
Remember me

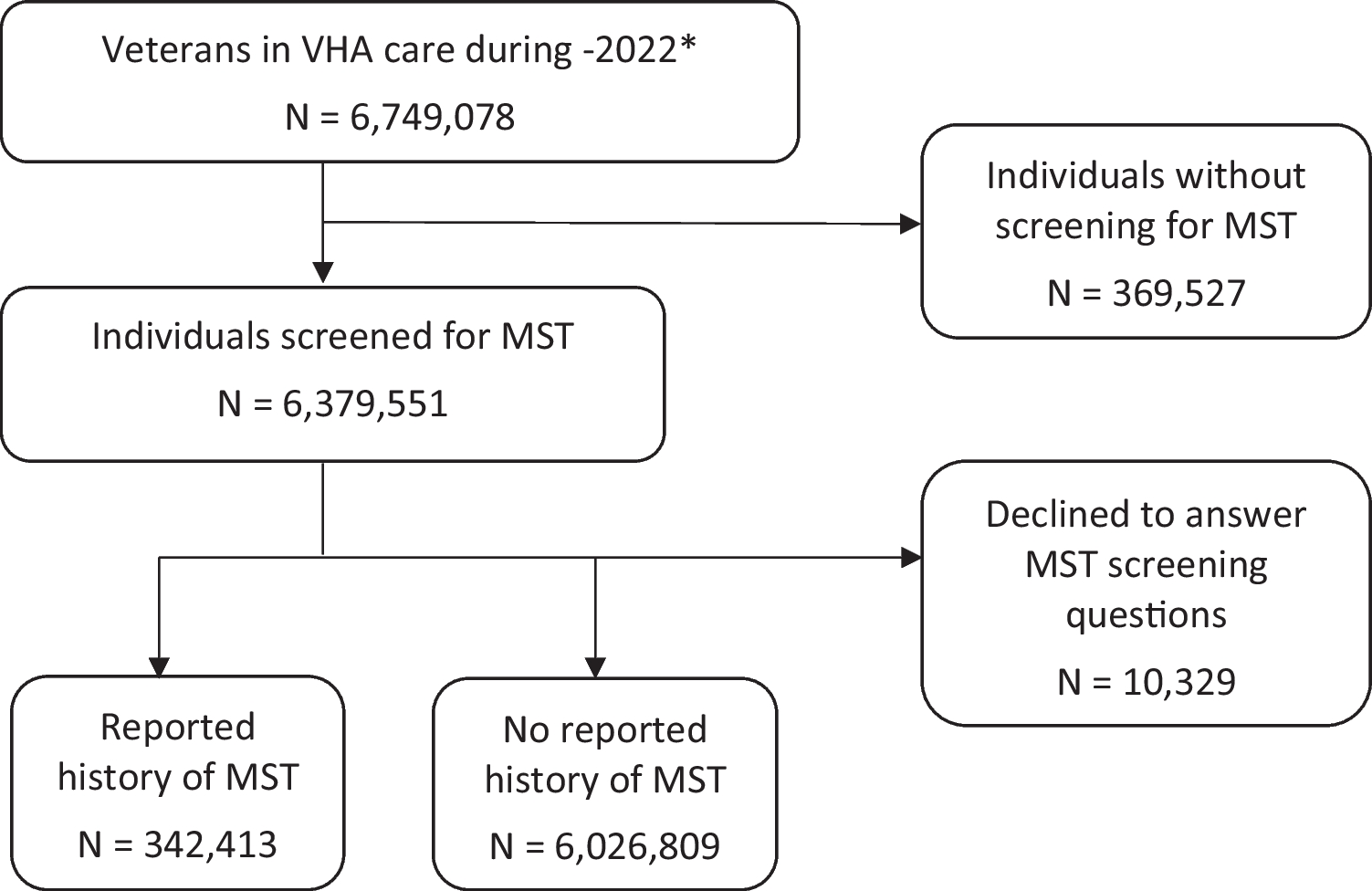


This study was conducted between December 1, 2023, and June 30, 2024. Seventy-three individuals were screened, and 69 (94.5%) were eligible to participate. Fifty participants provided complete responses to the first round, 39 (78%) to the second round, and 43 (86%) to the third round. Forty-eight participants were TGD (96%), and two participants (4%) were cisgender parents of a TGD child. Most participants (86%) were between ages 18 and 44 years old (Table 1).
