
Remember me




This is a retrospective, prospective, multicenter, observational, real-world study and will be conducted to determine the long-term efficacy and safety of PEG-rhGH or rhGH for the treatment of SS in children in China. The inclusion of all the patients, treatment pattern, follow-up visits, and data collection will be performed as per standard clinical practices. The study will be conducted in about 1000 centers and approximately 10,000 patients will be enrolled in three cohorts—3000 patients in the retrospective cohort and 7000 patients in the retrospective-prospective cohort and the prospective cohort. The retrospective cohort will include patients who have been previously treated with PEG-rhGH or rhGH for at least 1 year at the initiation of the trial and have now completed the treatment regimen. Patients’ data will be collected retrospectively on the first visit and follow-up visits every 6 months. The retrospective-prospective cohort will include patients who have been treated with PEG-rhGH or rhGH at the initiation of the trial. Data will be collected retrospectively on the first visit and follow-up visits every 6 months, and then prospectively on the follow-up visits every 6 months until patients reach near-adult height (NAH). The prospective cohort will include patients who will be treated with PEG-rhGH or rhGH regimen. Data will be collected prospectively on the first visit and follow-up visits every 6 months until patients reach NAH. This study is planned to last for 16 years, including a 2-year period for starting study sites and recruiting patients as well as the follow-up period with patients in both the retrospective-prospective and prospective cohorts until they reach NAH. The study consists of three phases: screening and baseline period, intervention follow-up for every 6 months, and follow-up after the termination of the drug for every 6 months. In addition, only a portion of patients with GHD will be covered by medical insurance, and coverage will vary according to regional policies. Patients who are not covered, such as those with ISS, must make self-paid purchases through hospitals. Besides, financial incentives will be provided to both the investigators and patients. Investigators will receive compensation for their work and patients will be provided with transportation subsidies.
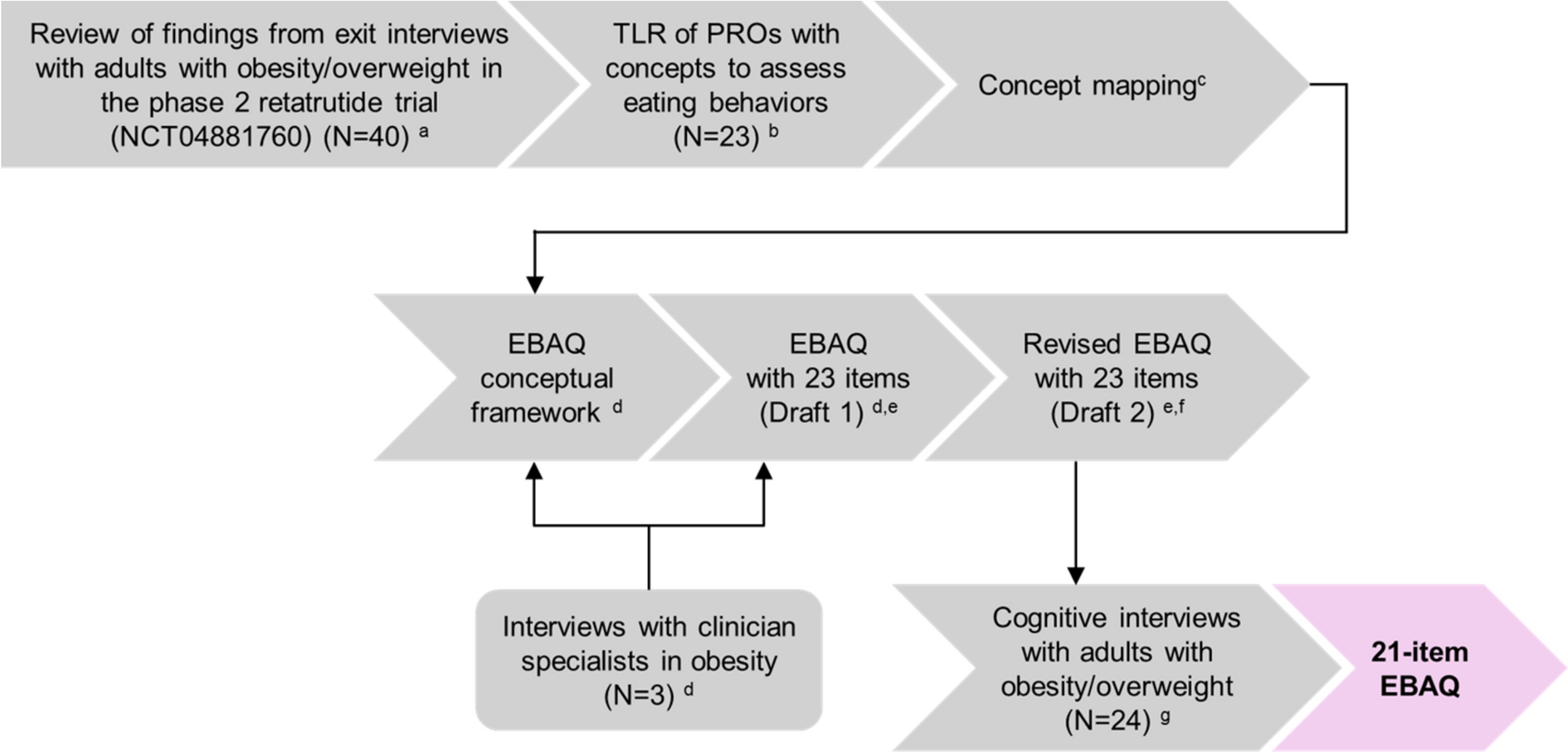
Inclusion criteria for patients’ enrollment into cohorts will be (1) voluntarily signed informed consent for the retrospective-prospective cohort and the prospective cohort; (2) children with SS aged ≥ 2 years; (3) height below the third percentile (− 1.88 SD) for normal, healthy children of the same age and sex; and (4) patients who have been previously treated with PEG-rhGH or rhGH for at least 1 year and who have now finished the treatment for the retrospective cohort and being treated with PEG-rhGH or rhGH for the retrospective-prospective cohort, and will be treated with PEG-rhGH or rhGH for the prospective cohort. Included patients