
Remember me


DTI has been studied across a variety of kidney disorders in both adults and children [7]. In this section, we will review potential applications of DTI in pediatric kidney diseases.
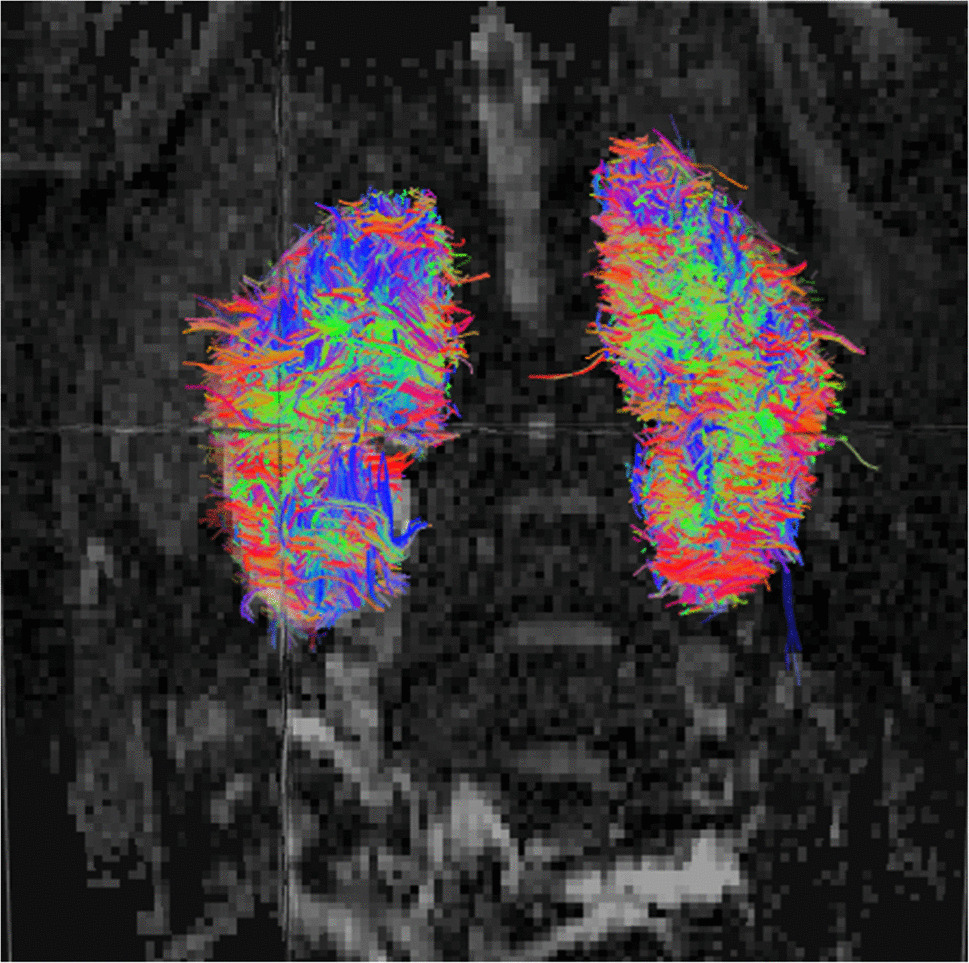
Diseases with strong evidence and clear pathophysiology for DTIPolycystic kidney diseaseIn autosomal recessive polycystic kidney disease (ARPKD), DTI detects microstructural disruption before conventional MRI shows overt changes, suggesting potential value for early diagnosis and treatment monitoring [10]. Children with ARPKD exhibit lower FA and disrupted tractography compared to healthy controls [10]. When comparing DTI of the kidneys in eight healthy children to six children with ARPKD, a previous study found that patients with ARPKD had significantly lower FA values (0.25±0.02) and mean track length (11.61±1.29 mm) when compared to healthy controls (0.33±0.03 and 16.73±3.43 mm, respectively) [10]. The study team concluded that DTI offers a novel approach for characterizing kidney disease based on changes in diffusion anisotropy and kidney structure [10]. An example comparison between a control patient and a patient with ARPKD is shown in Fig. 4.
