Studies have been conducted in Japan to investigate the status of providing instructions for topical medications from pharmacists to patients [10, 11], but few studies have investigated the actual status of topical medications for patients with AD on a nationwide basis.
This study, therefore, aimed to investigate the real-world prescription practices and patient adherence to topical anti-inflammatory agents during the remission maintenance phase of AD treatment.
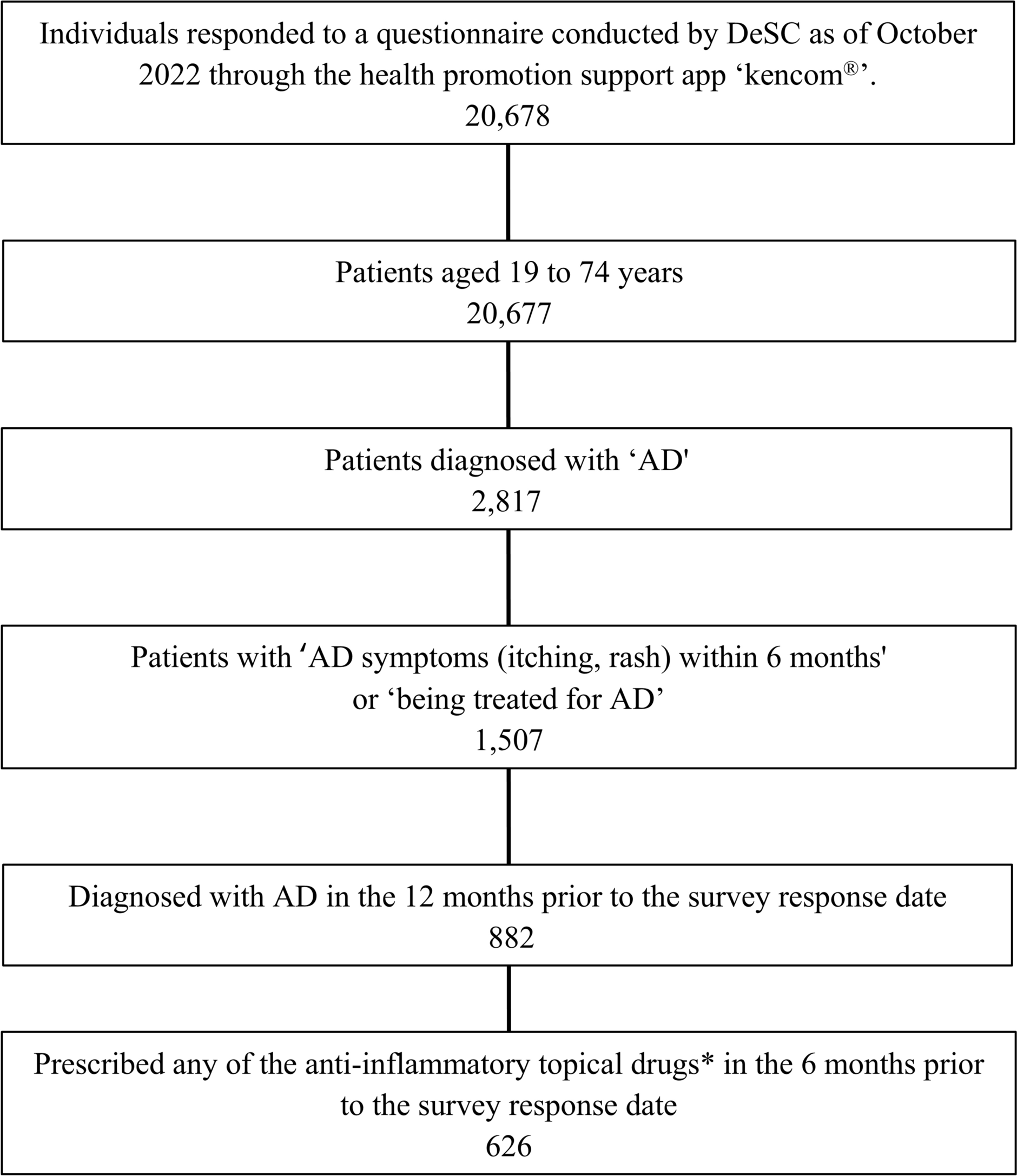
In this study, we evaluated 626 patients who were visiting medical institutions for AD and had been prescribed topical anti-inflammatory agents. We assessed the actual prescription practices (e.g., proactive therapy), and the instructions given by medical institutions regarding dosage amount, application area, and method (“instructions”), and compared them with patients’ actual application behaviors (“actual practice”) and adherence status. The most common type of treatment is reactive therapy, which means stopping the treatment once the eczema improves.