Table 1 Baseline Characteristics of Participants (N=50)Round 1 ThemesRecruitmentParticipants stressed the importance of a positive relationship between the institution, its simulation program, and the TGD community. They recommended inclusive hiring processes that outline both the monetary and non-monetary benefits and acknowledge the emotional labor involved in SP work. Despite recruitment barriers, participants noted a pool of prospective TGD SPs exists and suggested active outreach by simulation programs. They also identified ethical recruitment sources and methods for TGD SPs.
CastingParticipants recommended that SPs should, whenever possible, share the gender identity of the simulated patient to ensure authentic representation, obtain feedback from SPs with lived experience, and avoid discrimination. Even with an “identical” alignment, consent from the TGD SP to engage in the simulation event is necessary for psychological safety.
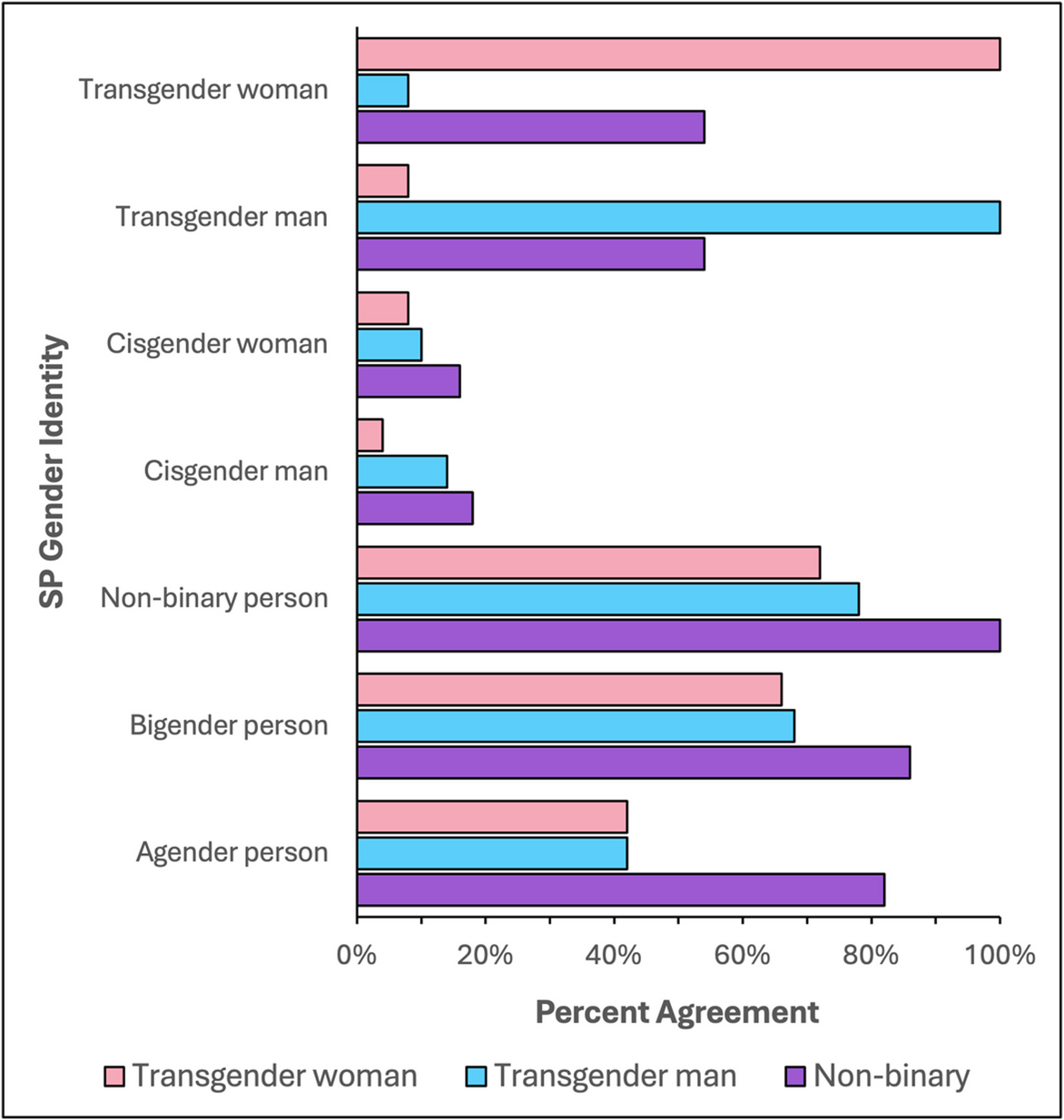
Participants provided insights into acceptable alternative casting decisions when an SP’s gender identity differed from that of the simulated patient (Fig. 1), emphasizing the importance of recognizing the diversity of individual experiences. They acknowledged that TGD individuals “may present in numerous ways depending on the context, safety, [and] experience of the individual’s own gender exploration.” One participant succinctly outlined consensus casting criteria: “Gender dysphoria must be experienced to really understand and react to questioning. Equally important is having experience in being a marginalized social group frequently under attack.”