Fig. 4
Coronal view diffusion tensor imaging tractography of a normal pediatric kidney of an 8-year-old boy (left) versus another 8-year-old boy affected by autosomal recessive polycystic kidney disease (right). Autosomal recessive polycystic kidney disease is associated with decreased fractional anisotropy, fewer coherent radial tracts, and substantial disruption of medullary organization, illustrating early microstructural disease not evident on conventional imaging
Another study by Lupica et al. focused on autosomal dominant polycystic kidney disease (ADPKD) [11]. Although both ARPKD and ADPKD involve cyst formation in the kidneys, ADPKD, the most common inherited kidney disease, typically manifests in adulthood due to PKD1 or PKD2 gene mutations, while ARPKD is a rarer, severe childhood form caused by PKHD1 gene mutations [12]. The Lupica et al. study found that parenchymal FA was significantly lower in adult ADPKD patients compared to healthy subjects. They also found a direct correlation between estimated glomerular filtration rate (eGFR) and FA, and an inverse correlation with creatinine. The authors suggest that DTI is a promising tool that could be used by nephrologists to evaluate ADPKD patients, highlighting early microstructure alterations without the need for a contrast agent [11].
Ureteropelvic junction obstruction (UPJO)A pilot study by Delgado et al. (2019) on children with UPJO demonstrated that, after controlling for age, FA and track length were lower in obstructed kidneys compared to those in normal kidneys [13]. The authors noted that further studies are needed to determine if this can differentiate UPJ obstruction from other forms of hydronephrosis.
When comparing DTI parameters in 22 kidneys with UPJ obstruction to 118 normal kidneys, a study in children found that mean FA values were significantly lower (0.31±0.07) in kidneys with UPJ obstruction compared to normal kidneys (0.40±0.08) [14]. The ADC was also marginally increased [14]. The study concluded that DTI-derived metrics, including FA and ADC, are potential biomarkers for assessing kidney parenchymal damage and differentiating kidneys with UPJ obstruction [14]. In patients with UPJO, reduced FA in the affected kidney correlates with severity and improves after surgical intervention. They reported that DTI may also help distinguish functional obstruction from non-obstructive dilation [14]. An example comparing a healthy kidney with a patient with unilateral UPJO is shown in Fig. 5.
Fig. 5
Representative coronal view images from a 6-year-old male healthy kidney vs an age-matched 6-year-old female patient with unilateral ureteropelvic junction obstruction. Obstruction is associated with lower fractional anisotropy, fewer coherent radial tracts, and visible disruption of medullary organization, aligning with the reported diffusion abnormalities in pediatric ureteropelvic junction obstruction
Kidney transplantationDTI is increasingly explored to monitor kidney transplant health [5, 9]. Kidney transplant recipients, particularly pediatric transplant patients, often require periodic biopsy for active surveillance to prolong allograft half-life. As such, the development of non-invasive markers of transplant rejection is highly desirable. Studies have demonstrated reduced FA and tract disruption in allografts undergoing acute rejection [15, 16]. In a study of 79 kidney transplant patients, DTI was able to detect patients with dysfunctional allografts [17]. In another study of 141 kidney transplant recipients with biopsy confirmation, DTI was able to show a higher diagnostic value than arterial spin labeling (ASL) in non-invasive identification of the degree of kidney allograft fibrosis [18]. In a pediatric study of kidney transplant patients, significantly smaller FA values and longer track lengths were observed in kidney allografts [9]. There were visual differences in DTI tractography between patients with high versus low Chronic Allograft Damage Index (CADI score) (Fig. 6); FA and track lengths between allografts with and without rejection were not significantly different, although this could be due to a small sample size. Findings have suggested DTI may potentially detect graft dysfunction earlier than serum markers. A study by Palmucci et al. found that DTI is a promising tool for the non-invasive monitoring of kidney function in kidney transplant recipients. Their study of 40 adult patients with a single kidney transplant found that medullary ADC and medullary FA were the most reliable parameters for assessing kidney function [19]. They concluded that medullary ADC was the best single parameter for assessing kidney function, with the highest area under the curve (AUC) for predicting normal kidney function or severe kidney impairment [19].
