
Remember me




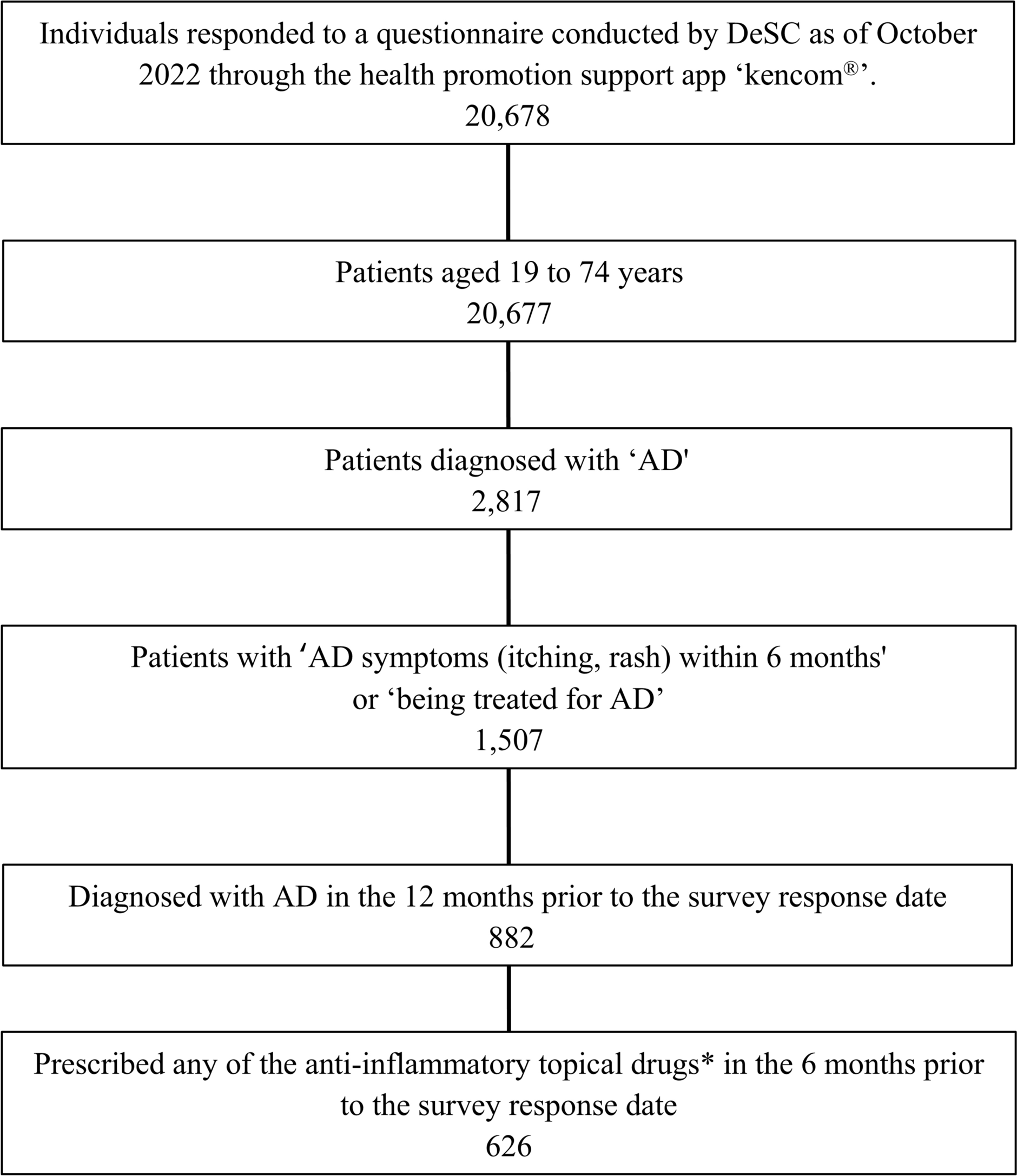
Our search strategy identified 2532 unique citations (Fig. 2). Following title and abstract screening, 187 full text records were assessed for eligibility, and 37 studies were included; 17 of the studies assessed skin microbiota, while 21 of the studies assessed microbial-targeted therapies.
