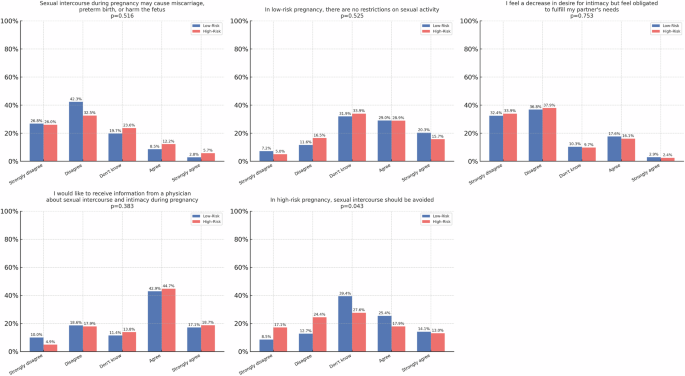
We report that sexual activity, desire, satisfaction, and perceived partner interest during pregnancy were broadly similar among women with high-risk and low-risk pregnancies. Most participants reported decreased sexual activity during pregnancy, regardless of risk status. Physician-initiated counseling on sexual health was infrequent, despite a clear interest from patients to receive such guidance. Beliefs about the safety of sexual activity varied. However, a notable proportion of high-risk patients disagreed with the notion that intercourse should be avoided due to their condition. Similar responses were observed among participants with GDM and those with low-risk pregnancies.
This study provides important insights into the sexual health experiences and counselling needs of pregnant women across both high-risk and low-risk categories within a culturally diverse population. Despite differences in clinical risk profiles, the overall patterns of sexual health reported by the participants were broadly similar between the two groups.
The high-risk condition that has been examined in the literature is GDM. We report similar outcomes related to sexual activity, perceptions, and counseling, between patients with GDM and with low-risk pregnancies [10]. However, the evidence regarding the impact of GDM on sexual function during pregnancy remains inconclusive. Some studies suggest that women with GDM are more likely to experience sexual dysfunction including decreased libido, reduced sexual satisfaction, and increased dyspareunia [5, 7]. These outcomes are often attributed to hormonal changes, metabolic disturbances, and the psychological stress associated with high-risk pregnancies. [8, 11] Such findings support the hypothesis that GDM may exacerbate both the physical and emotional burdens of pregnancy, thereby adversely affecting sexual health. Conversely, and in alignment with the findings of the current study, other research has reported no significant differences in sexual function between women with GDM and those with low-risk pregnancies. These findings suggest that GDM, in isolation, may not be a decisive factor influencing sexual well-being. [10] We compared only 31 participants with GDM and 72 with low-risk pregnancies. Future studies with larger cohorts are needed to further explore these findings.
Importantly, unlike other high-risk conditions such as a short cervix, premature contractions, or threatened preterm labor where sexual activity may reasonably raise concerns about preterm birth GDM does not constitute an evidence-based indication for restricting intercourse during pregnancy. Although it can be assumed that GDM may contribute to sexual dysfunction through metabolic, hormonal, or psychological mechanisms similar to those observed in diabetes [12], it does not share the obstetric contraindications characteristic of conditions directly associated with preterm birth. This distinction highlights the importance of nuanced, condition-specific counseling rather than generalized recommendations for all women classified as high-risk. In accordance with prior research, [13, 14] a substantial proportion of our participants, regardless of their risk status, reported a decline in sexual activity and desire during pregnancy. This reduction was frequently linked to concerns about fetal safety. Several studies have documented that many couples harbor fears that engaging in sexual intercourse during pregnancy may result in obstetric complications, including vaginal bleeding, miscarriage, preterm labor, or potential harm to the fetus. [15, 16] Although misconceptions about the potential risks of sexual activity during pregnancy were relatively common, more than 40% of participants in both groups disagreed with these beliefs. This suggests a growing awareness and acceptance of evidence-based information regarding the safety of sexual activity during pregnancy. [13] These findings underscore the importance of targeted antenatal education to correct misinformation and alleviate unwarranted fears. Despite these concerns, perceptions of partner desire and overall sexual satisfaction were similar across both groups. Interestingly, high-risk pregnancy status did not correlate with increased sexual dissatisfaction or more negative self-perceptions of sexuality. This may reflect the influence of individual coping mechanisms, partner support, and sociocultural factors that help mitigate psychological stress. For women in the high-risk group, the gestational age at the time of questionnaire completion was significantly lower compared with the low-risk group. Sexual function is known to change throughout pregnancy, as demonstrated by Fernández-Carrasco et al. [6] who described trimester-related variations. These changes, however, were most pronounced when comparing different trimesters, rather than within the same trimester. Since both groups in our study were, on average, in the third trimester when sexual desire and activity are reported to rise, this difference in gestational age is unlikely to have had a major impact on the overall outcomes. None of the participants reported cultural or family-imposed restrictions on sexual activity. However, a significant gap emerged in clinical practice, and physician-initiated discussions on sexual health were notably infrequent. Only 21.4% of the women reported receiving any counseling on sexual matters from healthcare providers, despite more than half expressing a desire for such guidance. This highlights a critical missed opportunity to normalize conversations around sexual health, dispel persistent myths, and provide essential emotional support during pregnancy. The limited provision of sexual health counseling reported in our study likely reflects a broader systemic gap in medical education. [17] Research assessing curricula across North American medical schools has shown that although most programs include some theoretical instruction on human sexuality, the majority provide fewer than 10 h of education. The latter is often delivered in lecture format without practical training or clinical exposure. Less than half of medical schools offer supervised clinical programs addressing sexual dysfunction, or patient counseling on sexual concerns. [17] The lack of training may contribute to physician discomfort and to lack of confidence in initiating conversations about sexuality during pregnancy. This is consistent with the low rates of counseling reported in our cohort.
Strengths of this study include its focus on an often-overlooked aspect of maternal health, namely, sexuality during pregnancy. The comparison between high-risk and low-risk pregnancies contributes to the current literature. Furthermore, the inclusion of both subjective experiences (e.g., satisfaction and desire) and behavioral outcomes (e.g., frequency of intercourse and help-seeking behaviors) offers a comprehensive overview of sexual health in pregnancy. The relatively large sample size and high response rate further support the robustness of the findings. However, several limitations should be acknowledged. First, the cross-sectional design precludes assessment of causality or changes in sexual health across pregnancy. Second, the use of a self-administered questionnaire introduces the potential for recall bias and social desirability bias. Third, while the questionnaire was reviewed by experts and pilot-tested, it was not formally validated, which may affect the generalizability of the findings. Finally, the high-risk category encompassed a broad range of. These conditions may have differential effects on sexual health, particularly for women with a history of preterm birth or cervical shortening, who comprised nearly one third of this group. This heterogeneity should be explicitly acknowledged, as it may limit the comparability of outcomes within the high-risk cohort.
Our findings emphasize the need to integrate comprehensive, culturally sensitive sexual health counselling into routine antenatal care. Empowering healthcare providers to initiate open, empathetic discussions can help reduce stigma, address patients’ unmet needs, and improve the overall quality of care for pregnant women, particularly those managing the added complexities of high-risk pregnancies.


Comments (0)