This pilot randomized control trial (RCT) was approved by Advocate Aurora Health Institutional Review Board (IRB protocol #00104818) and all patients provided written informed consent. The trial protocol has been previously registered (NCT, NCT06175793) and published.16 Analyses and reporting followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline extension for pilot trials.17
Study Design
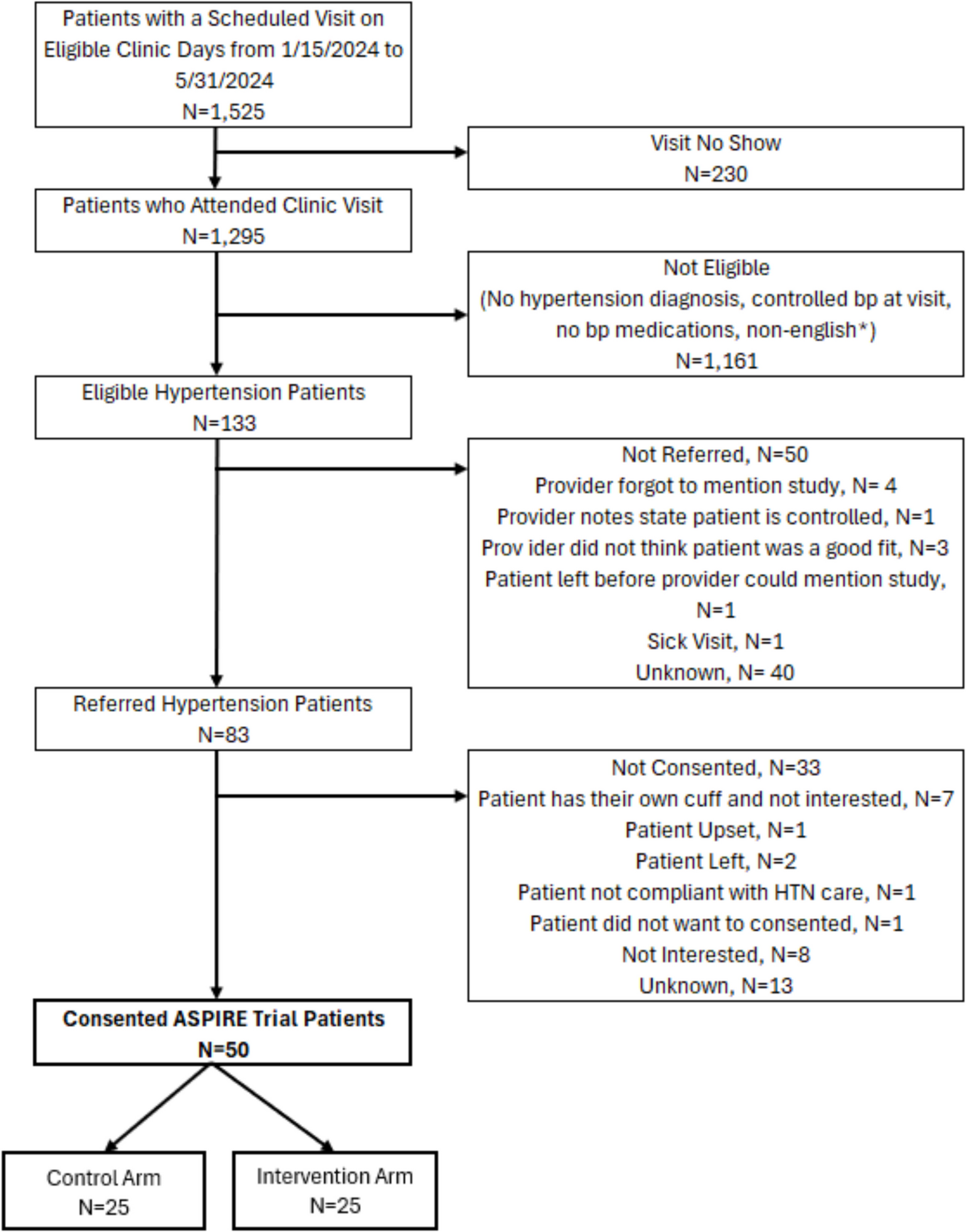
This was a parallel, 2-group unblinded, pragmatic pilot RCT with participants allocated 1:1 to receive a free SMBP device (control arm; n=25) or ASPIRE support which also includes a free SMBP device (intervention; n=25) when eligible patients present to the primary care clinic for a visit with elevated blood pressure. Recruitment of participants occurred between January 5th and May 31st, 2024. Patients were followed for a minimum of 6 months ending on November 30th, 2024.
Patient Eligibility
Eligible patients were adults aged ≥18 years, with a documented hypertension diagnosis using the international classification of disease (ICD-10) code I10, were prescribed ≥1 blood pressure lowering medication, and had an elevated blood pressure reading during the qualifying primary care visit (systolic≥140 mmHg or diastolic blood pressure ≥90 mmHg) documented in the electronic health record (EHR). Patients were excluded if their blood pressure was controlled upon recheck or if they resided in a nursing home or received home health care.
Randomization
The random allocation sequence was generated by the study epidemiologist using SAS (PROC PLAN for assignment of two treatments). Group assignments were sealed in opaque envelopes and opened sequentially by the research assistant to ensure allocation concealment. Randomized patients and the care team were not blinded to the treatment allocation given the pragmatic nature of the trial.