Figure 1
Quantitative responses on acceptable casting decisions based on a standardized actor’s gender identity to portray a simulated patient identifying as a transgender woman, transgender man, or non-binary individual (SP, standardized patient).
Transgender Men and Women PortrayalWhen an SP’s gender identity did not match the role, they recommended preferentially casting TGD individuals based on matching sex assigned at birth. For example, transfeminine individuals—a term inclusive of a range of gender identities of persons assigned male at birth (AMAB) who identify with a feminine gender experience, either wholly (usually transgender women) or in part—were preferred over TGD individuals assigned female at birth (AFAB) to portray a transgender woman as “they are more likely to understand [their] struggles and concerns.”
Cisgender representation was generally unacceptable due to concerns that the lack of lived experience could lead to “inaccuracies of reaction and demeanor” and stereotyped portrayals during simulation encounters. As one participant reflected, “Being trans is not a costume that someone can put on and take off at will.” Another participant drew a comparison to other minoritized groups, asking, “Do white persons portray Black persons? If so, they should not. There is a lived experience that cannot be trained.” However, participants were more accepting of this practice if the simulated patient’s gender identity matched the cisgender SP’s sex assigned at birth. For example, one participant noted that cisgender and transgender women “face many similar societal issues” that inform their portrayal. Moreover, “engaging in this labor may cause further harm to minoritized individuals, potentially necessitating the use of individuals from other backgrounds or identities.”
Participants strongly opposed casting transgender men as transgender women and vice versa, due to lack of lived experience and potential psychological harm, including worsening gender dysphoria.
Non-binary PortrayalRecommendations were like those for transgender individuals. Importantly, participants indicated high acceptability of casting of transgender men, transgender women, bigender, and agender individuals. Bigender describes an individual who identifies with two genders, either at the same time or at different times, whereas agender describes individuals who do not identify with any gender.
Two-Spirit PortrayalTwo-Spirit is a culturally specific identity used by some Indigenous people in North America to describe a person who embodies both masculine and feminine spirits, or who holds a distinct gender or social role within their community. Participants emphasized that casting for Two-Spirit individuals should be considered separately due to intersectional considerations, cautioning that simulation programs “should be mindful of cultural appropriation.” They recommended restricting Two-Spirit roles to Two-Spirit SPs, with participants acknowledging their own lack of lived experience, as one participant indicated: “Could I, as a transgender woman, accurately portray a Two-Spirit person? I don’t think I could. I don’t [...] know what etiquette or pronouns a Two-Spirit person deems important.”
Cisgender PortrayalMost participants recommended against casting TGD SPs as simulated patients who were explicitly identified as cisgender. This practice could harm SPs’ psychological safety and trigger gender dysphoria.
Case ModificationsParticipants provided insights on how common medical simulation variations, such as manikins, videoconferencing software, and simulation case content, might affect appropriate portrayal. They advocated against altering casting decisions based on simulation modality. They also suggested best practices for affirming TGD SPs when voicing manikins and using videoconferencing software.
