in a clinical trial were excluded from the efficacy analysis set, resulting in 114 patients in the efficacy analysis population. Patient demographics and disease characteristics at baseline are summarised in Table 1. In the safety analysis population, 56.8% of patients were female, mean age was 11.4 years and approximately 70% of patients were between the ages of 6 and 20 years. Disease duration was ≥ 4 years in 47.2% of patients, and nearly 70% of patients had mild disease activity or better at baseline.
Table 1 Patient demographics and disease characteristics at baseline (safety analysis set)Exposure to CanakinumabThe median duration of treatment with canakinumab (including interruptions) was 710.0 (range 1–729) days and the median total number of doses was 25.0 (range 1–29). Canakinumab was discontinued in 30 patients (24.0%) in the safety analysis population, most commonly due to AEs, including worsening of the underlying disease in 14 patients (11.2%), inadequate response (7 patients, 5.6%), change to other therapies (3 patients, 2.4%) and achievement of the therapeutic goal (3 patients, 2.4%). Interruption of canakinumab occurred in 12 patients (9.6%), most commonly due to AEs (5 patients, 4.0%) and physician’s decision (5 patients, 4.0%).
SafetyAdverse EventsAdverse events occurred in 91 out of 125 patients (72.8%) in the safety analysis population (Table 2). The most common AE was relapse, worsening or exacerbation of Still’s disease (24 patients, 19.2%), followed by upper respiratory tract inflammation (18 patients, 14.4%), gastroenteritis and HLH (11 patients, 8.8% each), Coronavirus disease 2019 (10 patients, 8.0%) and abnormal hepatic function (9 patients, 7.2%). Serious AEs occurred in 49 patients (39.2%), with the most common being relapse, worsening or exacerbation of Still’s disease (17 patients, 13.6%) and HLH (11 patients, 8.8%). All other serious AEs occurred in ≤ 2 patients each.
Table 2 Adverse events occurring in five or more patients, by system organ class and preferred term (safety analysis set)In 35 patients (28.0%), AEs were judged to be related to canakinumab. The most common related AE was HLH (5 patients, 4.0%), followed by upper respiratory tract inflammation (4 patients, 3.2%); all other related AEs occurred in ≤ 3 patients each. Related AEs most frequently occurred between 24 and 36 weeks after the initiation of canakinumab therapy.
Serious related AEs occurred in 22 patients (17.6%), with the most common being HLH (5 patients, 4.0%). At end of study, all serious related AEs were reported as resolved or resolving, except for one event each of Crohn’s disease (not resolved), Epstein-Barr virus (EBV) infection (fatal) and autoimmune hepatitis (outcome unknown).
A total of nine related AEs led to discontinuation of canakinumab, including two instances of Crohn’s disease (one of which was considered possibly also related to the underlying disease) and one event each of EBV infection, infectious mononucleosis, HLH, ulcerative colitis, autoimmune hepatitis, liver disorder and relapse, worsening or exacerbation of Still’s disease.
Two deaths occurred during the study. One patient with a history of MAS and complications of HLH and liver disorder died following an opportunistic infection and cerebral haemorrhage that were not considered related to canakinumab. Another patient, with a history of MAS, complications of Kawasaki's disease, HLH and hypertension, developed aggravation of sJIA, MAS, EBV infection and EBV-associated lymphoproliferative disorder with liver metastases, and died due to subsequent rupture of lymphoproliferative site of the liver during an episode of MAS. Although the EBV infection was reported to be related to canakinumab, causality for all other events could not be conclusively established.
Safety ConsiderationsAmong the specific safety considerations selected for investigation, AEs judged to be related to the study drug occurred in 14 patients (11.2%) in the form of infections (including opportunistic infections), in five patients (4.0%) as MAS, in three patients (2.4%) as hepatic impairment and in two patients (1.6%) as neutropenia. No AEs of shock/anaphylaxis or malignancies were reported.
A total of ten MAS-related events were reported among the five patients with MAS as a related AE. All were cases of HLH and were considered to be serious. Seven of these events resolved and three were resolving at the time of reporting; the latter occurred in a single patient who experienced four MAS events, three resolving with treatment interruption and one that resolved after discontinuation of canakinumab. All events required symptomatic therapy. The median time from canakinumab initiation to the first MAS event was 389 (range 71–582) days, and the median event duration was 17 (range 7–144) days.
The most common related infection events were bacteraemia, cellulitis, infectious mononucleosis, influenza and tonsillitis (each in 2 patients, 1.6%). Ten patients experienced 15 serious related AEs, including two cases each of bacteraemia and infectious mononucleosis; the remaining serious events occurred once each. Outcomes were reported as resolved (11 events) or resolving (3 events), except for one fatal case of EBV infection.