Study Setting and Recruitment
This pilot took place at one primary care site at Advocate Health, a large integrated not-for-profit healthcare system in Illinois. The site is located on the South Side of Chicago and serves a predominantly Black patient population with a median household income of $70,806 and 10.7% (±1.9%) living below the Federal Poverty Level.18 Five internal medicine physicians and their residents serve at this clinic. This clinic was selected because it was part of a system initiative where SMBP devices were offered for free to patients as part of an ongoing donation. According to standard clinic practice, patients diagnosed with hypertension who present with elevated blood pressure during their visit are asked to perform home monitoring. Patients are typically provided with a paper-based log for recording their blood pressure readings. However, standard practice does not include additional SMBP support such as assistance with cuff-sizing, structured training, comprehensive instructions, or systematic follow-up. Additionally, there is no established workflow for documenting SMBP readings within the EHR, leading to inconsistent documentation—readings are variably entered in clinical notes, structured EHR fields, or not documented at all.
A trained research assistant was on site 3 days a week and randomized eligible patients visiting one of these physicians. It was up to the discretion of the physician to invite patients with an elevated blood pressure reading and hypertension medication prescription at the conclusion of their visit to participate in the study. Patients interested in SMBP were escorted to the research exam room to confirm eligibility by the research assistant who then consented and randomized eligible patients. All patients received a SMBP device (upper arm blood pressure monitor HEM-91210 T) from the research assistant after consent and randomization. Patients randomized into the intervention arm additionally received ASPIRE support.
Intervention Arm
Patients received ASPIRE components 1–4 via the research assistant and components 5–6 via a medical assistant who was assigned as the ‘ASPIRE coach’. The ASPIRE coach was an existing medical assistant (MA) designated by clinic leadership to deliver ASPIRE components in addition to their normal workload. A 1-hour training session was conducted to review the ASPIRE components with the MA. At the qualifying visit, patients were (1) fitted with an appropriate cuff size and given a free SMBP device, (2) trained on its use, and (3) provided an ASPIRE log to record 4 daily readings (2 morning and 2 evening) for 7 days. They discussed how to share readings via the patient portal or at a follow-up visit. Additionally, (4) patients completed a short EHR-based social needs questionnaire. Between days 7 and 14, (5) the ASPIRE coach called patients to remind them to share readings and provided resources for identified social needs. (6) A workflow was created to help the coach document SMBP readings in the EHR for care team access.
Control Arm
Patients randomized to the control arm received a free SMBP device per standard practice. There was no training provided on how to use the device and no instructions given by the research assistant on how many readings to take or when. There was no follow up call from the ASPIRE coach to remind patients to take, document, and share readings.
Measurement StrategyFeasibility and Fidelity Outcomes
As a pilot study, our trial focused on feasibility and fidelity outcomes as our primary outcomes outlined a priori using a set of progression criteria in the protocol.16 A full-scale RCT would be deemed feasible if (1) physicians are interested in referring their patients to SMBP measured by the proportion of eligible patients referred), (2) that 50 patients are successfully recruited within the 5-month study period (recruitment), and (3) ≥80% of consented patients have at least one documented ambulatory blood pressure reading during the 6 months follow up (retention).
Fidelity was assessed using a checklist that the ASPIRE coach completed for each patient. Each of the 6-ASPIRE components was coded as either completed or not completed by the ASPIRE coach for patients in the intervention arm. Details for each component were also systematically documented to ensure that the self-report was accurate.
Secondary Implementation Outcomes
Engagement with SMBP was defined as having at least one SMBP reading documented in the EHR by month 1. Documentation by months 3 and 6 were also explored. The mean number of SMBP readings (among patients who reported at least one reading) at 1, 3, and 6 months was also documented.
Secondary Clinical Outcomes
Clinical outcomes were assessed secondarily to inform the measurement strategy and sample size requirements for a future full-scale RCT. These outcomes included change in systolic blood pressure, blood pressure control, defined as ≤140/90 mmHg, and time to blood pressure control (among patients who reached control) at 1, 3, and 6 months. Medication intensification was defined as any increase in class or dose of one of the blood pressure-lowering medications and was evaluated at months 1, 3, and 6.
We chose to use 140/90 mmHg cutoff for blood pressure control instead of 130/80 mmHg as our target because it aligns with historical hypertension guidelines, allows for consistency with prior studies and datasets and is also the common target across healthcare systems in the U.S.4,19,20 To maximize generalizability and minimize disruptions to clinic workflow, we used EHR documented ambulatory blood pressure readings as they are conducted during routine care, rather than having study-specific procedures. Advocate has standard procedures for measuring blood pressure across clinics, and values are regularly captured using automated devices.20
Data Collection and Follow-up Procedures
Given the pragmatic nature of the trial, we did not collect any data beyond routinely collected EHR data for outcome assessment. Patient clinical and demographic characteristics were obtained from the EHR using the baseline visit. SMBP and ambulatory readings were extracted from the EHR. The EHR for this healthcare system has a distinct field for these two different types of blood pressure readings. Medication intensification was determined using prescriptions documented in the EHR. The dataset generated and analyzed during the current study are not available due the sensitive nature of the data (medical records).
Sample Size and Statistical Analysis
We aimed to recruit 50 patients into this pilot, consistent with recommendations regarding the minimal number of participants required to identify feasibility issues.21 Feasibility outcomes were estimated using descriptive statistics with 95% CIs. Between-group comparison of outcomes followed the intention-to-treat principle and focused on descriptive statistics and exploratory effect estimates with 95% CIs.17 Blood pressure outcomes were calculated using the most recent ambulatory reading documented at 1, 3, and 6 months. At 1 and 3 months we report results only among patients with ambulatory readings during each period. At 6 months, we reported results among all 50 randomized patients. Patients who did not have any readings during follow-up were included in the 6-month analysis and their blood pressure readings were imputed by carrying their baseline reading forward.
To inform the generalizability of our results, we compared the characteristics of randomly assigned patients with those of patients who did not consent to randomization using p-values. All analyses were performed using SAS software 9.4 (SAS Institute Inc, Cary, NC).




Comments (0)