While most participants agreed that casting restrictions could be relaxed for simulations unrelated to gender-affirming care, a sizeable minority (26%) argued that all patient care for TGD SPs is inherently gender-affirming care and requires inclusive communication and respect. To illustrate their perspectives, nine participants referenced a scenario involving a TGD patient presenting with a broken arm. Some viewed this case as unrelated to gender-affirming care and appropriate for portrayal by a cisgender SP. As one participant noted, “You don’t need to know what [organs] I was born with to put my arm in a sling.” Others challenged this framing, invoking concerns related to “trans broken arm syndrome,” a term used in the medical literature to describe situations in which a transgender patient’s gender identity is inappropriately centered during unrelated clinical encounters.17 In this context, a cisgender SP “may not accurately identify where a learner is inappropriately focused on a trans identity in this scenario, as they may believe this is routinely how doctors may need to treat trans patients.” Finally, participants emphasized that even scenarios that appear neutral may involve gender-affirming care depending on the educator’s learning objectives: “If you need to train people how to treat a TGD individual who may be suffering a breakage that could be due to osteoporosis that may or may not be down to their estrogen medications being off[,] then it does matter.”
SupportAlthough the questionnaire included an item on optimal training for cisgender SPs portraying TGD simulated patients, participants expressed low acceptability for this practice. A qualitative evaluation of responses showed that 14% of participants firmly recommended against this practice, 24% conditionally recommended against it, and 62% conditionally recommended in favor of it, provided specific training and limitations were in place. Lack of acceptability was driven by several concerns, including an absence of lived experience among cisgender SPs, inauthentic and uninstructive experiences for trainees, and potential offensiveness to the TGD community. However, many participants also acknowledged the tension between ensuring authentic portrayals and protecting psychological safety. Cisgender representation, some noted, may “prevent potentially harmful labor” for TGD SPs, mitigating the emotional burden associated with repeated participation in simulations.
Given these mixed perspectives, we performed a thematic analysis of the suggested training for cisgender SPs but did not develop formal guideline statements. Key recommendations included mandatory cultural and clinical competency training, screening for transphobia, peer discussions or training by TGD community members, and recommendations against modifying an SP’s voice, appearance, or dress during encounters.
Participants made several recommendations to support TGD SPs before, during, and after simulation encounters. Before a simulation, they emphasized the importance of obtaining informed consent from TGD SPs for the specific case. They also recommended that trainees receive baseline TGD cultural competency training to reduce the risk of psychological harm. This training should cover respectful communication, including how to ask about chosen names and pronouns, basic terminology related to gender identity and expression, and common biases or microaggressions experienced by TGD individuals. Ideally, TGD voices should be included in the training. Participants also suggested informing trainees in advance that they will be working with TGD SPs to increase awareness and reduce microaggressions. During the simulation, they recommended measures to preserve TGD SPs’ agency and psychological safety, such as promising intervention by staff in unsafe situations, allowing optional breaks, and permitting external support members. After the simulation, they advised holding debrief sessions for TGD SPs to process emotions and provide feedback for program improvement as the “most valuable data on how to improve this process is going to come from people who have been through it.”
Round 2The Round 2 questionnaire was developed based on emergent themes from the Round 1 questionnaire and included 49 guideline statements in four domains: recruitment (12 items), casting (22 items), case modifications (5 items), and support (10 items).
RecruitmentParticipants reported nearly unanimous agreement (> 90%) with all guideline statements. However, they cautioned that “institutional trust is necessary” for educational organizations to recruit prospective SPs, particularly in light of the current sociopolitical climate. They acknowledged that while healthcare providers have trusted relationships with prospective SPs, only passive recruitment methods, such as posted flyers, are acceptable to avoid coercion and compromising clinical care by distracting from “sacred provider time.” This item was revised for inclusion in the Round 3 questionnaire.
CastingParticipant agreement with guideline items was largely consistent with emergent themes in open-ended responses from Round 1.
Transgender Men and WomenWe will focus on casting decisions for simulated encounters of transgender women, noting parallel themes for transgender men. Most participants supported casting transgender women as SPs for transgender women patients (94.3%). Dissenting responses emphasized that matched gender identity does not replace the need for case-specific consent, however, particularly in scenarios where “the portrayed patient is experiencing discrimination.” Participants preferred transfeminine individuals as the best alternative portrayal, followed by AFAB non-binary individuals. While most participants agreed that cisgender women could portray transgender women under limited circumstances, a sizeable minority (25%) strongly recommended against this practice under any circumstance. This dissenting group cited the practice as “[dis]respectful to the lived experience” of TGD individuals and “a disservice to the medical professional you’re trying to train.” Participants almost unanimously agreed that cisgender men should never portray transgender women, consistent with Round 1 results.
