
Remember me



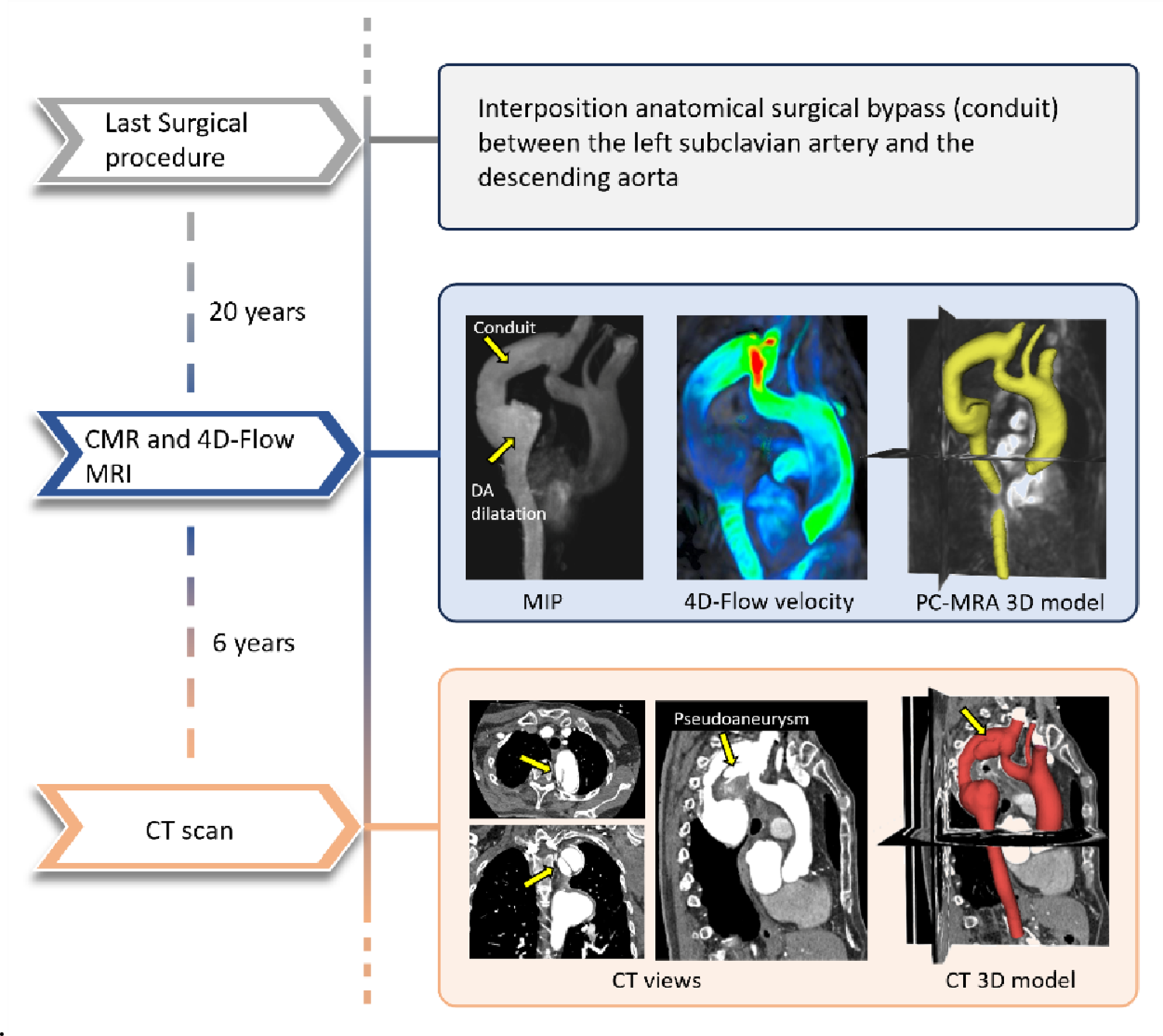

A patient with complex Ao-Coa underwent several surgical procedures, the last one was an interposition anatomical surgical bypass between the left subclavian artery and the descending aorta. The chronological course of the patient’s surgical procedures and imaging follow-up described here is summarized in the timeline shown in Fig. 1. During follow-up, CMR examinations were performed; the one reported here was acquired 20 years after surgical repair and confirmed a patent conduit, a native aortic isthmus, and a dilatation at the distal conduit–descending aorta anastomosis. The CMR examination with gadolinium contrast was performed on a 3 Tesla scanner (Ingenia, Philips Medical Systems, the Netherlands) according to a standard clinical protocol. A 4D-Flow MRI sequence was also prescribed in sagittal orientation covering the entire aorta with the following parameters: velocity-encoding of 200 cm/s in three directions, reconstructed spatial resolution 1.95 × 1.95 × 2.5 mm, flip angle 15°, the repetition time (TR)/echo time (TE) 4.8/2.8 ms, 20 phases, temporal resolution of 39.6 ms, and a sensitivity encoding factor of 2 without respiratory gating.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Case history timeline after complex aortic coarctation repair. The first arrow marks the last surgery. Twenty years later, CMR with 4D-Flow MRI shows: (i) MIP (Mean Intensity Projection), highlighting the patent conduit and distal anastomotic dilatation; (ii) 4D-Flow velocity map; (iii) PC-MRA overlaid on the 3D reconstructed model. Six years later, CT images in three standard views (i) demonstrate a pseudoaneurysm at the distal conduit–arch anastomosis, with the corresponding CT-based 3D reconstruction (ii)
Six years later, a CT scan was prescribed for the anatomical evaluation of the repaired coarctation and highlighted a new onset large pseudoaneurysm of the aortic arch at the level of the anastomosis with the conduit.
