This large cross-sectional study revealed that migraine cessation usually occurs within the fifth decade of a woman’s life, with an average cessation age of 49.7 years. The average age at menopause was 50.1, implying a temporal relationship between age at last migraine attack and age at menopause. Cessation of migraine before 60 years of age was reported by > 80% of the participants. However, 46.3% of the women continued to experience migraines postmenopause. This finding suggests that menopause, defined as menstruation cessation, serves as a technical marker of time. However, ovarian function is recognized to not abruptly cease following menopause but gradually decline. The data in this study indicate a gradual decline in migraine prevalence with an increase in the duration since the last menstruation. A recent extensive Norwegian study found that, for women born in the 1930 s to the 1960 s, the age at menopause and the duration between menarche and menopause increased by three years [20]. This extension suggests that women experience cyclic hormonal fluctuations related to the menstrual cycle longer, increasing reproductive life expectancy and potentially impacting the prevalence of migraine.
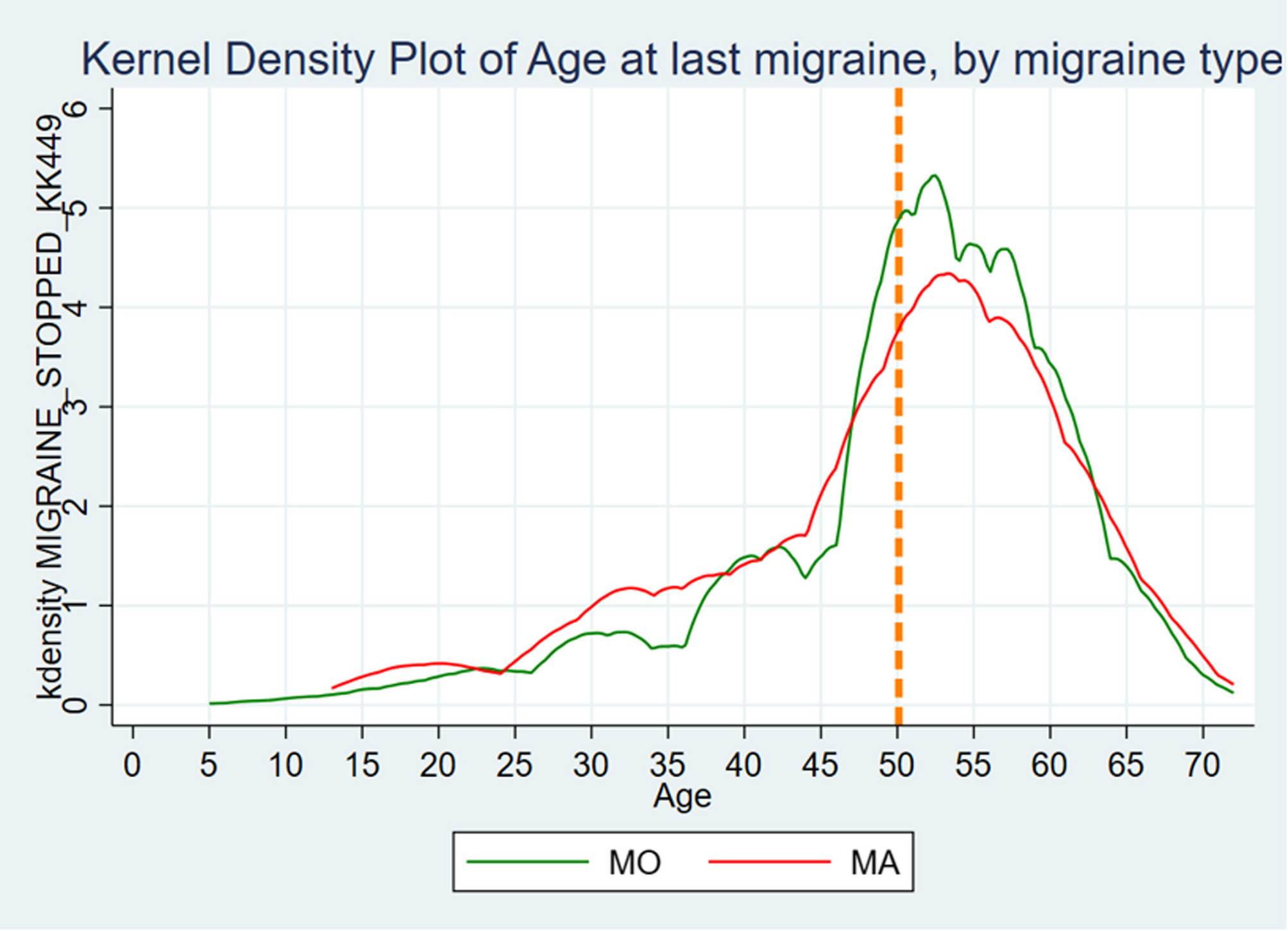
Previous research has documented a decline in migraine prevalence with advancing age [5,6,7] However, to the best of our knowledge, curves showing migraine cessation in relation to the years since menopause (Fig. 5) have not been previously described, nor have the ages of migraine cessation been illustrated (Fig. 4). Figure 4 shows that many of the women continued to experience migraine postmenopause, followed by a gradual decline. This indicates that menstruation cessation does not necessarily equate to migraine cessation.
