
Remember me


All experiments were conducted according to institutional regulations and approved by the Purdue University IACUC (IACUC #2111002218). Sows were transported to Purdue Large Animal Hospital on the morning of surgery after fasting overnight. Sows were sedated prior to cesarean delivery using Telazol (tiletamine/zolazepam) and xylazine. Premature piglets were delivered via cesarean section at 103 days gestation, prior to the piglets reaching term at 115 gestational days. Piglets were resuscitated with light chest stimulation, nasopharyngeal suctioning, supplemental oxygen, and 1–2 drops of atipamezole (5 mg/mL) to reverse maternal anesthetic effects. Control piglets were sacrificed, and tissue was harvested within 4 hours of birth to establish baseline characteristics of preterm piglets. After resuscitation, radiofrequency temperature probes (2.1 mm x 13 mm, UID Temperature Programmable Microchip UCT-2112) were inserted subcutaneously, and central line catheters (Culex® Rat femoral vein catheter, Model CX-2021 S) were inserted into the jugular vein via a cutdown method. Piglets were placed in heated individual polystyrene incubator/nebulizer boxes equipped with water jacketed heating blankets. Homeostatic temperature was maintained over the course of the 5-day experimental study as established in the previously described model [26, 28,29,30] (Fig. 1).
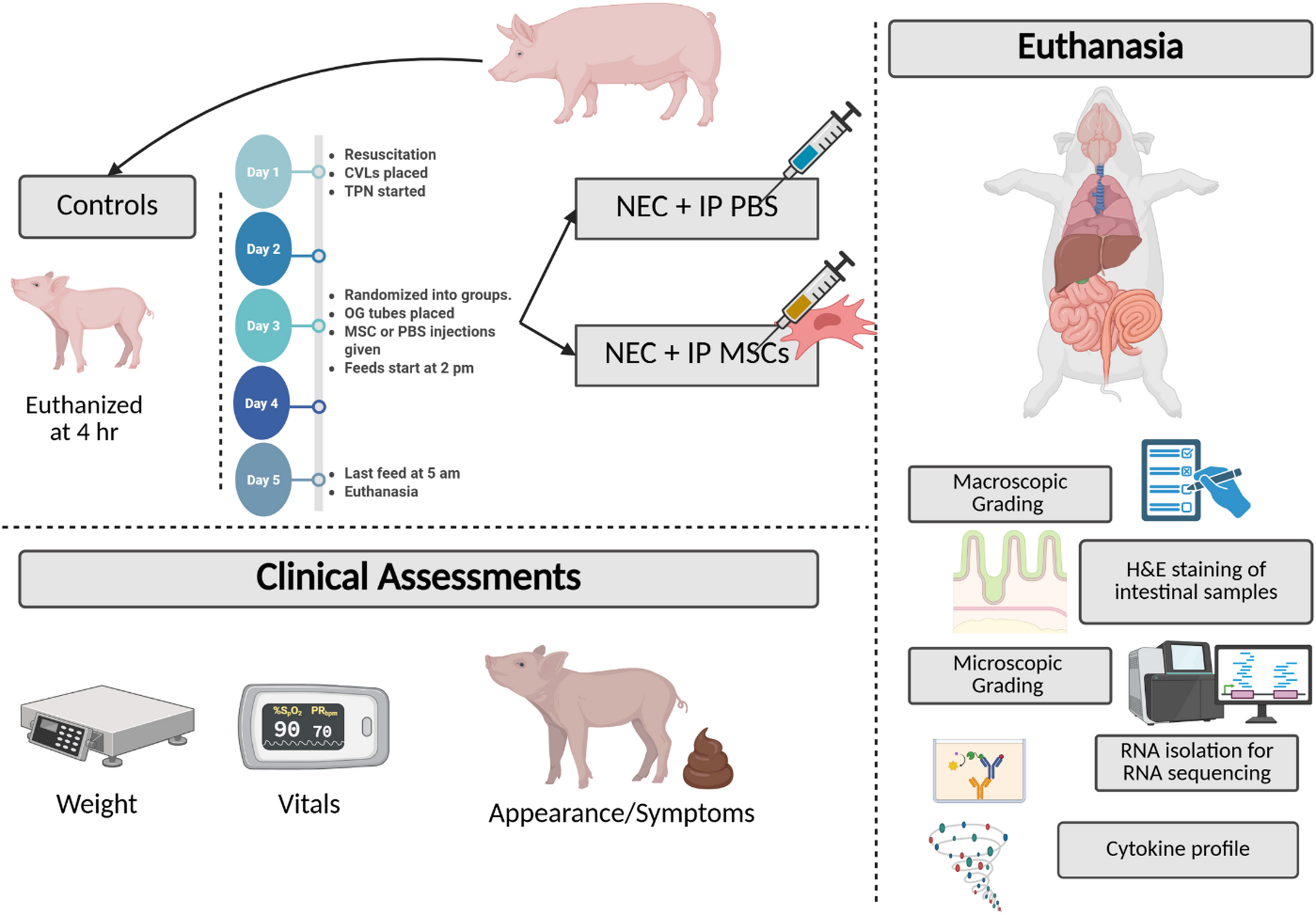
Fig. 1
The Premature Piglet NEC Model. Schematic representation of the preterm piglet model of necrotizing enterocolitis (NEC) and treatment with intraperitoneal (IP) mesenchymal stromal cells (MSCs). Control piglets received resuscitation but were euthanized 4 h after delivery without enteral feeding. Experimental piglets received central venous lines (CVLs) and total parenteral nutrition (TPN) on Day 1, were randomized to receive IP injections of either phosphate-buffered saline (PBS) or human MSCs on Day 3, and began enteral feeding on Day 3. Clinical assessments, including weight, vitals, and appearance/symptoms, were recorded daily. On Day 5, after the final feed, piglets were euthanized for sample collection. Post-mortem evaluations included gross and microscopic intestinal grading, hematoxylin and eosin (H&E) staining, cytokine profiling, and RNA sequencing of intestinal tissue. Created in https://BioRender.com
