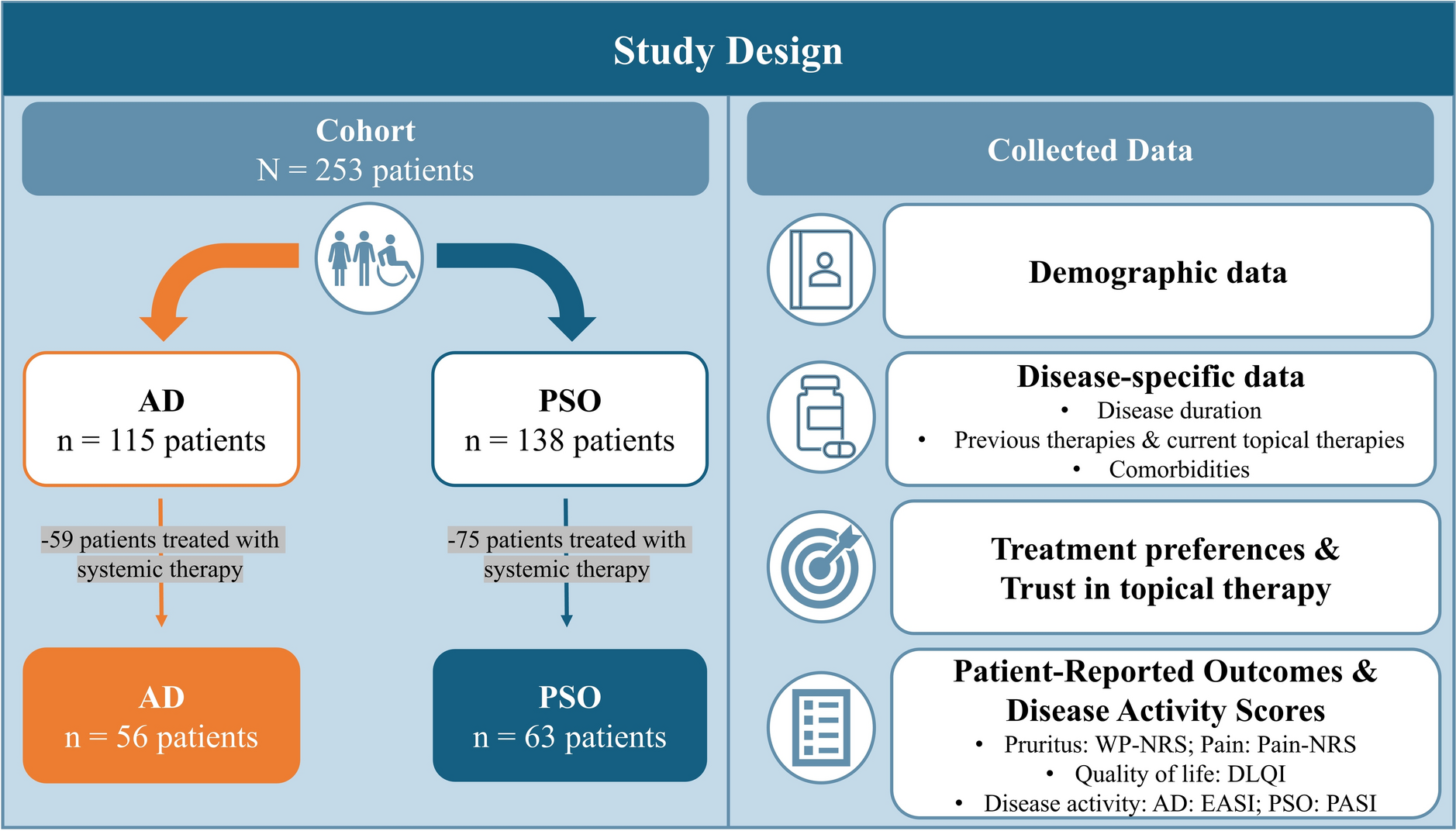
Study Design
This prospective study was conducted at a tertiary academic skin laser center of a university hospital. The study protocol was approved by the Siriraj Hospital Institutional Review Board, Mahidol University, Bangkok, Thailand (Si 025/2024) and was registered at Thaiclinicaltrials.org online registry (TCTR20250317012). Written informed consent was obtained from all participants before entering the study. Written consent to publish participants’ photographs was obtained.