A recent review has examined the patterns of postmenopausal migraine, where they discovered inconsistent prevalence, ranging from 14.7 to 61.0% [11], underscoring the requirement for larger-scale research to clarify these aspects, as demonstrated in the present study.
In addition, this study separately investigated the onset and cessation of MO and MA. The onset of migraine in women with MA and MO occurs at approximately the same age, although a trend toward earlier onset in those with MA exists. Our data imply that MA occurs independently of menarche more often than MO, as more women with MA experience migraine before their first menstruation. Furthermore, our findings imply that a slight difference may exist between the groups regarding the co-incidence of menopause and migraine cessation, with a tendency toward fewer women with MA (16.6%) than those with MO (18.0%) reporting this. To the best of our knowledge, this finding has not been previously reported. However, this aligns well with the idea that MA is less closely related to menstruation than MO [9, 10].
Our findings on age of migraine cessation align well with clinical experience, and previous studies on age-related migraine prevalence [1, 5,6,7]. Even though menopause has been established, migraine continues in a subset of women as noted in one in five women after the age of 60 years in the present study. This insight is critical for managing migraine and information provided to patients, especially regarding symptoms persistence post menopause. Furthermore, it is relevant because of aging demographics, suggesting that migraine prevalence in mid- and late-life women will increase, causing substantial personal and public health difficulties. Migraine management in older adults may be complicated by factors such as polypharmacy and comorbidities [21].
The results of this study indicate the alterations in migraine prevalence during puberty and the menopausal transition, highlighting the significant role of the maturing and aging hypothalamic-pituitary-ovarian axes. With aging, the neuroendocrine system undergoes substantial changes, including fluctuations in estrogen levels when approaching menopause, and attenuation of negative estrogen feedback loops to the pituitary and hypothalamus. Although shifts in female sex hormone levels reflect hypothalamic alterations, they do not directly cause alterations in the prevalence of migraine. The interplay between cerebral changes and hormonal fluctuations during the menopausal transition may critically affect migraine patterns and presentations across reproductive milestones.
MA without headache is more prevalent in older adults and predominantly presents with visual symptoms [7, 22]. However, this impression may be due to the decrease in MO prevalence in women. The prevalence of migraine in men, both MO and MA, may have less age variation but a higher frequency of non-migraine headaches [9]. Notably, MA and MO in the present cohort seemed to follow a similar pattern of cessation. MA in older adults may be clinically challenging because it resembles conditions such as transient ischemic attacks and epileptic seizures [22].
Strengths and limitations
This study has some limitations. The migraine headache diagnosis and its subtypes were self-reported in a questionnaire rather than confirmed by a physician using the diagnostic gold standard ICHD criteria. However, the questionnaire was derived from the ICHD criteria, which is usually accepted as a valid method for diagnosing migraine, and a similar set of questions based on the ICHD criteria reported sensitivity of 59%, specificity of 99% for lifetime detection of migraine, making it a valid tool for identifying migraine [23].
Moreover, the single question ”Do you have migraine? ‘yes’ or ‘no’ “ has proved to be a valid way of identifying people with migraine [24, 25]; where the “gateway” question in this study is “Have you ever had one or more of the following reoccurring headache conditions– migraine Yes/No”, suggesting that the identification of women with migraine is satisfactory.
