Children encounter a diverse set of foreign objects, and the specific location in which these objects become lodged in their bodies is subject to various factors. In line with previous investigations conducted by Na’ara S et al. [11], the present study revealed a greater occurrence of tracheobronchial foreign bodies among children younger than 3 years, with males being more affected than females at a ratio of 2.29:1. These findings are consistent with those reported in most previous studies [12,13,14]. The difference noted between the two genders could have stemmed from the heightened inquisitiveness and physical engagement of male children with their surrounding environment [15]. Solid foreign bodies accounted for 78.97% of all cases and were the predominant type of airway foreign body incident. Nuts, particularly peanuts and melon seeds, accounted for the greatest number of cases. These incidents were more prevalent during the winter and spring seasons. This pattern could be related to the fact that these months represent a period of traditional festivities in China when children have greater access to nuts such as peanuts and melon seeds [16]. These incidents are often a result of inadequate supervision by family members or improper feeding practices adopted by relatives. Moreover, the limited chewing ability of young children, coupled with activities such as running, laughing, and crying during meals, also contributes to the risk of airway foreign bodies. Therefore, family members of young children must exercise heightened vigilance to monitor whether their children are accessing or consuming food items that may cause airway obstruction. It is also imperative to enhance supervision of children accessing other potential objects that may become lodged in the airway.
Interindividual anatomical variations may lead to significant differences in the morphology of the left and right main bronchi. The left main bronchus has a characteristic slender structure, inclined to the longitudinal axis of the trachea at an angle of about 37.5 degrees. The right main bronchus, on the other hand, is thick, short, and steep, with an angle of about 23 degrees from the longitudinal axis of the trachea. The right main bronchus appears notably thicker, shorter, and straighter than its left counterpart, with the tracheal carina exhibiting leftward displacement [17]. These anatomical differences contribute to the increased vulnerability of the right main bronchus to the aspiration of foreign objects. Interestingly, the findings of the present study aligned with those reported previously by Ahmed and Shuiabu [18], who reported a slightly greater incidence of foreign body aspiration on the left side (46.20%) than on the right side (44.02%). Nevertheless, the conflicting findings reported in the literature suggest that the prevalence of impacted foreign bodies in the bronchi is either similar between the left and right sides or slightly more frequent on the left side in the Chinese population [19, 20]. The following could be the reasons for this:
1.
Children exhibit immature bronchial development, and the difference in the inclination of the left and right main bronchi between children and adults is not as evident. At a certain age, this inclination might even become equal on both sides. The type, shape, and size of a foreign body also influence its entry into the child’s body. A foreign body with a large volume tends to lodge in the trachea, whereas a relatively smaller body is more likely to enter the main bronchus or deeper parts on both sides.
2.
The position of the child while he/she is choking on the foreign body is another important factor to consider. The probability of the foreign body entering the right or left bronchus is different depending on whether the child is in an upright or oblique lateral position while choking. The right main bronchus appears notably thicker and shorter, so the foreign body can easily enter the right side in the upright position. In the oblique position, depending on the current position, it is not possible to predict which side of the bronchus a foreign body will tend to enter.
3.
The initial position of the foreign body within the tracheobronchial tube varies with time due to coughing, crying, or changes in the body position of the child, which may cause the foreign body to become dislocated [21].
Pneumonia, obstructive emphysema, pulmonary atelectasis, mediastinal emphysema, subcutaneous emphysema, granulomatous hyperplasia, etc., are the major complications of exogenous solid airway foreign bodies. Wang Y, et al. reported thin-slice CT as the best method for locating lodged foreign bodies, with an accuracy as high as 99.4% [22]. In the present study, a CT scan of the lungs of children revealed the following as the main comorbidities of foreign body aspiration: emphysema in 65 cases (35.33%), atelectasis in 40 cases (21.74%), subcutaneous emphysema/mediastinal emphysema in 8 cases (4.35%), and granulation tissue hyperplasia in 144 cases (78.69%). These complications caused by solid foreign bodies were not treated further, except for post-operative nebulized inhalation. The follow-up after a period of 2 weeks to 1 month revealed that all patients had been cured, except for 1 patients in which the granulation tissue was significantly enlarged, and symptoms of dyspnea were observed at the follow-up. The patient’s dyspnea was relieved after nebulized inhalation and intravenous glucocorticoid treatment. This observation indicated that treating airway obstruction could resolve the occurrence and development of complications. This would be important for prognosis. Therefore, bronchoscopy could be the most direct method for confirming the diagnosis and treatment of tracheobronchial foreign bodies [15, 23].