NEC protocolNEC was induced in piglets with total parenteral nutrition (TPN) starting on day 1 and hypertonic oral feeding via orogastric tube on day 3. TPN was initiated immediately after central venous access was achieved at a rate of 5 ml/kg/hr and continued until the end of the experiment. Parenteral nutrition provided (kg/day) 410 kJ energy, 12.5 g dextrose, 6.5 g amino acids, and 2.5 g fat (Intralipid 20%). Maternal plasma was administered intravenously at 4, 5, and 7 ml/kg at 6, 12, and 22 hours after birth, respectively, to provide passive immunity. Orogastric feeding tubes (5-Fr, NEOMED) were inserted prior to the initiation of gastric feeds. Position was confirmed with auscultation prior to the initiation of the first feed and if there were concerns for tube dislodgement. On day 3, enteral feeding was initiated at 15 ml/kg every 3 hours for 42 hours. Caloric nutrient content of the enteric formula is provided in Supplementary Table 1. Piglets (n = 7–9 per group) were monitored for the duration of the experiment with hourly pulse oximetry, temperature, and scheduled evaluations of clinical sickness. Clinical sickness scores were assigned using a standardized scoring rubric (see Supplementary Table 2). Weight change over the course of the experiment was documented. Piglets were euthanized via cardiac injection of sodium pentobarbital 390 mg/ml dosed at 0.22 ml/kg while under isoflurane anesthesia. All piglets who survived the length of the study were euthanized on day 5. At the time of euthanasia, serum was isolated from collected blood. Tissue from the terminal ileum were harvested uniformly and segments were placed in histology processing/embedding cassettes.
Cell cultureHuman induced pluripotent MSCs (iPMSC) were acquired from Cynata Therapeutics (Cremome, Australia). These MSCs were cultured in a serum free expansion medium consisting of 47.5% Human Endothelial Serum-Free Media (Thermofisher, Waltham, MA), 51.5% Stemline II Hematopoietic Stem Cell Expansion Media (Sigma-Aldrich, St. Louis, MO), 2 mM Glutamax (Thermo Fisher, Waltham, MA), 0.01 ng/mL Fibroblast Growth Factor (FGF-2) (R&D Systems, Minneapolis, MN), and 0.1 µM 1-thioglycerol. iPMSCs were cultured on fibronectin/collagen (Thermofisher, Waltham, MA /Sigma-Aldrich, St. Louis, MO) coated three-tiered 525 cm2 flasks. Cells were initially seeded at a density of 5,000 cells/ cm2 and passaged every 3–4 days. After reaching 80–85% confluency, iPMSCs were lifted using StemPro Accutase Cell Dissociation reagent (Thermofisher, Waltham, MA) at 0.5X and the reaction was stopped using deactivation media consisting of 4% Human Serum Albumin (25%, filtered, Nova Biologics, Oceanside, CA) and 0.5 mM EDTA in DPBS. The cells were then resuspended in 1.2mL of PBS, counted with a hemocytometer, and administered to piglets intraperitoneally in doses of 500,000 cells/kg (denoted as low-dose, or LD), 1 million cells/kg (denoted as mid-dose, or MD), or 10 million cells/kg (denoted as high-dose, or HD) using 1 mL syringes with a 21 gauge 1.5” needle on day 3 of the experiment. Untreated piglets (NEC group) were injected with PBS vehicle.