In our study results the majority of cases were those in which the treatment was stopped once the eczema improved, which is generally referred to as reactive treatment. Only about 5% of cases were administered intermittently during the remission maintenance period, which is generally considered to be proactive in the guidelines. There were 11 patients (1.8%) who answered “No” to Question 1 and inconsistently answered that they did not need to apply medication during the remission maintenance phase, which may limit the possibility that the intention of the question was not clearly communicated. Proactive therapy during the remission maintenance phase is considered effective in reducing the recurrence of dermatitis and achieving complete remission, as suggested in previous studies [4, 12,13,14]. Furthermore, its efficacy has been demonstrated in several randomized controlled trials (RCTs) [15,16,17,18]. In a Japanese clinical trial, proactive therapy significantly reduced both the SCORing Atopic Dermatitis (SCORAD) index, which reflects the severity of AD, and the Dermatology Life Quality Index (DLQI), a measure of skin-related quality of life, compared with reactive therapy [18]. However, the results of this study suggest that proactive therapy has not yet been widely adopted in the treatment of AD. Of note, in Japan, topical corticosteroids prescribed by physicians are, in principle, covered by the national health insurance system, whether used for proactive or reactive therapy. Patients are usually responsible for copayment of approximately 30%, with the remaining medical expenses covered by insurance. Therefore, we consider that the low prevalence of proactive therapy is likely to be unrelated to insurance coverage. At present, patients in remission tend to reduce the frequency of outpatient visits for treatment. Because proactive therapy requires regular outpatient visits even after clinical improvement, the proportion of patients receiving it is expected to be low. We believe it is essential to further communicate the importance of proactive therapy, strengthen education, and promote its wider adoption, with the goal of providing better treatment for patients.
As for instructions from medical professionals (doctors, nurses, pharmacists, etc.), for the amount of medication applied, the most common response was “No specific instructions” at 44.2% (Fig. 2), but the amount of application indicated was “FTU” [7, 8] (as described in the Japanese guidelines[1]), “Enough to make skin shiny” and “Enough to make a tissue stick to the skin”, in that order, and for those patients for whom instructions were given, approximately 50% were considered to have received appropriate instructions. Of note, these instructions are intended for healthcare professionals, including doctors, nurses and pharmacists.
The most common amount of anti-inflammatory topical medication actually applied, in the clinical situation where patients conducted self-application was by “FTU” [7, 8], followed by “Enough to make skin shiny”; and “Enough to make a tissue stick to the skin “, and the majority of patients used the appropriate amount of medication, with a combined rate of approximately 70%. Despite “No specific instructions” being the most common instruction. The fact that FTU [19], which is considered the appropriate dosage, is the most frequently used suggests that patients are applying the correct amount based on information from external sources.
