This study comprehensively evaluated LN involvement patterns using FDG-PET/CT in patients with known or suspected CS. We identified characteristic dissemination patterns that reflect the underlying lymphatic spread of sarcoidosis into the upper abdominal region. These findings enhance our understanding of the disease pathophysiology and may have important implications for diagnostic assessment. Sarcoidosis is a multisystem granulomatous disease with heterogeneous clinical presentations and variable organ involvement. FDG-PET/CT has proven highly effective in detecting extracardiac inflammatory activity, which is present in up to 97% of patients with CS [7], and in guiding the selection of biopsy sites [8, 9]. FDG-PET/CT has emerged as a critical modality for CS evaluation, providing high sensitivity for the detection of active inflammation in both cardiac and extracardiac sites [10].
In our study, hilar and mediastinal LNs were involved in 79% and 76% of cases, respectively, consistent with prior reports [11]. Simonen et al. reported increased FDG uptake in mediastinal LNs in 63% of CS patients, particularly in the right upper and lower paratracheal, subcarinal, subaortic, and para-aortic regions. In addition, 26% of their cohort showed FDG-avid lesions outside the mediastinum, reinforcing the role of mediastinal LNs as accessible biopsy targets [12]. Teirstein et al. identified 139 cases of extracardiac uptake in their evaluation of 188 FDG-PET scans in 137 sarcoidosis patients. Mediastinal LNs (n = 54), extrathoracic LNs (n = 30), and lung parenchyma (n = 24) were the most frequently involved regions, followed by the spleen, liver, muscle, lacrimal/parotid glands, subcutaneous tissue, and bone [11]. Their findings highlighted the mediastinum as the most common site of extracardiac disease, possibly explained by lymphatic drainage of the left heart to the right upper paratracheal LNs [13].
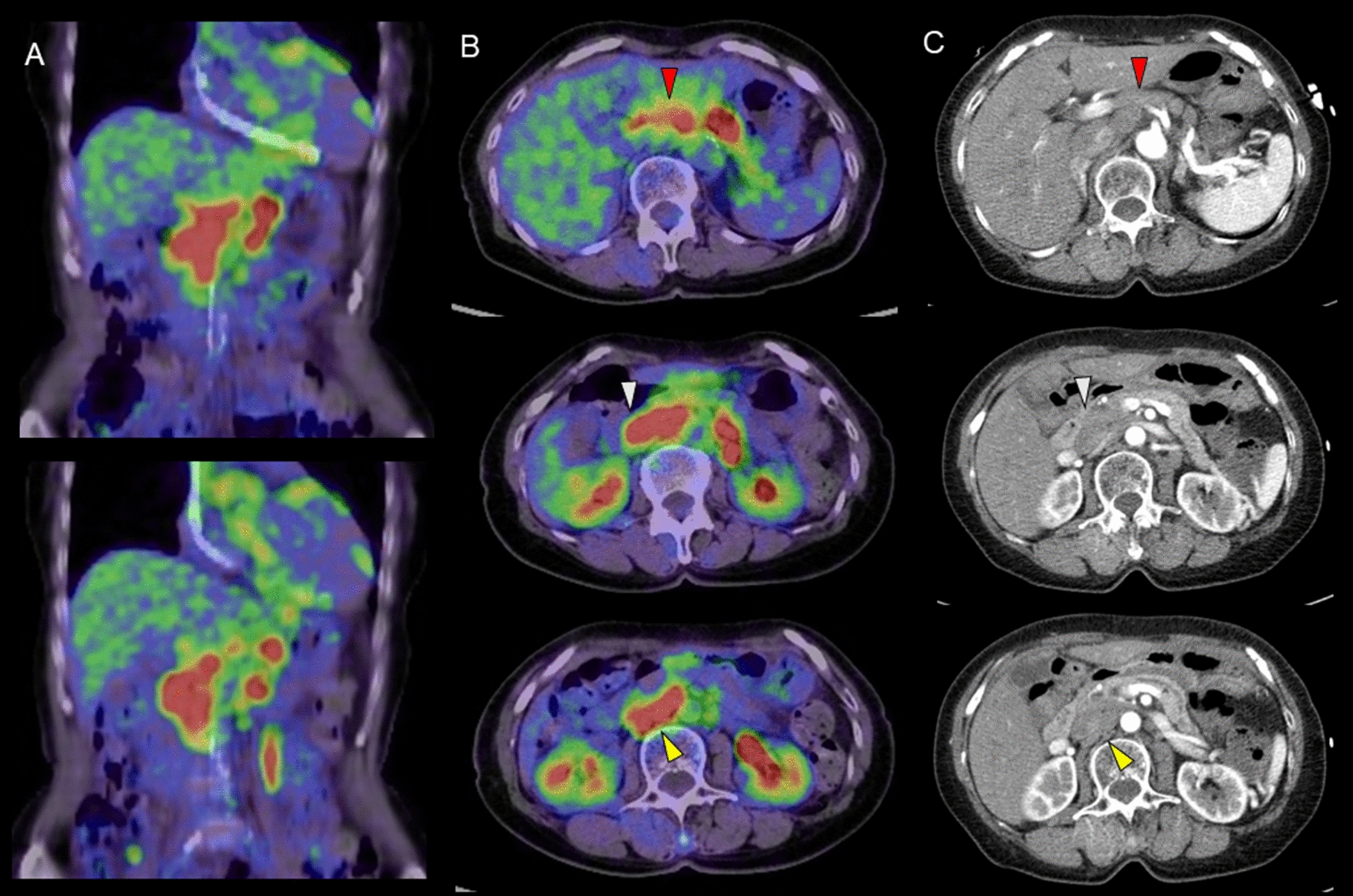
Beyond thoracic involvement, FDG uptake in upper abdominal LN was identified in over 50% of our cohort. FDG-positive LNs were detected most frequently in the PLN, PPDLN, APDLN and celiac LN regions. Our heatmap analysis further demonstrated frequent co-positivity among anatomically adjacent LNs within established lymphatic territories. For example, the highest co-occurrence was observed between hilar and mediastinal LNs (133 cases), followed by upper abdominal–hilar (88 cases) and upper abdominal–mediastinal (85 cases) associations. These findings support the hypothesis that sarcoidosis spreads through lymphatic channels. In contrast, peripheral LNs such as the axillary, subclavian, inguinal/pelvic, and bone marrow regions showed minimal co-occurrence with central LNs.