should also fall under any of the following indications: cohort 1, GHD; cohort 2, ISS; cohort 3, small for gestational age (SGA); cohort 4, Turner syndrome (TS); cohort 5, Prader–Willi syndrome (PWS); cohort 6, Noonan syndrome (NS); and cohort 7, deficiency of the short stature homeobox gene on the X-chromosome (SHOX deficiency) and other causes of SS. The key exclusion criteria will be (1) patients having completely closed epiphyses; (2) patients treated with PEG-rhGH or rhGH for less than 1 year in the retrospective cohort, those who have been treated with and are anticipated to receive PEG-rhGH or rhGH treatment for less than 1 year in the retrospective-prospective cohort, and those who are anticipated to receive PEG-rhGH or rhGH treatment for less than 1 year in the prospective cohort; (3) patients with potential tumors, diagnosed with tumors, or having any signs of progression; (4) patients having hypersensitivity to GH or its protective agents; (5) patients already on different GH intervention other than the drugs used in the study, within 6 months before screening; (6) patients with incomplete medical records or anticipated inability to complete follow-up or collection of complete medical data; and (7) any unsuitable condition which will be considered by the investigator. The study flowchart is present in Fig. 1. Furthermore, the first patient was enrolled on October 25, 2023, and about 5000 patients have been enrolled so far.
Fig. 1
Study flowchart. SS short stature, GHD growth hormone deficiency, ISS idiopathic short stature, n number of subjects, NAH near-adult height, NS Noonan syndrome, PEG-rhGH polyethylene glycol (PEGylated) recombinant human growth hormone, PWS Prader–Willi syndrome, rhGH recombinant human growth hormone, SGA small for gestational age, SHOX short stature homeobox gene on the X-chromosome, TS Turner syndrome
Study ObjectivesThe primary objective of this study will be to evaluate the long-term safety of PEG-rhGH or rhGH for the treatment of SS in children in China. The key secondary objectives of the study will be to assess the efficacy of PEG-rhGH or rhGH for the treatment of SS in children with different etiologies. In addition, the exploratory objective will also be explored to compare the levels of insulin-like growth factor 1 (IGF-1) and body mass index (BMI) SDS before and after the PEG-rhGH or rhGH therapy. It will explore that how the GH treatment influences the nutritional status and IGF-1 level in the children with SS. Each individual will be examined for treatment-related or non-treatment-related safety endpoints and will be measured in terms of AEs and SAEs throughout the clinical trial.
Ethical ApprovalThe study will be performed in accordance with ethical principles that are consistent with the Declaration of Helsinki, the International Conference on Harmonization’s Good Clinical Practice. Informed consent will be obtained from all the included patients before study initiation. This study has been registered on ClinicalTrials.gov (NCT06110910).