CT acquisition was performed with a 320-detector scanner (Toshiba Aquilon One, Toshiba, Japan), an iodinated contrast medium was adopted, and the dataset was characterized by a pixel size of 0.468 mm and a slice thickness of 1 mm.
The image datasets were retrospectively analysed to investigate the aorta hemodynamics during the Ao-Coa repair follow-up and assess the efficacy of CFD simulations to predict potential long-term complications starting from 4D-Flow MRI. The post processing of 4D-Flow MRI data was performed by a custom in-house software implemented in VMTK-Python, the 4D-Flow Phase Contrast Magnetic Resonance Angiography (PC-MRA) was computed and velocity patterns and WSS were evaluated [10]. Specifically, it was estimated from 4D-flow MRI by using a velocity-based linear extrapolation method, in which near-wall velocity gradients are estimated from adjacent voxels under the assumption of a linear velocity profile close to the wall, as previously described in [11].
3D models of the thoracic aorta before (3D-PRE) and after pseudoaneurysm formation (3D-POST) (Fig. 1) were reconstructed using 3D Slicer software. Both the 3D-PRE and 3D-POST models were segmented using a combination of threshold-based automatic segmentation and manual correction for complex regions, followed by surface smoothing with a low-pass Taubin filter to remove small artifacts. The 3D-PRE model was derived from the PC-MRA from the 4D-Flow MRI acquisition, while the 3D-POST model was reconstructed from follow-up CT images. As the vascular geometry and velocity field were both derived from the same 4D-Flow MRI dataset, they were inherently co-registered and shared the same spatial reference frame, allowing direct extraction of patient-specific inlet velocity profiles without additional rigid or non-rigid registration or interpolation procedures. The rigid registration between the 3D-PRE and 3D-POST models was performed solely for anatomical comparison and to identify, on the 3D-PRE geometry, the region corresponding to the site of subsequent pseudoaneurysm formation. CFD simulation was performed on the 3D-PRE model, to assess the potential role of hemodynamics in the later development of the pseudoaneurysm.