Fig. 2
Flow diagram of study selection
Skin Microbiome CompositionPatient DemographicsWe identified 17 references out of the total 37 studies included that assessed skin microbiota comprising data from 642 patients with CTCL. There was a higher proportion of male sex (57.6%, n = 370) compared to female sex (42.4%, n = 272) represented, although the degree of male sex predominance was lower than previously reported rates [3]. Six studies reported race or ethnicity, with the majority of participants identified as Caucasian/White (n = 193), followed by Black/African American (n = 47), and patients characterized as “Other” (n = 4). Representation from certain global regions such as Asia and South America remains limited in the literature, yet an increased frequency of CTCL was reported within these groups when compared to other parts of the world [28]. Of the studies that reported disease staging, microbiome composition was more frequently assessed in early-stage disease (IA–IIA, n = 391) than in advanced-stage cases (IIB–IVB, n = 169).
Microbe Analysis MethodsAmong microbial domains, bacteria were the most frequently studied (15 of 17 studies), followed by viruses (6 of 17 studies) and fungi (3 of 17 studies) (Fig. 3a), reflecting the predominance of bacterial species in skin colonization [10]. Broad sequencing approaches including whole-genome/metagenomic sequencing were used in four studies, while targeted methodologies including standard culture, PCR or RT-PCR, 16S rRNA sequencing, and molecular histopathology were employed in 13 studies (Fig. 3b). Furthermore, usage of greater resolution and comprehensive methods tended to increase in studies published from 2020 onwards.
Fig. 3
An overview of the characteristics of studies assessing the skin microbiome in CTCL and antimicrobial therapeutic outcomes. a Pie chart demonstrating the proportion of studies included that analyze bacterial, viral and fungal compositions in patients with CTCL. b Figure depicting the change in skin microbiome assessment techniques in the field of CTCL. The number of studies using the assessment techniques is graphed to the year the study was published. c An overview of the prominent bacteria, virus, and fungi that were studied across the studies included. Bar charts indicate the number of studies that analyze each microbial taxa and whether they reported a significant increase, decrease, or no change when comparing lesional skin of patients with CTCL to non-lesional skin or healthy controls. d Pie chart demonstrating the proportion of studies included that assess the use of antibiotics, antivirals, antifungals, and direct decolonization techniques of the skin in patients with CTCL. CTCL cutaneous T cell lymphoma
Sites of skin sampling were inconsistent both within and between studies; swabs were obtained from various anatomical locations including head and neck, arm, axillary, trunk, back, buttock, thigh, leg, and foot. Given the well-characterized site-specificity of the skin microbiome, this variability could contribute to interstudy heterogeneity [29].
Skin Microbiota CompositionA culture-based assessment of the skin microbiota by Allen et al. found that 75.4% of patients with CTCL were colonized by S. aureus, with coagulase-negative Staphylococcus (CoNS) and Corynebacterium spp. representing the next most frequent taxa [30]. This is quite striking as S. aureus only colonizes 20–30% of nares in the general population and its presence on healthy skin is typically minimal or transient [31, 32]. Other detected genera included Pseudomonas and Klebsiella, although at a lower prevalence [30]. The predominance of potential pathogens may reflect microbial dysbiosis observed in the patients with advanced-stage CTCL within their study.
S. aureus was the most frequently examined species across all studies, likely due to its proposed role in CTCL pathogenesis. However, findings were inconsistent. Some studies reported increased S. aureus abundance in CTCL lesional skin, while others determined no difference compared to healthy controls or non-lesional skin (Fig. 3c). When analyzing intra-patient comparisons of lesional and non-lesional skin, three out of six studies suggested S. aureus enrichment at lesional sites [33,34,35,36,37,38]. One study by Olesen et al. did not report significant differences in microbiome composition between lesional and non-lesional skin; however, when data were stratified by MF, folliculotropic mycosis fungoides (FMF), and SS subtypes, variations in S. aureus abundance were shown [37]. In contrast, when the skin microbiome of patients with CTCL was compared to healthy, age- and sex-matched controls, no significant differences in S. aureus were observed [32, 39, 40]. Although Nguyen et al. reported a trend towards greater S. aureus abundance in CTCL lesions (P = 0.07), the association did not reach statistical significance as a result of a limited sample size [40]. A possible increase in lesional S. aureus burden with advancing disease stage was noted, though few studies formally evaluated this [34, 40]. As more than two-thirds of patients studied had early-stage disease, and dysbiosis is likely more pronounced in advanced stages, larger cohorts of late-stage patients are warranted in future studies.