In this study, the participants were 34–49 years old at the time of completing the initial questionnaire and 60–74 years old at the time of completing the fourth questionnaire, with migraine questions. Nonetheless, 11.5% (556) of the participants did not report their age at first migraine. This could be due to the differences in perception between childhood and adult migraines, as this may not be recognized in childhood until much later, complicating the determination of migraine onset. Furthermore, 10.8% (332) of the women did not report age at last migraine. Migraine cessation is retrospectively identified based on the time elapsed since the most recent attack. The migraine attack frequency may suddenly or gradually decrease, making it challenging to determine the precise age at which migraines cease. This may have contributed to the missing values. However, few missing values were observed for age at menarche (1.1%, n = 52) and age at menopause (3.4%, n = 162). Additionally, given that some women were not postmenopausal, missing values existed for age at menopause. A total of 194 women were excluded from the analysis because they reported an age at menopause of ≤ 39 years. Premature menopause is menopause before 40 years and has a prevalence of approximately 1% [26]. We consider it unlikely that premature menopause is more than three times more common among women in the present study. Instead, factors such as medical conditions, medication use, use of hormonal contraception causing amenorrhea or misunderstanding the question, are more probable explanations.
When differentiating between MO and MA in the analysis, women were assigned to either the MO or MA group. Women in the MA group reported MA most of the time. The rationale for this subdivision was the lack of sufficient information about separate migraine attacks to classify MO or MA according to the gold standard set by the ICHD-3. Most patients who experience migraine aura likely do so infrequently, with migraine without aura being more common. Thus, the criterion of ‘Most of the time’ may result in an underestimation. Additionally, since aura can occur independently of headache or during the headache phase, the criterion of ‘before headache’ may also lead to an underestimation. Migraine aura is not uncommon [27]. Conversely, many individuals report nonspecific visual disturbances, such as light sensitivity, which they interpret as migraine aura. In conclusion, the criteria of ‘Most of the time’ and ‘Before headache’ are appropriate, as they provide a conservative estimate. Moreover, the prevalence of MA in NOWAC is similar to what you could expect, based on previous research [27].
Some women experience migraine attacks with and without aura. In our study, we did not facilitate analysis in which one woman could be represented on both the MA or the MO group. Due to the lack of data regarding the frequency of migraine attacks with or without aura, it was more appropriate to categorize the women based on the predominant type of migraine attack they experienced. Furthermore, the absence of data on migraine attack frequency precludes the analysis of the differences in migraine frequency throughout a woman’s life or the identification of life stages with increased migraine impact, such as perimenopause. Existing literature shows a heightened impact of migraine during perimenopause, followed by a reduction post menopause [13]; however, the current study could not explore these patterns because data related to the headache characteristics and frequency was obtained only at one time point in the questionnaire.
The women invited to NOWAC were randomly selected from the national population register. However, it has been found that the responders have a slightly higher level of education and on average have more children compared to the general population of Norwegian women, potentially affecting the generalizability of the results. Nevertheless, the prevalence of migraine found in NOWAC is similar to that found in a recent large-scale review [1]. This study’s examination of the general population, as opposed to earlier research that often focuses on selected groups such as headache clinic patients, provides a broader perspective and strengthens the validity of the findings on migraine in postmenopausal women. Furthermore, the large sample size of 4825 women with migraine strengthened the result’s robustness and statistical power. This study may also be subject to recall bias, as it relies on self-reported data from participants regarding their migraine history and other health-related factors, possibly impacting the study’s findings on migraine onset and cessation. Nonetheless, we do not consider it likely to be systematic differences between the MO group compared to the MA group.
One strength of the present study is the possibility of comparing MO and MA. We found few differences between MO and MA; however, women with MA experienced their first migraine slightly earlier and were more likely to continue having migraine after menopause. This suggests that female sex hormones may play different roles in the two subgroups.
Notably, 9.2% of the women experienced their first migraine attack after 50 years of age, a rarely documented occurrence that warrants further investigation.
Significant gaps remain in understanding migraine cessation, especially regarding the prevalence and impact of postmenopausal migraine. Clinical studies rarely include participants aged > 65 years, though previous reviews suggest that migraine attacks tend to decrease in frequency and intensity with age [11]. Future research is required to confirm these observations, expand our understanding of migraine progression in later life stages, and examine whether the type of menopause (spontaneous or medical/surgical) influences the prevalence and course of migraines following menopause. Future research should explore how migraine attack frequency changes across various life stages and identify potential hormonal or lifestyle predictors of (early) migraine cessation. Such studies could aid in developing personalized treatment strategies.




Comments (0)