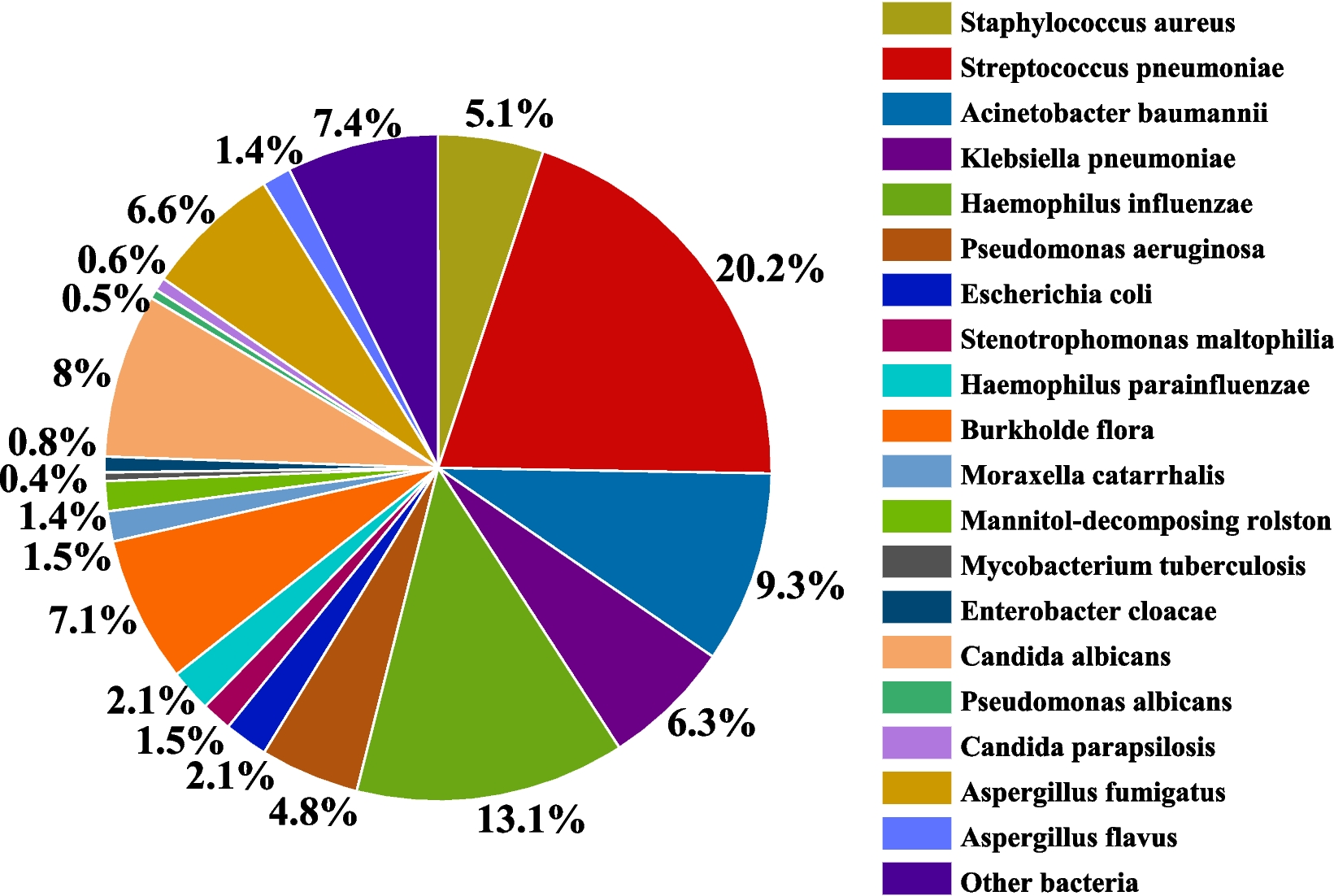
The bacterial culture examination was also performed for the 184 patients whose bronchoalveolar lavage fluid was used in the present study. The positive rate of bacterial culture was 15.76% (29/184). The most common bacteria isolated were Acinetobacter baumannii, which accounted for 27.57% (8/29) of the isolates, followed by Streptococcus pneumoniae [24.14% (7/29)], Klebsiella pneumoniae [20.69% (6/29)], Enterobacter cloacae [10.34% (3/29)], Staphylococcus aureus [6.90% (2/29)], Haemophilus influenzae [3.45% (1/29)], Pseudomonas aeruginosa [3.45% (1/29)], and Burkholderia cepacia complex [3.45% (1/29)]. The top three pathogens were Acinetobacter baumannii, Streptococcus pneumoniae, and Klebsiella pneumoniae, which is consistent with the reported distribution of common pathogens causing community-acquired pneumonia in children [24]. The results of the statistical analysis indicated the presence of a diverse set of infecting pathogens, including opportunistic pathogens. The author suggested that this could be related to the translocation and implantation of common respiratory tract parasites after foreign body aspiration or the presence of pathogenic bacteria carried by the foreign body itself. The early identification of infecting pathogens provides a basis for the rational use of antibiotics, which could reduce the risk of secondary infections resulting in pneumonia, lung abscess, lung necrosis, and other complications.
Exogenous solid foreign body insertion may result in the formation of airway granulation. The proliferation of granulation tissue may envelop the foreign body, making it difficult to identify the foreign body during bronchoscopy, which increases the abundance of granulation tissue, leading to misdiagnosis and leakage. The close relationship between the granulation tissue and the foreign body may cause local bleeding and mucosal swelling during the removal process. In patients with a significant amount of bleeding, rapid obstruction of the airway may occur, leading to asphyxiation and life-threatening situations. Therefore, the removal of the foreign body becomes further challenging in such cases [25].
