Study design and participants
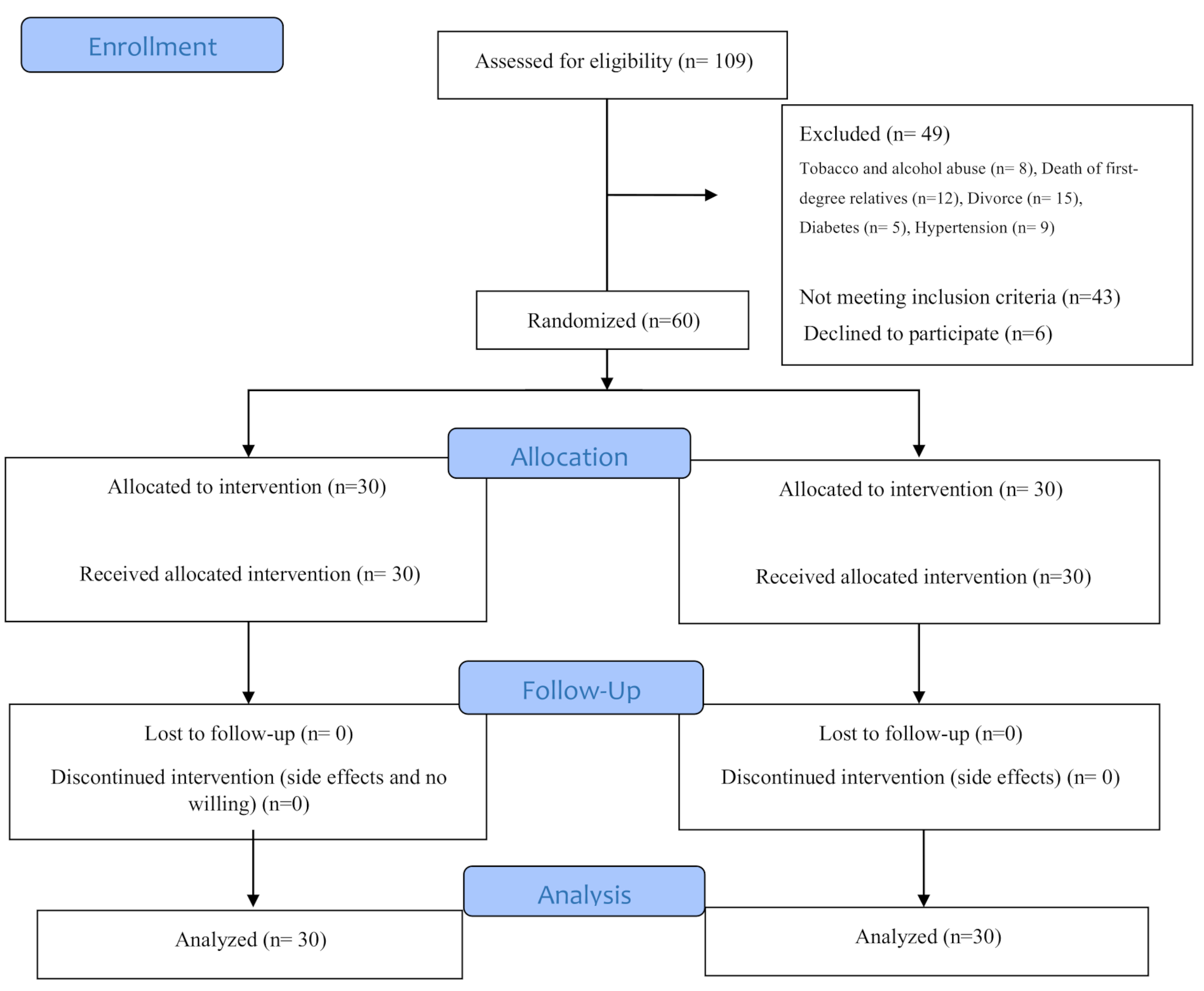
This was a double-blind, randomized clinical trial with two parallel arms. Participants, intervention administrators, care providers, and data collectors were all blinded to the type of intervention received by each participant.
The study population included women diagnosed with panic disorder by the investigator based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-VI) criteria, who attended Sheikh al-Raees Clinic and the psychiatric outpatient clinic at Imam Reza Hospital in Tabriz. Exclusion criteria included substance or alcohol abuse; experiencing a stressful event (such as divorce, death of a first-degree family member, diagnosis of a terminal or hard-to-treat illness in a family member, or job loss) within the past three months; the presence of cardiac, pulmonary, diabetic, asthmatic, gastrointestinal, hepatic, hematologic, or endocrine disorders; and the use of antidepressants, antihistamines, barbiturates, narcotics, diazepam, amphetamines, or cocaine.
