Obesity is a major public health problem, with a progressively increasing prevalence, reaching over 50% in several countries [11]. Adipose tissue is not simply a storage depot; it is a more complex organ with endocrine functions and the ability to synthesize a series of hormones and active molecules, which are associated with elevated levels of pro-inflammatory cytokines [12]. These cytokines, such as tumor necrosis factor-α, interleukin-6, interleukin-1β, and adipokines such as leptin and resistin, are pro-inflammatory molecules exacerbating various metabolic changes, cardiovascular diseases and chronic inflammatory state [13, 14]. Numerous studies have correlated BMI with mortality for cardiovascular disease. Although BMI measurement has significant clinical limitations unlike evaluation of the body fat percentage, more accurate measure but less usable in large-scale studies.
In this study, carried out on a population without previous cardiovascular events, we confirmed that obesity, assessed through BMI, is strictly correlated to significant increased blood pressure values, both SBP and DBP, and to several metabolic alterations, such as dyslipidaemia and hyperglycaemia.
Several studies on different populations have demonstrated a linear relationship between BMI and SBP. The Framingham Heart Study highlighted that 78% of primary essential hypertension in men and 65% in women may be due to excessive weight gain [15]. The underlying mechanisms are several: increased intrarenal pressure and impaired natriuresis, activation of the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system, leading to the development of advanced forms of coronary artery disease, arrhythmia, heart failure, and stroke [16, 17]. Beyond arterial hypertension, obesity has been strongly associated with diabetes mellitus, dyslipidaemia, atherosclerosis, obstructive sleep apnea syndrome (OSAS) and MS [11].
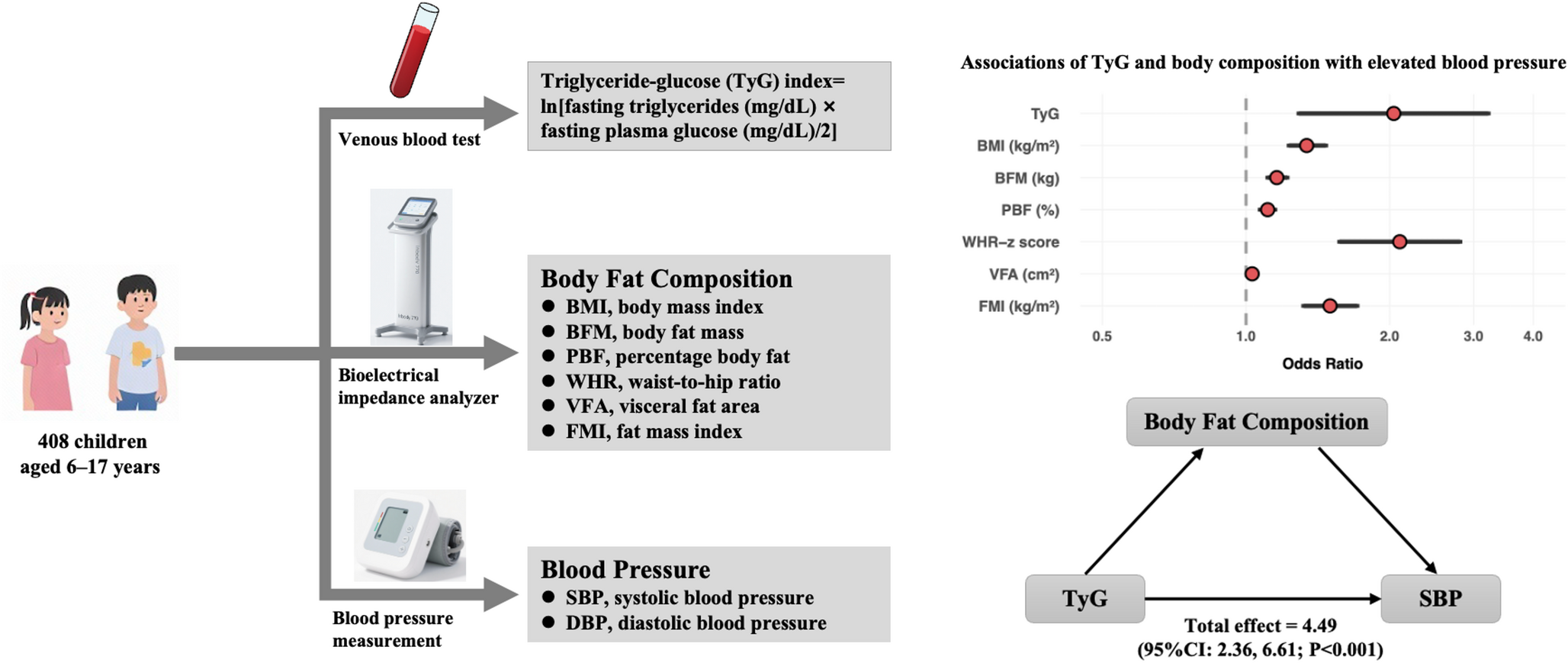
A common element in all the alterations inducing complications of obesity, the IR affects the cardiovascular system by promoting chronic inflammation, increased production of nitric oxide and sympathetic nervous system overactivity [18,19,20]. Therefore, early diagnosis of IR is crucial to identify high-risk individuals. Although the hyperinsulinemic-euglycemic clamp is the established "gold standard" for detecting IR, its complexity prevents the widespread use [21]. As regards, the TyG index is emerging as a simple, cost-effective, and reliable alternative [22]. Calculated on a logarithmic scale from fasting triglyceride and glucose levels, the TyG index effectively assesses the pathophysiology of IR, highlighting increased triglycerides, due to overproduction of VLDL and chylomicrons, and hyperglycaemia, promoted by higher gluconeogenesis [23]. Numerous studies have confirmed the significant correlation of the TyG index with cardiovascular risk and overall mortality [24,25,26], and the predictivity of the TyG index on the development of MS [27].