Based on participant feedback, we combined items describing the casting of cisgender SPs to portray TGD patients, applying narrow restrictions such as the availability of more appropriate casting options and the case context being unrelated to gender care.
Non-binary IndividualsParticipants confirmed high acceptability for casting non-binary, bigender, and agender individuals, as well as transgender men and women, as TGD SPs. They recommended limiting cisgender portrayals based on case content and availability of more suitable SP candidates. Participants also confirmed that casting Two-Spirit individuals should be restricted to those who hold this gender identity.
Cisgender PortrayalFor the prohibition of casting TGD SPs as explicitly cisgender patients, participants reported borderline agreement (63.2%). Most dissenting responses supported allowing this practice if the SP was comfortable, arguing they likely have lived experience with male and/or female gender identities and to reflect equity in bidirectional representation. We eliminated this item from Round 3 due to borderline acceptability and a literature review revealing simulated patients are almost never explicitly identified as cisgender.18,19
Case ModificationsParticipants reported nearly unanimous agreement (> 90%) with all guideline statements. Three respondents noted that simulation manikins typically exhibit binary gender expressions, which may not align with the SP’s gender identity, suggesting the need to consider auditory and visual components thoughtfully. Two respondents cautioned against including simulated patient’s pronouns in videoconferencing software if the TGD SP is uncomfortable with their inclusion.
SupportParticipants reported nearly unanimous agreement (> 90%) with nine of the ten guideline statements. However, the statement about disclosing to simulation participants that SPs are from the TGD community received only 73.7% agreement. Concerns included safety, SP consent, and the belief that such disclosure might diminish the simulation’s value as trainees may not have this information in real-world scenarios. As one participant reflected, “I think [trainees] would be more likely to react honestly if they don’t know [an SP] is trans.” Due to these concerns and potential issues for contracted employees, this item was removed from the tentative guidelines. Participants also suggested expanding SPs’ agency to remove themselves from simulations for safety purposes, and this item was revised for inclusion in the Round 3 questionnaire.
Round 3The Round 3 questionnaire included 8 revised guideline statements in three domains: recruitment (1 item), casting (6 items), and support (1 item). All guideline statements received > 60% agreement by participants.
Recruitment95.2% of participants agreed with the revised item on passive recruitment techniques by trusted healthcare providers. Dissenting responses were qualitatively compatible with the guideline statement.
CastingParticipants’ quantitative agreement with the revised guideline statements regarding transgender women and men was similar to the previous iterations in Round 2. Qualitative responses also remained unchanged. We elected to preserve the revised statements for parsimony as they were in a collapsed form compared to Round 2. Importantly, a stable minority (25%) continued to recommend against cisgender SPs portraying transgender patients under any circumstances, citing the lack of lived experience necessary for appropriate reactions during encounters and the potential offensiveness to the TGD community.
Respondents expressed more favorable agreement with the revised statement on casting transgender men and women to portray non-binary simulated patients, noting that this casting is more appropriate if a non-binary SP is not available.
SupportRespondents reported 97.6% agreement with the revised item enhancing the agency of TGD SPs to end a simulation encounter for psychological safety. The sole dissenting response emphasized the importance of SPs fulfilling their contractual obligations.
Final GuidelineThe final guideline consisted of 44 statements across four domains: recruitment (11 items), casting (19 items), case modification (5 items), and support (9 items). Thirty-nine statements were strong recommendations, and five were conditional (Table 2). In the sensitivity analysis, 38 of the 39 strong recommendations retained their classification, while one was downgraded to conditional. Of the five conditional recommendations, one remained, and four were excluded due to agreement rates falling marginally below the consensus threshold of 60% (range 57.3–59.3%). Excluded items shared a common theme, addressing conditional support for casting transgender individuals with discordant sex assigned at birth or cisgender individuals with matched gender identity, as well as one item related to cisgender portrayal of a non-binary individual.
Table 2 Extent of Participant Agreement with Final Guideline Statements
Comments (0)