Thomaskea reported the type of foreign object inhaled and the duration of its presence in the respiratory tract as the most significant factors leading to complications, including granulation tissue hyperplasia [26]. However, Zhang Yueming et al. reported that the factors contributing to granulation tissue formation are further complex and exhibit varying degrees of correlation with the nature of the foreign object and its lipid content. Therefore, further research is needed in this regard [27]. In this context, clinical data on whether children with foreign body aspiration exhibited lipid release were collected in the present study, followed by the application of logistic regression models in R language and XGBoost to model and analyze the factors influencing the formation of granulation tissue in the airway. Modeling analysis revealed that the duration of foreign body impaction and whether the foreign body released oil were high-risk factors for the formation of airway granulation tissue. The logistic regression model presented an AUC of 0.948, along with high precision, sensitivity, and F value. The XGBoost model presented an AUC of 0.902, along with good precision, sensitivity, and F value. According to this analysis, a critical time threshold was determined to predict whether airway granulation tissue would be formed. The threshold was as follows: when the duration of impaction of the foreign body that released oil was ≥ 99.98 h, and the duration of impaction of the foreign body that did not release oil was ≥ 47.94 h, it indicated the possible formation of airway granulation tissue.
Limitations of the present study
The present study has certain limitations that must be acknowledged. First, the data collected in the study were limited to the Quanzhou region in Fujian, which must have limited the comprehensiveness of the analysis in terms of the various types of solid foreign bodies. In addition, this study focused solely on the impact of oil release and the residence time of foreign bodies in the airway on the development of granulation tissue. However, other factors, such as the size, shape, and sharpness of the foreign bodies, could also play a significant role. Therefore, further refinement of these factors in future studies is necessary.






Comments (0)