In the literature there are no univocal cut-offs for TyG values, but different studies have identified a cut-off for TyG >4.5, strong predictor for cardiovascular events; in our study we confirmed that obesity is associated with higher TyG index and with higher prevalence of patients with TyG index higher than 4.5 and greater subclinical organ damage, in particular, myocardial remodeling and hypertrophy. In this regard, IR, assessed by elevated TyG index, can promote organ damage both directly through arterial hypertension and metabolic alterations related to IR.
Several observational studies have been conducted to explore the predictive role of TyG index on the incidence of arterial hypertension. A recent large-scale meta-analysis showed that higher TyG values were associated with 2-fold higher risk of hypertension and 3-fold higher for isolated systolic hypertension [28,29,30]. Page et al [31], in a large series of hypertensive on the National Health and Nutrition Examination Survey, during long-term follow-up (8 years) observed that higher TyG index was correlated to higher mortality for all causes and for cardiovascular diseases. Moreover, a large study conducted in China found significant relationship between TyG index, arterial hypertension and arterial stiffness, showing the positive association between the TyG index and brachial-ankle pulse wave velocity (baPWV), auxiliary tool for the evaluation of arterial stiffness in daily clinical practice [32].
The development of arterial hypertension in IR is supported by numerous alterations involving the endothelium dysfunction, activation of the sympathetic-adrenal system and RAAS, and by suppression of the functioning of the sodium-potassium and calcium-magnesium ATPase complex [33].
In this study we found higher prevalence of MS with increasing BMI and the TyG index proved to be a better predictor in identifying patients with MS than alone blood glucose and triglycerides. MS is characterized by a combination of different factors associated with the risk of residual cardiovascular disease; the underlying pathophysiological elements are central obesity, hypertension, insulin resistance (IR), and atherogenic dyslipidemia [34]. Therefore, it is important to develop routine markers to assess patients' cardiometabolic status without incurring significant delays or increased financial costs. In the Olivetti Heart Study-OHS, the Authors have highlighted the ability of TyG index to predict the risk of developing MS during 8-year follow-up period [35]. Similar results were shown in a meta-analysis by Nabipoorashrafi et al. [36], evidencing the predictive value of TyG index superior to other indices, including the HOMA index. In this regard, in large population-based studies of diabetic patients conducted in both Europe and Asia, the TyG index has proven to be a reliable tool for predicting the development of T2DM over a 5-9-year follow-up, particularly with TyG index >8.3 [37]. In the cross-sectional PROCARDIO-UFV study, elevated TyG index (>9) were shown to be more predictive of developing MS, type 2 diabetes, and non-alcoholic fatty liver disease (NAFLD), as well as a higher rate of developing cardiovascular events over 10 years [38].
