
Remember me



A total of 175 BPD patients were included in the study, with a mean gestational age of 25.3 (SD 1.3) weeks. Of the patients included, 84 patients (48%) had pulmonary hypertension demonstrated on at least one echocardiogram. There were no significant differences between sex and gestational age between the two groups (P = 0.32 and P = 0.28, respectively). The PH group had a significantly lower average birth weight as compared to those patients without PH (677.1 g vs. 771.6 g, P = 0.0006) as shown in Table 1.
Table 1 Demographics of infants by presence of pulmonary hypertensionPatients with PH had a longer median length of initial stay in the NICU (109.5 days with IQR 78.0–142.0 vs. 88.0 days with IQR 62.0–106.0, P = 0.002) and were intubated for a longer period of time (57.0 days with IQR 33.0–75.0 vs. 32 days with IQR 15.0–56.0, P = 0.0005) as compared to patients without PH. In addition, patients with PH were more likely to require respiratory support with an oscillator (65.5% vs. 37.4%, P = 0.0002).
Patients with PH were more likely to undergo tracheostomy prior to discharge from the NICU as compared to patients without PH (20.2% vs. 8.8%, P = 0.03). The rates of co-morbidities of prematurity, IVH, NEC, sepsis, and ROP were not significantly different between the two groups (Table 2). A PDA was present on at least one echocardiogram in 77.3% of patients with PH and 64.5% in those without PH, which was not statistically significant. Patients with PH and the presence of a PDA were more likely to have surgical closure of their PDA as compared to patients without PH (83.0% vs. 50.0%, P = 0.004).
Table 2 Pulmonary vasodilator medication use during NICU hospitalizationOf patients with PH, 52 (47.6%) patients received pulmonary vasodilators during their NICU admission. Most patients only received one pulmonary vasodilator (N = 36). The most common pulmonary vasodilator used was inhaled nitric oxide (iNO) (38/52 patients). Of the 38 patients that received iNO, 13 patients also received sildenafil (34.2%), while 25 patients received iNO alone (65.8%). The second most common pulmonary vasodilator used was sildenafil (27/52 patients) (Table 3). Of the 52 patients receiving at least one PH medication, 27 (51.9%) patients were started on an additional medication of either a PDE5 inhibitor, prostacyclin, or endothelial receptor antagonist while hospitalized in the NICU, and 88.9% of those patients were discharged home on a pulmonary vasodilator. The median duration of pulmonary vasodilator medication use (excluding iNO) was 335.0 days. The median duration of pulmonary vasodilator medication use (excluding iNO) after NICU discharge was 205.0 days.
Table 3 Co-morbidities of prematurity and NICU course of infants by presence of pulmonary hypertensionOf the 84 patients with PH demonstrated on at least one echocardiogram, 73 patients had data available to determine the timing of PH resolution based on echocardiogram findings. The median time from initial PH diagnosis to resolution on echocardiogram was 59.0 days. There were 32.9% (N = 24) of patients that still had PH on their echocardiogram prior to NICU discharge. Of the patients who had PH by the time of NICU discharge, 91.7% (N = 22) showed PH had resolved on echocardiogram by 1 year, one additional PH patient resolved by 3 years, and the last PH patient had resolved by 5 years after initial NICU discharge.