Other bacterial genera noted by the literature include Corynebacterium and Cutibacterium spp. Corynebacterium was more prevalent in lesional skin, while Staphylococcus epidermidis and Cutibacterium acnes were less prevalent in lesional skin. Harkins et al., in contrast, observed no significant changes in S. aureus but did report increased CoNS colonization in patients with CTCL [32]. Intriguingly, Borrelia burgdorferi DNA was detected in lesions and hypothesized to serve as a potential antigenic driver of lymphomagenesis in two Italian studies [41, 42]. One study evaluated Chlamydia pneumoniae but found no evidence supporting an etiopathogenetic role in MF [43].
Bacterial signatures associated with narrowband ultraviolet B (nbUVB) treatment response was also explored [44]. Phototherapy responders exhibited elevated baseline Staphylococcus across lesional and non-lesional skin, with Staphylococcus capitis and Staphylococcus warneri enriched in lesions. Following nbUVB, responders showed increased Streptococcus and Acinetobacter in lesional skin, accompanied by a decreased abundance of S. aureus. These findings suggest that distinct microbial profiles may be associated with phototherapy responsiveness.
From a viral perspective, Epstein–Barr virus (EBV) was identified in some reports to be a possible risk factor, with studies indicating increased viral load in MF lesions [45, 46]. Another German study reported high human T cell leukemia virus type 1 (HTLV-1) prevalence in lesional skin [41]. Fungal data were sparse, and no consistent trends in fungal colonization were reported across studies when comparing lesional, non-lesional, and healthy skin.
Microbial-Targeted TherapeuticsPatient DemographicsWe identified 21 studies out of the 37 studies included that evaluated the outcomes of microbial-based therapy in patients with CTCL, comprising a total of 231 individuals. Among these, 46.8% (n = 108) identified as female and 53.2% (n = 123) as male. Eight studies reported patient race or ethnicity, with most individuals identified as White (n = 90), followed by Black (n = 51), Hispanic (n = 8), and Asian (n = 1). There was a predominance of advanced-stage disease with 136 patients with stage IIB–IVB disease compared to 88 patients with early-stage IA–IIA disease. This predominance likely reflects antimicrobial use in refractory CTCL, where barrier disruption and immune dysregulation heighten microbial dysbiosis and infection susceptibility.
Antimicrobials UsedPatients were treated with a wide range of antiseptic treatments, antibiotics, antifungals, and antivirals (Fig. 3d). Antiseptics included baths containing 0.4% chlorhexidine gluconate [47]. Mupirocin 2% was frequently employed for skin decolonization. Commonly reported systemic antibiotics included clindamycin, ampicillin, dicloxacillin, ciprofloxacin, and doxycycline; doxycycline was commonly selected for both its antimicrobial and anti-inflammatory properties. Vancomycin was reserved for severe infections and/or very ill patients, particularly in hospitalized cases or those with ulcerated tumors [47,48,49,50]. The various antimicrobial regimens were mainly driven by conventional culture-based sensitivities, unless the study was interventional in nature. Itraconazole was frequently administered for suspected opportunistic fungal infections, which were prevalent in patients with CTCL [51,52,53]. Antifungal and antiviral agents were typically introduced in the setting of documented co-infections. Most patients were already receiving CTCL-directed therapies at the time of antimicrobial administration, such as phototherapy, radiation therapy, methotrexate, interferon, brentuximab, oral retinoids, chemotherapy, topical corticosteroids, or immunomodulators (e.g., topical imiquimod).