Moreover, in this study we highlighted that cardiac remodeling is strongly predicted by the TyG index with respect to plasma glucose or triglycerides alone.
Regarding the predictive capacity of TyG index to detecting the organ damage, a recent meta-analysis involving 28,643 participants found that the TyG index was positively associated with myocardial fibrosis, as well as the risk of all-cause mortality and hospitalization for heart failure [39].
Beyond the high blood pressure values, cardiac remodeling is the consequence of various cardiovascular and metabolic alterations, such as hyperinsulinemia, oxidative stress, and low-grade inflammation, particularly in patients with IR and/or T2DM [40]. Chronic hyperglycaemia causes various pathophysiological alterations, such as increased cardiomyocyte size, as a consequence of increased expression of genes such as atrial and B-type natriuretic peptide (ANP-BNP), heavy-chain beta-myosin, and transforming growth factor (TGF) beta [41]; systemic and tissue RAAS, resulting in cardiac fibroblast proliferation and cardiomyocyte fibrosis [42]; increased acylation of glucosamine; increased oxidative stress with mitochondrial damage and endothelial dysfunction [43]. More advanced stages involve increased NADPH oxidase activity in cardiomyocytes, closely correlated with RAAS activation [44], macrophage infiltration, exacerbation of systemic inflammation and development of coronary artery disease (CAD) and heart failure [45]. IR is one of the main metabolic alterations observed in heart failure (HF) and closely correlated with poor prognosis. A recent meta-analysis conducted on over 750,000 subjects has evaluated the TyG index as a surrogate marker of IR in HF, highlighting that higher TyG index was associated with a greater risk of HF development (OR 1.21), particularly in patients with type 2 diabetes or coronary artery disease (OR 2), with a higher incidence of adverse events, such as rehospitalization and mortality [46].
Firstly in the literature, in our study we observed that the TyG index had greater predictive ability in highlighting cardiac remodeling and presence of MS, in particular in normal weight patients.
As regards, some studies have evaluated the clinical usefulness of new parameters including laboratory and anthropometric data. Recently, Ke Song et al. [47] evaluated the predictive value of a new TyG-BMI index, composed of three simple indicators as triglycerides, blood glucose, and BMI, highlighting greater sensitivity than alone triglyceride or blood glucose measurements. In asymptomatic patients this index appears suitable for identifying high-risk populations, especially regarding the risk of cardiovascular events or development of type 2 diabetes and non-alcoholic fatty liver disease (NAFLD). Since there are no recognized risk thresholds, this index could have clinical utility in assessing improvement in IR status following dietary or pharmacological interventions for weight loss.
In conclusion, our study confirms that obesity is correlated with a worse hemodynamic and metabolic profile. IR is one of the main pathophysiological elements underlying all complications, and the TyG index could represent an efficient and easy-to-use surrogate biomarker for identifying both individuals developing MS and early cardiac remodeling. These results are most evident in normal-weight hypertensive subjects, which represents the population in which the failure to recognize hemodynamic and metabolic alterations can cause the greatest harm.
4.1 Study Limitations and Clinical Perspectives
Although our data are encouraging, some limitations deserve discussion. The cross-sectional design of the study precludes temporal or causal conclusions; increasing the sample size could find additional data, such as identifying a cutoff point to predict subclinical organ damage at different sites (such as renal injury, fundus oculi, or vascular level) or gender-related differences. There are no clear cutoff values for TyG levels in the literature; we used a cutoff value of TyG >4.5, due to its strong predictive ability to predict cardiovascular events; other values have been used to predict MS, development of arterial hypertension in children and adolescent, or the development of metabolic dysfunction-associated fatty liver disease (MAFLD) in older ager [48]. Moreover, during lifestyle modification or pharmacological treatment, the evaluation of the TyG index can be efficient for assessing changes in IR in individual patients. Nonetheless, the internal consistency of our results, combined with the robust methodology (uniform patient assessment, standardized and blinded echocardiography, exclusion of secondary hypertension), represent important methodological strengths that increase the reliability and clinical relevance of our findings.



Comments (0)