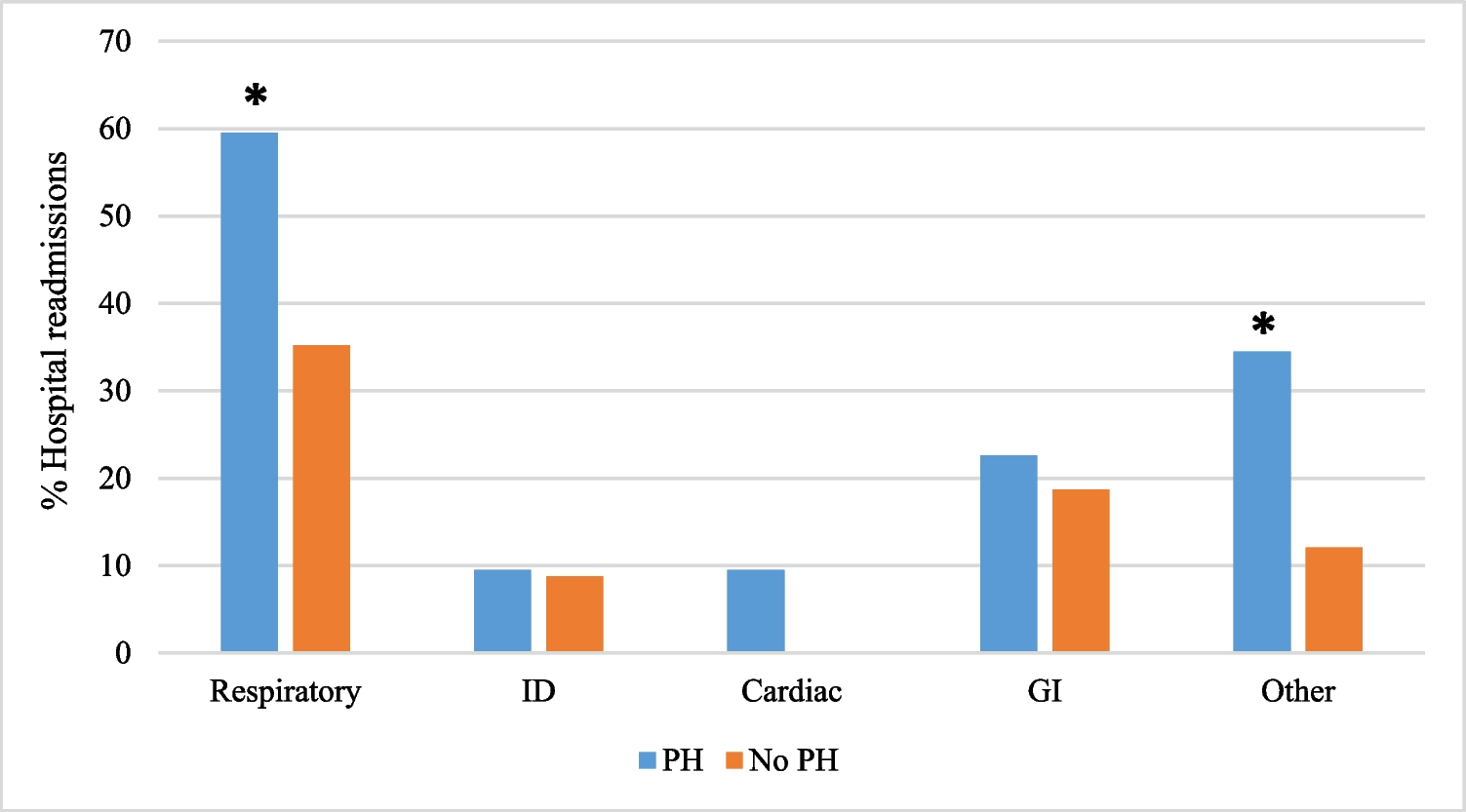
During a 5-year post-NICU follow-up, patients with PH on echocardiogram at any time were more likely to require repeat hospitalization after initial discharge compared to patients without PH (71.4% vs. 48.4%, P = 0.002). Patients with PH also had a significantly higher median number of re-admissions per patient (2 with IQR 0–6 vs. 0 with IQR 0–2, P < 0.0001). Of the patients with at least one hospitalization, patients with PH had a higher median (IQR) number of hospitalizations (4 with IQR 2–8 vs. 2 with IQR 1–4, P = 0.0006). In addition, the median number of days from initial hospital discharge to first re-admission was significantly shorter for patients with PH (53.5 with IQR 15.5–145.4 vs. 155.5 with IQR 42.0–331.0, P = 0.03) (Table 4). Patients with PH were more likely to require hospitalization for respiratory, cardiac, and “other” reasons (Fig. 1). However, the percentage of patients with PH who had any ED-only visits was not significantly different compared to patients without PH (79.8% vs. 75.8%, P = 0.53). Additionally there was no significant difference between the median number of ED visits between the two groups (6 with IQR 3–12 vs. 5 with IQR 2–9, P = 0.47).
Table 4 Hospitalizations by presence of pulmonary hypertensionFig. 1
Reasons for hospital readmissions for infants by the presence of pulmonary hypertension. * indicates statistical significance with P < 0.05. Note: hospital readmission for cardiac reasons was not noticed in the subjects with no PH
Patients with PH had a significantly longer median (IQR) duration of home oxygen use as compared to patients without PH (189 with IQR 121–276 vs. 134 with IQR 98–250, P = 0.02). There was no significant difference in death at 5 years’ follow-up between the two groups (4.8% vs. 4.4%, P > 0.9).
Comments (0)