The computational domain was discretized using an unstructured volumetric mesh composed of tetrahedral elements in the core flow region and wedge elements in the near-wall boundary layers. A mesh sensitivity analysis was performed by systematically refining the mesh, and comparing the WSS and velocity results within the region corresponding to the site of subsequent pseudoaneurysm formation. Based on this sensitivity analysis, a mesh of approximately 1.52 × 106 elements with an average edge size of 0.9 mm was selected, incorporating four near-wall layers with a growth factor of 1.2 and a total boundary layers thickness of 1.5 mm.
The wall was assumed rigid, and the blood was modelled as a Newtonian incompressible fluid, characterized by a density of 1060 kg/m3 and a constant viscosity of 0.0035 Pa·s. Blood flow was assumed to be laminar throughout the computational domain. Although the local Reynolds number reached values of up to 3680 at peak systole, these conditions were short-lived (0.1 s within a 0.8 s cardiac cycle), and Reynolds numbers were substantially lower during the remaining phases (below 2040). In pulsatile vessels, transition to turbulence requires not only high instantaneous Reynolds numbers but also sufficient temporal persistence and spatial development. Therefore, the adoption of a laminar flow model is considered consistent with the hemodynamic conditions investigated and with common practice in large-artery CFD under physiological conditions. The patient-specific 2D velocity profile extracted from the 4D-Flow MRI dataset at the aortic sinotubular junction was applied directly as the inlet boundary condition of the CFD model. At the outlets, patient-specific pressure boundary conditions were prescribed for the supra-aortic branches and the descending aorta using a three-elements lumped-parameter Windkessel model [12]. The Windkessel model was implemented through a user-defined function written in C language and compiled within ANSYS Fluent, allowing the boundary conditions to reproduce the patient-specific haemodynamic behaviour derived from clinical data. A comparison between CFD simulation results and 4D-Flow MRI analysis is reported in Fig. 2 in terms of flow profile in the same selected planes: at descending aorta (DA), at brachiocephalic artery (BCA), at left common carotid artery (LCCA) and at left subclavian artery (LSA). This evaluation revealed a qualitative good agreement between the patient’s flow profiles and the results obtained from CFD simulation.
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Comparison of flow profile extracted from 4D-Flow data and obtained from CFD simulation at the supra-aortic vessels and descending aorta
The blood flow behaviour was investigated through the evaluation of velocity streamlines in the aortic lumen, in the arch and pseudoaneurysm region for three different phases of cardiac cycle: maximum acceleration (t1), systolic peak (t2) and maximum deceleration (t3). Additionally, the WSS for each of selected phases of cardiac cycle was calculated to better highlight the potential effect of flow pattern on the arterial wall. The velocity patterns were characterized by an increase in flow complexity at the beginning of descending aortic region (Fig. 3) in correspondence with the tract where pseudoaneurysm was diagnosed six years after the CMR examination.
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Focus on the region with the pseudoaneurysm (a), velocity streamlines at t1 (b), t2 (c) and t3 (d) instants of cardiac cycle
The WSS distribution along the aorta extracted from 4D-Flow MRI and calculated by CFD simulations are reported in Fig. 4(a-c) and (d-f), respectively. In Fig. 5 the distributions of velocity derived from CFD and 4D-Flow MRI data are depicted for selected cross-sectional planes, along with a focus on the WSS values in the region corresponding to pseudoaneurysm formation.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.WSS distribution extracted from 4D-Flow data at t1 (a), t2 (b) and t3 (c) instants of cardiac cycle; WSS distribution obtained from CFD simulations at t1 (d), t2 (e) and t3 (f) instants of cardiac cycle
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Focus on the CFD derived WSS values in the region corresponding to pseudoaneurysm formation at systolic peak; distributions of velocity at the three selected instants of cardiac cycle for three cross-sections in the region corresponding to pseudoaneurysm formation extracted from CFD and from 4D-Flow MRI data
Comments (0)