Data Collection and Follow-upData from retrospective-prospective cohorts and prospective cohorts will be collected from patients after signing the informed consent form. Medical history related to the SS, diagnosis, information on previous use of any GH for the treatment, any medical history related to diagnosis and treatment of other organ system disease should also be considered. Further, birth length, weight, gestational age and feeding status, history of craniocerebral tumors along with the history of head radiotherapy will be assessed. Family history related to SS, tumors, diabetes mellitus, cardiovascular diseases, pregnancy-related information of the mother of the patient along with the height of the patient’s parents will also be evaluated. Eligible patients will be evaluated, and clinical characteristics during pre and post treatment will be determined along with physical examinations including height, weight, and Tanner staging. GH stimulation tests (GHD and ISS) will also be performed during the screening and baseline periods. Hematology and biochemistry samples will be collected during the screening, baseline, and follow-up periods, assessed every 6 months. If there is discontinuation of the treatment as a result of the completion of the study or any withdrawal occurs because of any reason a virtual follow-up will be performed every 6 months and the patient will be asked to complete the following documentation: (i) information related to physical examination: height and weight; (ii) adverse events: start and end date, severity of the adverse event, whether the adverse events are PEG-rhGH or rhGH related, regression, or outcome; (iii) concomitant medications: name of the medication should be included, dose, mode of administration, initiation and termination time, etc. Medication record related to the dosage of GH, duration of the treatment and termination of the treatment, maintained during the screening, baseline, and treatment follow-up periods will also be evaluated every 6 months. Reporting of AEs and any concomitant medications used will be monitored throughout the study period and at follow-up visits and even after discontinuation of the treatment. Additional tests will be determined by the researchers on the basis of the patients’ condition.
Data from patients belonging to the retrospective cohort will be retrospectively collected on the first visit if they have been on the PEG-rhGH or rhGH treatment for at least 1 year, and follow-up data will be collected after every 6 months from the start of the study. Data from patients in the retrospective-prospective cohort will be retrospectively collected on the first visit if they have been on the PEG-rhGH or rhGH treatment at the beginning of the study and during follow-up visits after every 6 months. Afterwards, data will be collected prospectively during follow-up visits every 6 months until the patients attain NAH or the end of follow-up. In the prospective cohort, data will be collected at the first visit and every 6 months until the patient reaches NAH or the end of the follow-up. In addition, efficacy and safety evaluations will be performed by local clinical study centers according to the usual practice (Table 1).
Table 1 Study data collectionData ManagementThe principal investigator (PI) plays a crucial role in managing clinical data and trials to ensure the integrity of the study along with the safety of participants. This includes ensuring all study sub-investigators and staff are adequately trained and qualified for data collection, protocol adherence, and institutional review boards (IRBs) communication. Sub-investigators will have the access to electronic case report forms (eCRF), and will be responsible for completing patient’s follow-up visit, entering data into the eCRF, and answering any data discrepancies raised by the data quality control staff.
Patient data will be entered into an eCRF at each routine visit by the investigator or site study coordinator manually. All study visits will be recorded in the eCRF which must be reviewed and signed by the respective investigator or any of their authorized delegates. The data in eCRFs will be monitored by the clinical research associate (CRA) and reviewed by the data manager (DM) from a contract research organization (CRO) to ensure data quality.
In addition, the data cleaning process involves four key roles: CRA, DM, medical monitor (MM), and statistician. (i) CRA will verify the data through source data verification conducted during site monitoring; (ii) DM will design a data validation plan based on the clinical report form (CRF) and the study protocol. This data verification plan will incorporate checks within the eCRF to identify missing data, assess logical relationships, flag outliers (such as vital signs), verify normal value ranges (such as laboratory normal reference values), and ensure proper data formatting (including date and time formats). In addition, the DM will create a data management plan to continuously monitor data quality, update validation checks as necessary according to the response to study progress and address any discrepancies or flagged data promptly to maintain data integrity; (iii) MM will verify the logic of medical data to ensure data accuracy, consistency, and reliability; (iv) the statistician will conduct statistical checks on the data to identify any inconsistencies or issues that may impact the validity and reliability of the data. Any inconsistencies or problems identified will be reported back to the DM for further verification.
This study will primarily focus on analyzing the available data, without specifically addressing missing data. The main analysis of this study will be based on the original data presented in eCRF. During the analysis, methods such as the mixed model for repeated measurements (MMRM), which can accommodate issues related to missing data, may be considered for longitudinal data analysis. If excessive missing data exists in a subject included in the analysis, that subject may be excluded during sensitivity analysis. The sensitivity analyses may include multiple imputation (MI), the last observation carried forward (LOCF), or other methods for supplementary analysis.
Statistical AnalysisThis study will adopt R software Version 4.2.2 or higher for the statistical analysis. Statistical tests will be conducted using the paired t tests or Wilcoxon signed-rank test for growth measurement data, and comparisons will be done before and after the treatment. Chi-square test or Fisher’s exact probability test will be used for categorical variables, and non-normally distributed data will be expressed as median and interquartile range, describing categorical variables using frequencies and percentage. Measurement data will be statistically described as mean ± SD (standard deviation), and missing data will not be included in the analysis of relevant efficacy indicators. P < 0.05 (bilateral) will be considered to be statistically significant. Safety data will be analyzed primarily using descriptive statistics, and chi-square test will be used for the incidence of AE and will be compared between the groups.
Interim and Final AnalysisInterim analysis of this trial will be performed at the end of the data collection from the retrospective cohort of patients’ follow-up. After information is collected from the last patient’s follow-up, final results will also be analyzed.
Comments (0)