Participant Selection
Thai patients aged more than 18 years old with FSTs III–V, presenting with mixed-type melasma determined by Wood’s lamp examination were considered eligible for the study. Inclusion criteria were as follows: volunteers having bilateral lesions and a modified Melasma Area and Severity Index (mMASI) score with homogeneity, darkness, and area involvement scores at least 2. Patients who were using bleaching creams, had undergone chemical peels, intralesional tranexamic acid injection, and/or laser treatments within the past 6 months, who were pregnant or breastfeeding, and those on orally administered tranexamic acids and/or oral contraceptive pills were excluded from the study. The use of oral or topical treatments for melasma was not permitted during the study period.
On the basis of a prior study [17], we assumed a mean change from baseline to 3 months of 10 and an SDpooled of 15, yielding an effect size of 0.667. With 90% power, a two-sided significance level of 0.05, and a 5% anticipated dropout, the minimum sample size calculated was 28 patients.
Intervention
All participants received three monthly treatments of a 675-nm laser (RedTouch®, DEKA M.E.L.A., Calenzano, Italy). No topical anesthesia was applied prior to the treatment. A thin layer of aqueous, transparent, non-colored gel was applied to the treatment surface before starting the treatment to allow smooth gliding of the sapphire tip of the laser handpiece. The study device emitted a 675-nm wavelength and was equipped with a 15 × 15 mm scanning system with a contact sensor integrated into a water-cooled handpiece, capable of generating fractional micro-zones (DOTs) measuring 0.7 mm in width. Each session employed two laser delivery modes including Moveo and Standard. In Moveo mode, a power of 4 W, dwell time 50 ms, DOT energy of 0.2 mJ, DOT fluence of 52 J/cm2, and 8% density with epidermal cooling of 5 °C was used to treat the entire face by delivering 2000 DOTs per cheek and 500–1000 DOTs to the forehead, depending on forehead size. The handpiece was placed in contact with the skin surface, without excessive pressure, using consecutive, non-overlapping spots over affected areas. Subsequently one pass of a Standard mode was then applied to melasma lesions with a power of 5 W, dwell time of 75 ms, DOT energy of 0.4 mJ, DOT fluence of 97 J/cm2, and 1.7% density with epidermal cooling of 5 °C for all subjects. The therapeutic endpoints were mild to moderate erythema and a mild warm sensation, both lasting several minutes.