Regarding the application area of topical anti-inflammatory drugs, in both of these, “Apply not only to the eczema or remaining inflamed areas, but also to the surrounding areas” considered an appropriate application area was less common than “Apply only to areas with eczema or remaining inflammation”. Regarding the application use method, “Apply thinly” (Fig. 6) was the most common method of application in both instructions provided and the actual status, while the more appropriate methods of application “Apply as if applying it on top” and “Apply gently without rubbing” [10] were relatively rare. These findings highlight the challenges of patient guidance in the medical field. A previous survey study of pharmacists [11] found that approximately 40% of those prescribing steroids to patients with AD were instructed to “Apply thinly”, and in the future, it is important to communicate appropriate topical application medical practice guidance to patients from medical professionals, including doctors.
The results of the present study showed a trend towards high adherence rates with instructions for the amount, area and method of application of topical anti-inflammatory drugs in patients with AD, with adherence rate of more than 70% in all but a few patients. Adherence with treatment is a very important factor in the longevity of topical treatment for AD [6], suggesting that patients are highly aware of their treatment. In a 2019 survey more than 80% of pharmacy department pharmacists, acknowledged the importance of the topical steroid amount applied. As these results demonstrate, although such practices are generally recognized as necessary in Japan, education on treatment among dermatologists and other healthcare professionals in clinical settings remains insufficient. With regard to patient education, it will be essential to continue providing practical instruction on methods of topical application, and to make use of simple, user-friendly tools that can effectively explain application techniques.
In the instructions for each application, “No specific instructions” (Figs. 2, 4, 6) for the amount, area and method of application, each of these figures was consistently slightly higher than 20.0%, indicating a lack of communication between medical professionals (doctors, pharmacists, nurses, etc.) and patients. However, one possible reason why many patients reported that they had “received no instructions” may be that, although healthcare professionals did provide guidance, it was not communicated to patients in a manner that was clearly understood. This finding suggests that providing accurate and appropriately frequent instructions on topical application is essential for long-term disease management and, through improved symptom control, can also contribute to enhanced quality of life (QOL). We consider these data to represent a valuable study that elucidates the current situation in this area. Based on this fact, and to raise awareness among specialists, it is important, although such initiatives have already begun in Japan, to further establish instruction groups within dermatology-related societies and to implement correct application guidance in each region. Accordingly, we believe that providing patients with appropriate guidance and building a good relationship between healthcare professionals and patients will help reduce the proportion of cases with ‘no specific instructions’.
The results of this study suggest that although a high percentage of patients complied with instructions, that includes information that is not necessarily appropriate, which suggests that information provided by healthcare professionals has a large influence on topical therapy for AD, and that appropriate patient guidance is important. It was also found that proactive therapy during the remission maintenance phase has not yet become widespread in the treatment of AD and is not commonly recommended. Possible reasons for the reported lack of instructions include that guidance provided by healthcare professionals is not communicated accurately to patients, that healthcare professionals are too busy to provide proper instructions on topical application, or that they themselves are uncertain of the correct application method. To address these issues, it may be useful to establish dedicated instruction groups for healthcare professionals, where correct application techniques can be taught through demonstrations or videos, and to raise awareness of the possibility that patients may not have fully understood the instructions given. In order to achieve the AD treatment goal of “No interference with daily life” [1] through long-term continuation of topical therapy, it is considered essential to raise awareness of the appropriate application of topical medications in healthcare settings and provide appropriate guidance on treatment for the remission maintenance period.
Limitations
This study has limitations. First, individuals included in this study were members of employment-based health insurance associations under contract with DeSC and their families, and those who voluntarily responded to a questionnaire. These individuals may be highly health conscious, taking positive health actions in their daily lives, and this may, therefore, introduce selection bias, which in turn limits the generalizability of our findings to the Japanese population.
Second, the self-reported questionnaire responses were subject to self-report bias and recall bias due to reporting treatments received within the past 6 months.
Third, The choice between reactive and proactive approaches should be based primarily on the clinical course, and not all patients are suitable candidates from proactive treatment.
Nonetheless, the strengths of the study include the new design of the study in combining receipt data from a health insurance association and the linked results of an online questionnaire; and the relatively large sample size.





Comments (0)