Clinical sickness score and macroscopic intestinal injuryEach piglet received a clinical sickness score prior to euthanasia (based on presence of diarrhea, bloody stool, and degree of abdominal distension). During necropsy, gross intestinal injury score was blindly calculated for each piglet based on the gross findings of the bowel. Previously described gross injury scoring [31] was used to assign scores to piglets.
Histologic intestinal injuryHistology cassettes were placed in 10% formalin and exchanged for 70% ethanol after 24–48 hours of fixation. These were embedded in paraffin, sectioned, and stained with hematoxylin-eosin. A ZEISS Axioscan was used to scan all slides. Each slide was evaluated at 10x magnification, and ten randomized photos of representative areas of the bowel were obtained. These photos were randomized and blindly scored by two independent graders. A scoring rubric previously described by Ragan et al. [31] was used by each grader to score the tissues.
Cytokine profiling by ELISASerum and terminal ileum samples were collected at necropsy and stored at − 80 °C until analysis. Concentrations of pro-inflammatory cytokines (IL-6, IL-17 A, and TNF-α) were quantified using commercially available porcine-specific ELISA kits (R&D Systems, Minneapolis, MN), following the manufacturers’ protocols. Cytokine levels in serum were reported as total picograms (pg) per mL sample. For terminal ileum, tissues were homogenized in lysis buffer (Buffer RLT, Qiagen), and cytokine concentrations were normalized to total protein content and expressed as pg cytokine/ng protein. All samples were run in duplicate, and standard curves were generated for each assay. Cytokine analysis was limited to the control, NEC, and medium-dose MSC (NEC + MD) groups.
Transcriptomic analysisTerminal ileal tissue was harvested from neonatal piglets (Sus scrofa) across three experimental groups: (1) Control, (2) NEC, and (3) NEC treated with the optimal mesenchymal stromal cell dose (NEC + MD). Total RNA was extracted using the RNeasy Mini Kit (Qiagen), following the manufacturer’s protocol. RNA integrity and concentration were assessed using the Agilent TapeStation system (Agilent Technologies, Santa Clara, CA). Samples selected for sequencing had RNA Integrity Numbers ranging from 3.7 to 8.3. Given the variability in RNA quality, a total RNA sequencing protocol was employed, which has high sensitivity to partially degraded RNA.
Library preparation was performed at the Center for Medical Genomics at Indiana University School of Medicine using the Illumina Total RNA-Seq protocol, which includes ribosomal RNA depletion and strand-specific paired-end library construction. Sequencing was carried out using the Illumina NovaSeq X Plus platform with 100 bp paired-end reads and NovaSeq X chemistry.
Raw reads underwent quality control using FASTQC, and low-quality reads, including those mapped to multiple locations, were excluded. Reads were aligned to the Sus scrofa reference genome using STAR [32], and genomic distribution across annotated regions was assessed using bamUtils [33]. Gene-level expression quantification was performed using featureCounts [34].
Differential gene expression analysis was conducted using edgeR [35] applying negative binomial generalized linear models with likelihood ratio testing. Comparisons included NEC vs. Control, NEC vs. NEC + MD, and Control vs. NEC + MD.
Smear plots were generated for each pairwise comparison to display log2-fold change versus log2-counts per million, highlighting significantly differentially expressed genes. Additionally, a heatmap of 15 inflammation- and injury-associated genes was constructed using the GraphPad Prism software, with expression values normalized and log-transformed to visualize relative gene expression across groups.
StatisticsStatistical significance between the groups was analyzed using GraphPad Prism software. Statistical analysis was performed using one-way ANOVA with Sidak’s post hoc test for normally distributed data, or Kruskal-Wallis test with Dunn’s post hoc correction for nonparametric data, to compare control, NEC, and MSC-treated groups. A p-value < 0.05 was considered statistically significant.
Comments (0)