
Remember me

An astonishing development has been observed in the treatment of patients with obstructive hypertrophic cardiomyopathy (oHCM) in recent years: the introduction of disease-specific medication, i.e., selective cardiac myosin inhibitors [1, 2]. Although many patients with oHCM are eligible for this medication, there are several barriers to its implementation. In addition to issues of differential diagnosis and cost, delayed diagnosis is another hurdle that we must recognize. I herein present two cases in which the initial clinical encounters did not lead to a suspicion of oHCM.
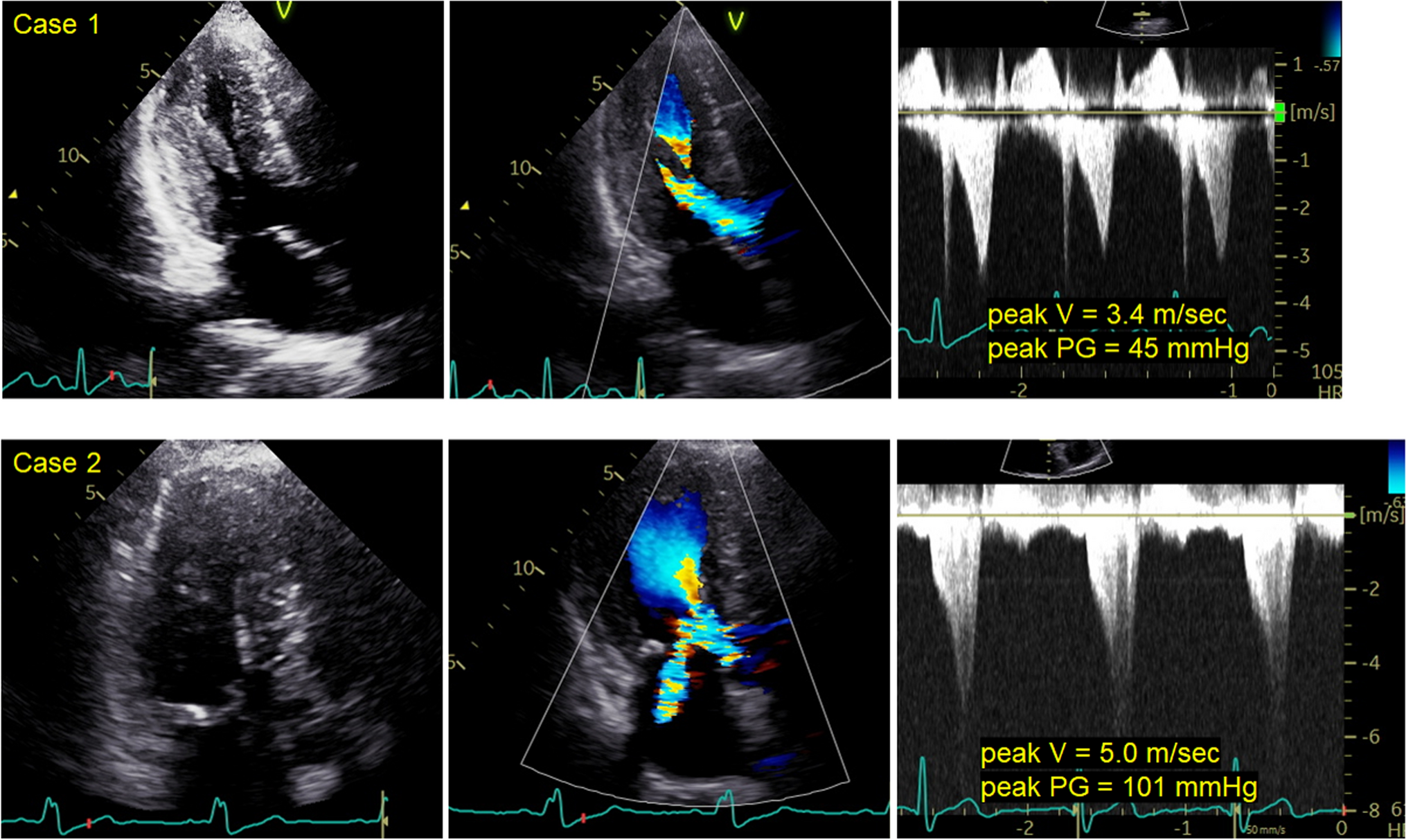
Case 1: A man in his 50 s visited our department complaining of faintness. His skin was sweaty and his systolic blood pressure was around 90 mmHg. A prominent systolic murmur was audible, and transthoracic echocardiography (TTE) demonstrated oHCM with an intraventricular pressure gradient of 45 mmHg even in the left-sided decubitus position (Figure: upper images). Despite multiple prior hospital visits for episodes of syncope, the patient had been managed for a presumed mental disorder. Following initiation of specific medical therapy for oHCM, his clinical condition stabilized.
Case 2: A woman in her 60 s visited our department complaining of chest discomfort. Angina pectoris was suspected and cardiac computed tomography was performed, revealing no organic stenosis in the coronary artery. She was then prescribed a beta-blocker, but her symptom did not resolve completely. Three years later, she visited again because her symptom had gradually worsened. Physical examination revealed a grade 3/6 systolic murmur at Erb’s area, and subsequent TTE confirmed a diagnosis of oHCM (Figure: lower images).

Although both of these patients are fortunately doing well, patients with oHCM remain at risk of sudden death. When diagnosing oHCM, it is essential to first suspect the presence of intraventricular obstruction. Detailed physical examination, especially cardiac auscultation, along with a thorough evaluation of the patient’s history of present illness, play a pivotal role. Patients with oHCM may present with distinctive symptoms, including dyspnea or blackout after exercise, and postprandial discomfort. When performing or ordering TTE, the possibility of intraventricular obstruction should always be considered. Otherwise, essential bedside stress echocardiographic assessments, such as the Valsalva maneuver or evaluation in the sitting position, may not be performed. Although TTE, including bedside stress assessments, is the most accessible method for diagnosing oHCM, it may delay the diagnosis if it is performed without appropriate prior clinical information.
Comments (0)