Although intra-abdominal sarcoidosis is relatively uncommon, it can occur even in the absence of thoracic or pulmonary disease. It is often asymptomatic but may lead to serious complications if left undiagnosed [14]. Abdominal lymphadenopathy is observed in approximately 30% of sarcoidosis patients, typically affecting the hepatic hilum, celiac axis, para-aortic area, mesentery, and iliac vessels. CT imaging shows hypodense LNs, generally 1–2 cm in diameter. LNs exceeding 2 cm are seen in up to 10% of cases and may raise concern for malignancy, particularly lymphoma [15,16,17].
However, due to their small size, benign appearance, and complex anatomical location, upper abdominal LNs have received limited attention, despite prior reports identifying them as a typical site of sarcoid involvement on CT imaging. Our findings provide additional evidence that FDG uptake in upper abdominal LNs is a specific and diagnostically useful feature of sarcoidosis.
Britt et al. have reported that sarcoid LNs were smaller and less confluent in sarcoidosis than in non-Hodgkin lymphoma (NHL). The average nodal size was significantly smaller in sarcoidosis (2.6 ± 1.7 cm) than in NHL (8.0 ± 5.5 cm), in which LNs were more frequently located in the retrocrural space [17]. In another study, assessment based on mediastinal LN FDG uptake showed no significant differences between sarcoidosis and sarcoid reaction, or between sarcoid reaction and malignant lymphoma [18]. Therefore, FDG uptake in upper abdominal LNs may serve as a key finding to support a more confident diagnosis of sarcoidosis. Involvement of PLNs, PPDLNs, APDLNs, and celiac LNs occurs because of their roles in the lymphatic drainage of the pancreas and liver. Celiac LNs, located at the root of the celiac artery, receive lymph drainage from the stomach and spleen. Duodenal lymphatics drain into pancreaticoduodenal and pyloric LNs (anterior group), or via the head of the pancreas to superior mesenteric LNs (posterior group), with eventual convergence toward celiac LNs [19, 20].
Several studies have proposed clinical phenotypes of sarcoidosis based on the distribution of lesions, with a primary focus on organ involvement. A large cohort study conducted in Spain that included 1230 patients found that those with pulmonary involvement had lower rates of skin and salivary gland disease but a higher frequency of liver involvement [21]. A retrospective multicenter study identified five clinical phenotypes using hierarchical cluster analysis. Their analysis revealed that cardiac and fibrotic pulmonary involvement clustered within the same phenotype, which also included neurological and abdominal manifestations [22].
Considering the superiority of FDG PET in the diagnosis of CS, it is expected that this modality will contribute to phenotypic disease characterization in sarcoidosis [23]. Papiris et al. proposed four distinct phenotypes of systemic sarcoidosis based on organ involvement: (1) thoracic nodal (hilar–mediastinal), (2) thoracic nodal and pulmonary, (3) extended thoracic and extrathoracic nodal (including inguinal, abdominal, and supraclavicular stations), and (4) a systemic phenotype involving all of the above plus organs such as muscle, bone, spleen, and skin [24]. Abdominal LN involvement is characteristic of phenotypes 3 and 4. No significant differences in myocardial involvement were found among the identified clusters, which suggests that CS may occur independently of other organ-based phenotypes.
Despite the comprehensive evaluation performed, this study has several limitations. First, it is retrospective in nature, which may have introduced selection bias and limited control over confounding variables. Second, while FDG-PET/CT is highly sensitive, FDG uptake is not specific to sarcoidosis and can be influenced by infections, malignancies, or other inflammatory processes. Histopathological confirmation was not available for all FDG-avid LNs, which limits correlation between imaging findings and definitive diagnosis. We used decreased or resolved FDG uptake on follow-up PET/CT as supportive evidence to increase confidence that an FDG-avid lesion represented true sarcoidosis. This was not used to diagnose sarcoidosis itself, but rather to strengthen the interpretation of each lesion as a true-positive finding. The heatmap provide valuable visual and quantitative insights but do not account for dynamic disease processes or temporal changes in nodal involvement. In addition, variability in image interpretation and differences in PET scanner technology or protocols could have affected SUV measurements and lesion detectability, even though we confirmed that the recovery coefficients were nearly equivalent across the PET/CT scanners based on a NEMA phantom study. Finally, the cohort was derived from patients undergoing evaluation for suspected CS, which may not fully represent the broader sarcoidosis population. In our country, FDG-PET is primarily approved for the diagnosis of CS, and it may account for the low incidence of lung uptake observed in our study.





Comments (0)