Safety Analysis by Patient CharacteristicsThe incidence of related AEs was analysed in relation to the following patient characteristics: sex, pregnancy, age, disease duration, hepatic impairment, renal impairment, medical history of MAS, body weight category, PGA, prior use of tocilizumab, prior canakinumab treatment, concomitant drugs and duration of concomitant oral steroid use. For all factors, the 95% CIs for the ORs included 1, indicating no association of these factors with safety outcomes.
EffectivenessGlucocorticoid Dose ReductionAmong patients who were receiving concomitant glucocorticoid at baseline, the proportion who achieved a successful glucocorticoid dose reduction increased over time, as shown in Fig. 1. At 104 weeks post canakinumab initiation, 67.2% of patients had achieved successful dose reduction. The mean (standard deviation [SD]) daily glucocorticoid dose (oral prednisolone equivalent) at baseline was 0.4 (0.4) mg/kg. Mean (SD) changes from baseline over the course of the study were − 0.2 (0.4) mg/kg at 28 weeks, − 0.3 (0.4) mg/kg at 48 weeks and − 0.3 (0.5) mg/kg at 104 weeks, with a gradual reduction in dose observed over time.
Fig. 1
Proportion of patients with a successful glucocorticoid dose reduction. Effectiveness analysis set. n indicates the number of patients receiving concomitant glucocorticoid at baseline and on continued treatment with canakinumab at each evaluation time point. Error bars indicate 95% confidence intervals. Success was defined as glucocorticoid dose reduction (oral prednisolone equivalent) meeting any of the following: reduction to ≤ 0.5 mg/kg from > 0.8 mg/kg baseline; reduction by ≥ 0.3 mg/kg from 0.5 to 0.8 mg/kg baseline; reduction to ≤ 0.2 mg/kg from any baseline; or any reduction from ≤ 0.2 mg/kg baseline
Effectiveness Analysis by Patient CharacteristicsThe proportion of patients with a successful glucocorticoid dose reduction was analysed by the following patient characteristics: sex, pregnancy, age, disease duration, hepatic impairment, renal impairment, medical history of MAS, body weight category, baseline PGA, prior use of tocilizumab, prior canakinumab treatment, concomitant drugs, and duration of concomitant oral steroid use. Patients with a baseline PGA score of 3–4 (moderate or severe signs and symptoms) had a lower likelihood of achieving a successful glucocorticoid dose reduction compared with those with a PGA score of 0 (no signs and symptoms; OR 0.06, 95% CI 0.01–0.62).
Common Signs and Symptoms of sJIAThe proportion of patients without common signs or symptoms of sJIA increased from 76.0% (79/104) at baseline to 97.9% (93/95) at 28 weeks, and remained ≥ 90% thereafter, with 95.4% of patients (83/87) being without signs or symptoms at 48 weeks and 93.8% (76/81) at 104 weeks.
Remission and RelapseSymptom remission increased over time, from 38.6% (44/114 patients) at 48 weeks to 50.9% (58/114 patients) at 104 weeks. The rate of relapse after remission remained under 10% throughout, at 3.5% (4/114 patients) at 48 weeks and 7.0% (8/114 patients) at 104 weeks.
PGAChanges in PGA score over time are shown in Fig. 2. The proportion of patients assessed as having PGA ratings of 0 or 1 (no or slight signs and symptoms) increased from 46.5% (47/101 patients) at baseline to 80.2% (73/91 patients) at 28 weeks, and then remained at approximately 90% through to 104 weeks. The percentage of patients with PGA rating of 4 (severe signs and symptoms) was 5.9% at baseline and remained close to zero throughout the study period.
Fig. 2
Changes in physician global assessment (PGA) ratings over time. Effectiveness analysis set. PGA of disease activity score was determined based on signs and symptoms related to the underlying disease: 0, none; 1, slight; 2, mild; 3, moderate; 4, severe
CRP LevelsAt baseline, 83.5% (91/109) of patients had CRP within the normal range (≤ 1 mg/dL). By 104 weeks, all patients (85/85) had normal CRP levels. Median CRP level remained stable at 0.03 mg/dL from baseline through to 104 weeks. The mean (SD) CRP level at baseline was 0.9 (2.4) mg/dL, with mean (SD) changes of − 0.5 (2.3), − 0.4 (1.9) and − 0.6 (1.9) mg/dL at 28, 48 and 104 weeks, respectively, indicating decreases at all time points compared with baseline.
Comments (0)