Recruitment, randomization, and blinding
The women diagnosed with panic disorder, which is characterized by sudden and unexpected episodes of intense fear or discomfort that peak within 13 min and involve at least 3 of 13 specific symptoms—including increased heart rate, chest pain, sweating, trembling, dizziness, heat sensations, fainting, shortness of breath, choking sensation, nausea, instability, lightheadedness, feelings of unreality or depersonalization, fear of losing control, fear of death, and paresthesia were selected using a convenient sampling method. After careful screening with an inclusion and exclusion criteria checklist, eligible individuals who provided written informed consent were enrolled in the study. Following the baseline assessment, participants were randomly assigned to the sertraline plus propranolol group and the sertraline plus propranolol placebo group, according to the sequential allocation order. Allocation was done using a computer program (www.random.org) with a random block design of four and six blocks, at a 1:1 allocation ratio. To conceal the allocation, opaque and identical glass bottles were numbered consecutively. For each participant, two drug bottles were prepared: one containing sertraline and the other containing either propranolol or its placebo for a 4-week treatment period. Propranolol and its placebo had identical appearance characteristics (shape, color, smell, etc.). The principal investigator (PI) (SR, the first author) conducted participant recruitment and allocation into the groups. A person not involved in the sampling, intervention administration, care provision, or data collection conducted the sequence determination and preparation of the bottles.
Intervention
The study participants underwent treatment that involved sertraline tablets in addition to propranolol or a placebo tablets. Propranolol was prescribed under the brand name Pranol® (Propranolol hydrochloride tablet oral 10 mg). The administration of Propranolol or its placebo began at 10 mg during the first week and was increased to 20 mg starting from the second week. Sertraline was initiated at a dose of 25 mg in the first week, then raised to 50 mg in the second week, and further to 75 mg over the following two weeks. The duration of both medications was four weeks from the start of administration.
Outcome and data collection
The primary outcomes were the frequency and severity of panic disorder, assessed using the Panic Disorder Severity Scale– Self Report (PDSS-SR). The secondary outcomes included depression scores and adverse events.
PDSS-SR is a new self-report diagnostic tool designed to assess panic disorder and monitor the severity of symptoms over the past week. Developed in 2002 by Patricia and colleagues, it consists of seven items that evaluate the frequency of panic attacks, distress during attacks, anticipatory anxiety, agoraphobic fear/avoidance, fear/avoidance of physical sensations related to panic, work impairment, and social dysfunction based on patient ratings. The scale uses a five-point range (0 = “not at all” to 4 = “most severe”), with higher scores indicating greater symptom severity. The total score ranges from 0 to 28 [22]. In the current study, Cronbach’s alpha was calculated to be 0.866.
The Beck Depression Inventory (BDI-13) Short Form was used to measure depression scores. This tool was designed by Beck in 1961, and its short form comprises 13 items that assess the global, behavioral, and cognitive symptoms of depression. Each item features four options, scored from 0 to 3, determining varying degrees of depression, from mild to severe. The maximum score for this test is 39, while the minimum is 0. A score of 0–4 indicates no depression, 5–7 indicates mild depression, 8–15 indicates moderate depression, and 16–39 indicates severe depression [23]. The Persian version of this tool has been psychometrically tested and validated in Iran [24].
A side effect checklist was used to record adverse events during the study. The assessment and follow-up of participants were conducted in two phases: the first assessment was before entry into the study, and the second assessment was 4 weeks after entry into the study. To ensure medication adherence and emphasize its importance, participants were contacted weekly via telephone to remind them to take their medications.
The baseline and sociodemographic questionnaire, Panic Disorder Severity (Self-Report Form), and Beck Depression Inventory were completed through interviews with the participants.
Sample size
The sample size was calculated based on the variable of panic attack severity using G-Power software. According to the results of Forsell et al.s’ study [25] regarding the panic attack severity variable, with M1 = 11.2, M2 = 7.28, SD1 = 4.9, SD2 = 4.7, a two-sided α = 0.05, and 80% power, the required sample size was determined to be 25 participants. Considering a 20% attrition rate, the final sample size was 30 participants per group.
Data analysis
The data were analyzed using SPSS version 26. Independent t, chi-square, chi-square for trend, and Fisher’s exact tests were used to compare the groups regarding socio-demographic characteristics. The normality of the distribution of quantitative data (panic and depression scores) was assessed using the Kolmogorov-Smirnov test. Given the non-normal distribution of quantitative data, the Mann-Whitney U test was used to compare the groups regarding the median of quantitative outcomes. An intragroup comparison was performed using the Wilcoxon Signed Ranks Test. All analyses were conducted based on an intention-to-treat approach. A p-value of < 0.05 was considered statistically significant.





Comments (0)