Fig. 6
Coronal view examples of transplanted kidney with Chronic Allograft Damage Index score <2 (left, 18-year-old male) and transplanted kidney with Chronic Allograft Damage Index score ≥2 (right, 15-year-old male). The allograft with a low Chronic Allograft Damage Index score (left) shows preserved corticomedullary alignment with dense, continuous radial streamlines. The allograft with a higher Chronic Allograft Damage Index score (right) demonstrates marked attenuation of tract density, fragmentation of streamline pathways, and loss of radial symmetry
Another study by Hueper et al. combined DTI and DWI to detect allograft dysfunction early after kidney transplantation in adult patients [20]. They found that FA was significantly reduced in patients with delayed graft function compared to those with initial graft function. The authors also noted that FA significantly correlated with kidney function and was inversely correlated with the amount of kidney fibrosis [20].
Diseases where DTI is promising but preliminaryDiabetic nephropathyPreliminary studies suggest DTI can detect subtle parenchymal changes in conditions such as diabetic nephropathy prior to the onset of clinical symptoms or changes in laboratory values [21,22,23]. A 2020 study by Deng et al. used a DTI-based radiomics signature to detect early kidney damage in patients with type 2 diabetes and found that texture features based on DTI could play a promising role in detecting early diabetic kidney damage [21]. Similarly, a 2017 study by Yan et al. investigated the use of DTI to assess kidney parenchymal injury in type 2 diabetic patients. The authors found that DTI showed a significant decrease in FA and an increase in ADC in the kidney medulla of diabetic patients, which correlated with the severity of their kidney disease [22].
Sickle cell diseaseA pilot imaging study by Donnola et al. compared DTI assessments of kidney microstructure in patients with sickle cell disease (SCD) and non-SCD control subjects. The study found a significant decrease in medullary FA in patients with SCD compared to controls, indicating microstructural alterations in the kidney medulla even without overt chronic kidney disease (CKD) [23]. These changes in medullary FA were consistent with previous studies on patients with CKD, suggesting that DTI provides a useful measure of kidney injury to complement other MRI assessments.
Acute kidney injury (AKI)DTI has also been explored as a tool to assess AKI that occurs as a complication of non-kidney conditions. A study by Li et al. investigated the diagnostic value of DTI in patients with acute pancreatitis (AP) who developed AKI. The study found that compared to patients without AKI, those with AKI had significantly lower FA values in the kidney cortex [24]. They concluded that DTI parameters could be a practical tool for diagnosing and predicting the severity of AKI in patients with AP [24].
Similarly, a 2020 study by Derlin et al. assessed the application of DTI for the non-invasive detection of kidney changes that correlate with AKI in patients after lung transplantation. The study found that all patients who underwent a lung transplant had a reduction in diffusion anisotropy, but only those who developed AKI had a significant reduction in kidney ADCs [25]. The study concluded that MR diffusion imaging enables non-invasive assessment of kidney changes that correlate with AKI early after lung transplantation [25].
Chronic kidney diseaseCKD is characterized by inflammation and fibrosis, and DTI is a promising, non-invasive technology for its evaluation. A recent study by Zhu et al. found that corrected diffusion-related indices, including cortical and medullary mean diffusivity (MD) and medullary FA, were superior to other imaging parameters for evaluating the severity of kidney pathology and function in CKD patients [26]. The authors also noted that these DTI parameters negatively correlated with glomerular and tubular interstitial fibrosis scores.
Other kidney disorders (emerging applications)In addition to the above conditions, DTI has been investigated for its utility in other kidney pathologies. While these studies have been performed primarily in adults, they could serve as a guide to future research applications in children.
Lupus nephritisRazek et al. evaluated the diagnostic value of DTI in the kidney cortex in assessing lupus nephritis (LN) [27]. The study found that the MD of the kidney cortex in LN patients was significantly lower, and the FA was significantly higher than that in healthy controls [27]. The study concluded that DTI metrics could help assess kidney affection in LN patients and predict pathological subtypes [27]. Similarly, Skeoch et al. demonstrated that non-contrast kidney MRI biomarkers, including those from DTI, are associated with standard measures of disease activity in lupus [28].
Oncological applications (tumor differentiation)DTI has also been explored for differentiating between kidney tumors. Feng et al. found that DTI could be used to differentiate low-fat kidney angiomyolipomas from clear cell kidney cell carcinomas, noting a statistical difference in both ADC and FA values [29].
Urinary tract infections (UTI)DTI can characterize kidney lesions in infants with UTI. Simrén et al. showed that DTI can distinguish between acute pyelonephritis and other kidney lesions, with acute inflammation presenting as increased signal on diffusion-weighted images and decreased ADC and FA values [30].
Comments (0)