Patient OutcomesSeveral cases illustrated the therapeutic synergy between antimicrobials and CTCL-directed treatments, particularly for fungal involvement. In one report, orally administered itraconazole alone failed to clear tinea corporis in a patient with recurrent infections [52]. However, once a biopsy confirmed patch-stage MF, concurrent treatment with orally administered itraconazole, methoxsalen, and ultraviolet A phototherapy resulted in fungal clearance and sustained MF remission [52]. Similarly, in a patient with CTCL and refractory fungal infection, resolution occurred only after switching from leukocyte to lymphoblastoid interferon alongside itraconazole, resulting in improvement of both fungal burden and CTCL lesions [51]. Such findings suggest a complex interplay between fungal colonization, CTCL therapeutics, and disease activity.
This pattern of CTCL regression coinciding with resolution of microbial colonization or infection also extends to bacteria. The aggressive and transient treatment with antibiotics decreased clinical symptoms in advanced-stage CTCL [21, 54]. Chi et al. described a patient with stage IVA pustular MF who received vancomycin in the context of S. aureus-driven sepsis, leading to improvement of their MF lesions [48]. A similar phenomenon was reported in a patient with neoplastic lesions infected with Corynebacterium striatum, where penicillin therapy reduced erythema and purulence, and complete regression of MF occurred following subsequent chemotherapy [55]. Additionally, one study showed that mupirocin 2% ointment and systemic antibiotics targeting S. aureus colonization led to objective improvement on cutaneous examination in 58% of patients with all stages of MF/SS [23]. Collectively, these observations suggest that microbial pathogens may exacerbate disease activity, even if they are not direct oncogenic drivers.
Antimicrobial therapy alone conferred benefit in select cases. 1% Gentian violet resulted in a sustained partial response in a patient with early-stage MF that failed nbUVB, topical corticosteroid, and retinoid treatments [56]. A patient with rare zosteriform MF was treated empirically with valacyclovir in the absence of virologic confirmation, leading to resolution of her lesions [57]. Interestingly, she experienced a recurrence of MF upon cessation of antivirals, and prior treatments, including triamcinolone acetonide 0.1% and bexarotene gel, were ineffective [57]. In another case series, antibiotic therapy directed against Enterococcus species without concurrent CTCL treatment led to healing of ulcerated tumors with eschars in some reports [58].
Notably, four studies highlighted positive outcomes for antimicrobial therapy in erythrodermic CTCL [23, 47, 49, 59]. Talpur et al. demonstrated that 50% of patients with erythrodermic CTCL and S. aureus colonization had dramatic reduction in their BSA with oral antibiotic treatment [23]. One patient with SS and an erythrodermic flare showed pronounced mSWAT improvement following IV vancomycin and cefepime, in combination with bleach baths of 15 mL chlorhexidine gluconate 0.4% and topical corticosteroid wraps [47]. Another analysis of 26 patients with erythrodermic CTCL demonstrated BSA and mSWAT improvement following antibiotic regimens targeting S. aureus in approximately 50% of the cases [49]. In Purnak et al., most patients with advanced-stage CTCL received long-term antibiotic therapy and antibiotics were suggested to improve or clear erythroderma [59].
However, antimicrobial therapy did not universally yield clinical benefit [60,61,62]. Panasiti et al. described a case of progressive MF with ulcerated tumors that grew CoNS but did not respond positively to antibiotics [60]. However, this may align with the hypothesis that critical colonization with specific bacteria like S. aureus modulates CTCL disease, rather than mere bacterial colonization itself. Another case described stage IB MF lesion progression despite clearance of Trichophyton rubrum dermatophytosis [61]. In a comparative study, doxycycline was found to be significantly less effective at reducing mSWAT, Composite Assessment of Index Lesion Severity, and histopathological scores relative to psoralen + ultraviolet A light in early-stage disease after 12 weeks [63]. Doxycycline only mildly attenuated disease when used alone [63, 64].
Lastly, prophylactic antibiotic use was variably effective and was associated with complications. Secondary infections were common, with some cases progressing to bacteremia or death from resistant pathogens [30, 58]. For example, Tsambiras et al. reported an initial tumor response to antibiotics, but recurrent infections and hospitalizations prevented further chemotherapy, ultimately contributing to patient mortality [50]. No clear protective effect of antimicrobial prophylaxis could be determined from the literature, underscoring the need for judicious antibiotic use in the context of rising antimicrobial resistance.
Comments (0)