Hypertension International Guidelines: Three of a Kind?
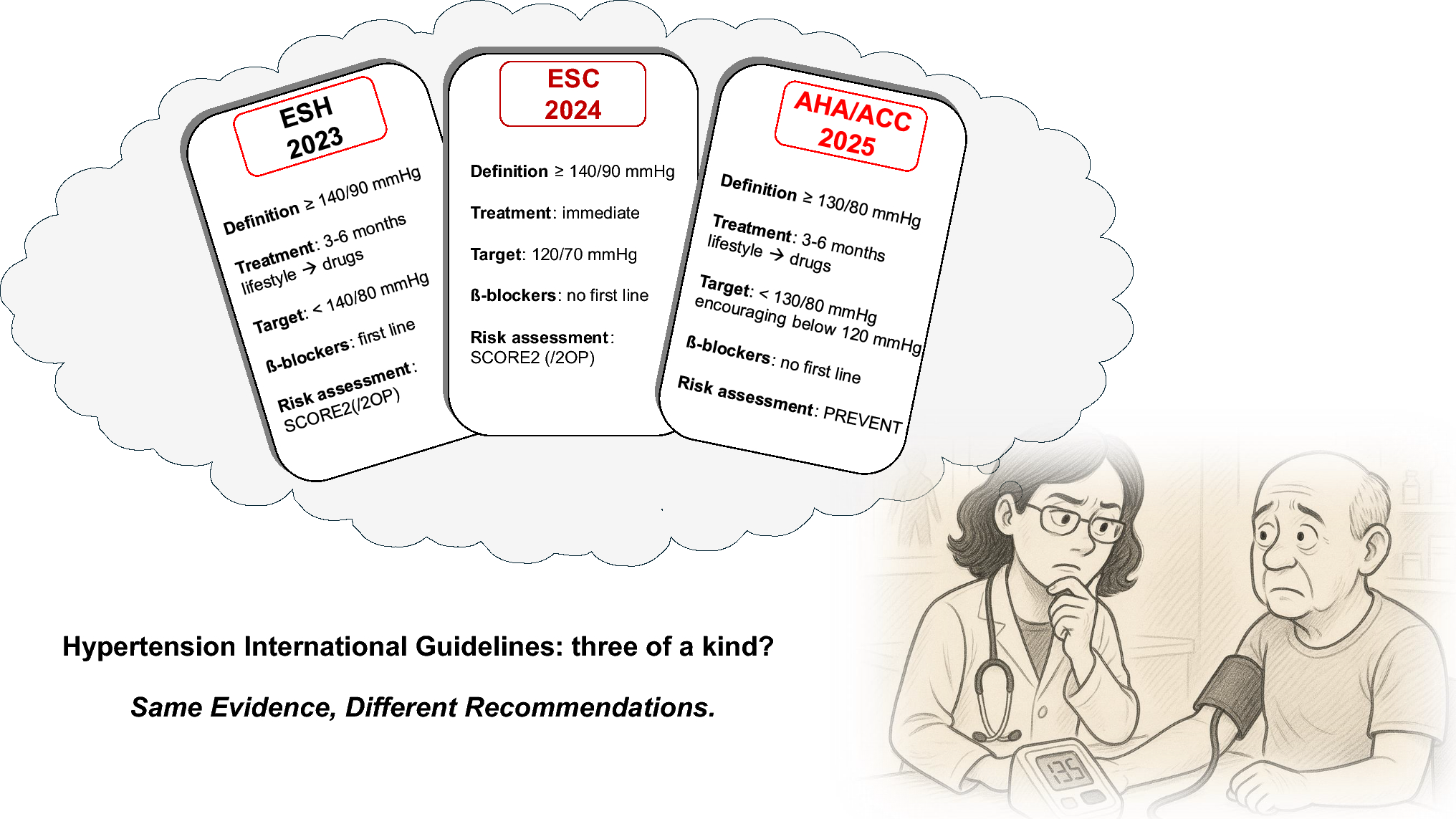
From the title onwards, it is interesting to note the different choices made by the task-forces in the three guidelines. The ESH and AHA/ACC remain consistent with the style of previous guidelines. While the ESH is focused on the disease, the AHA/ACC also emphasizes the importance of “prevention, detection and evaluation” as well as “management”. The ESC, on the other hand, introduce the new category of “elevated blood pressure” in the title. Turning to the definitions, the AHA/ACC adopted a systolic blood pressure (SBP) threshold of 130 mmHg and a diastolic blood pressure (DBP) threshold of 80 mmHg, which is consistent with that of the 2017 guidelines [6]. This is different from both the ESH and ESC and is based on the need for a more urgent and aggressive prevention and intervention strategy, as advocated by US physicians. This substantial change, indeed, halted the decline in BP control observed between 2013 and 2016, although the level of BP control has remained stable ever since [7]. In terms of classification, the AHA/ACC remains consistent with the 2017 guidelines by using the “elevated blood pressure” category, which was also adopted by the ESC in 2024, albeit with different cut-offs, as well as stages 1 and 2. Hypertension grading at three levels is present only in the ESH guidelines.
Some nuances are present regarding when to start pharmacological treatment. All three guidelines emphasize the need for lifestyle changes, regardless of BP control. As a general rule, all three guidelines recommend initiating treatment at 140/90 mmHg. However, the ESH takes a more conservative approach, recommending 3–6 months of lifestyle changes before starting treatment, unless BP is above 160/100 mmHg, the cardiovascular risk is high, or an established cardiovascular disease is present. In the last case, ESH recommends immediate treatment at BP levels of ≥130/80 mmHg. The ESC and AHA/ACC bypass lifestyle intervention alone for BP ≥140/90 mmHg. The AHA/ACC recommends immediate intervention when BP is ≥130/80 mmHg in cases of previous cardiovascular events and high CV risk, in line with the ESH.



Comments (0)