No special postoperative care was required. All participants were instructed to use a broad-spectrum sunscreen with SPF 50 and maintain their regular daily activities throughout the study period.
Outcome Measurements
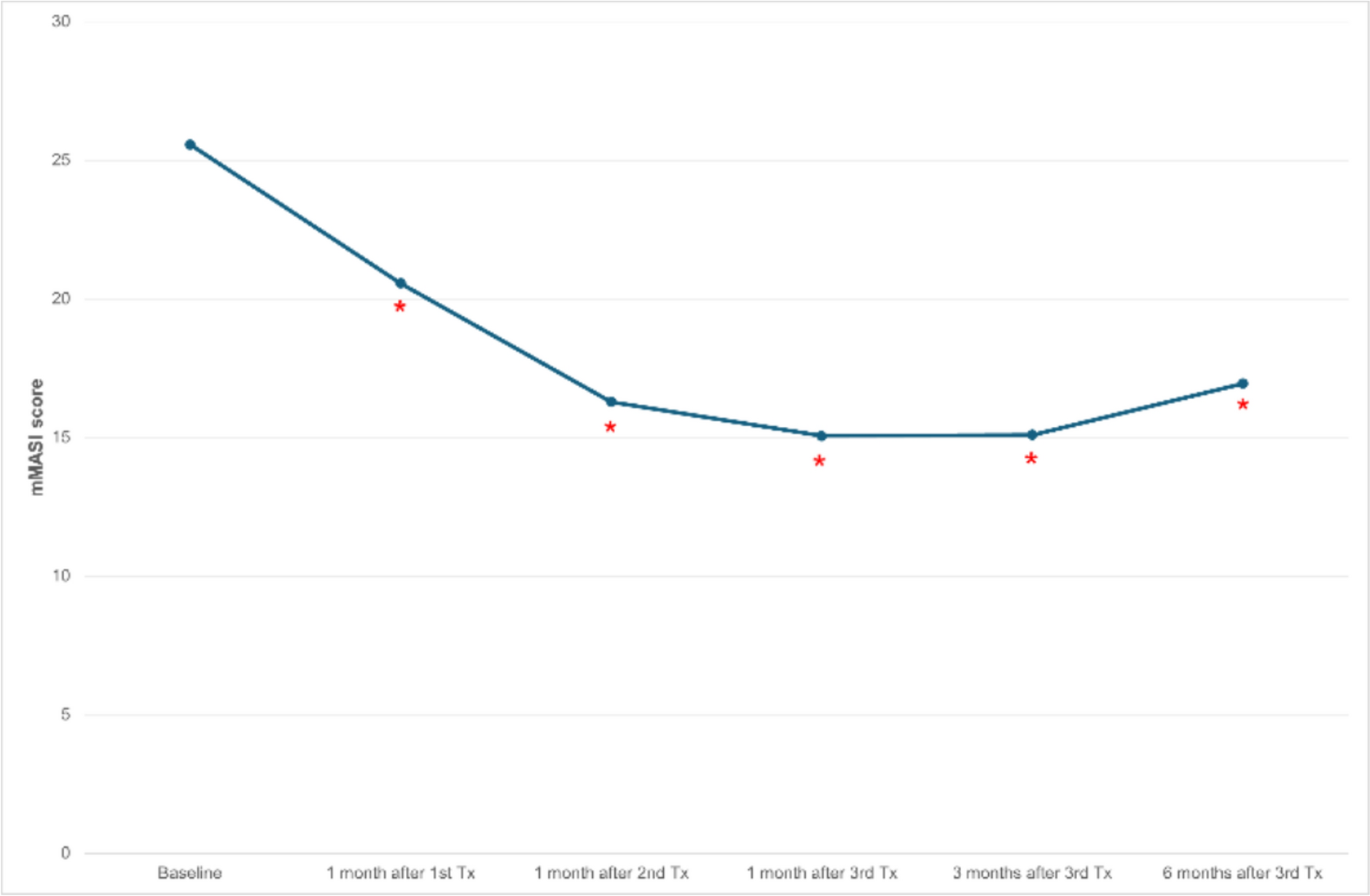
Treatment outcomes were evaluated using both objective measurements and subjective patient-reported outcomes. Assessments were performed at six standardized time points: baseline (prior to treatment), 1 month after each of the three treatment sessions, and at 3 and 6 months after completion of all treatments.
The primary outcome was clinical improvement in melasma severity, measured using the mMASI [19]. This validated scoring system quantifies melasma on the basis of its distribution and intensity across facial regions, producing a composite score derived from the affected area, pigmentation darkness, and homogeneity.
Secondary outcomes included objective assessment of skin pigmentation, along with patient-reported improvement and treatment tolerability. Pigmentation was quantified using a skin imaging device (Antera® 3D CS, Miravex Limited). Measurements were obtained at standardized anatomical sites at each visit and averaged over three consecutive readings to ensure reliability.
Patient-perceived improvement was assessed using the Patient Improvement Scale, a 5-point categorical tool in which participants rated their improvement as 0% (none), 1–25%, 26–50%, 51–75%, or 76–100%. Pain was evaluated immediately after each session using a visual analog scale (VAS) from 0 (no pain) to 10 (worst imaginable pain), with scores recorded separately for the Moveo and Standard modes to compare tolerability. Adverse events and treatment-related side effects were actively monitored and documented throughout the study period.
Statistical Analysis
Changes in outcome measures over time were evaluated using mixed-effects repeated-measures models (REML) to account for within-subject correlations and missing data. Statistical significance was set at a two-sided p value < 0.05. Categorical variables, including patient-reported improvement, were summarized descriptively using frequency distributions.





Comments (0)