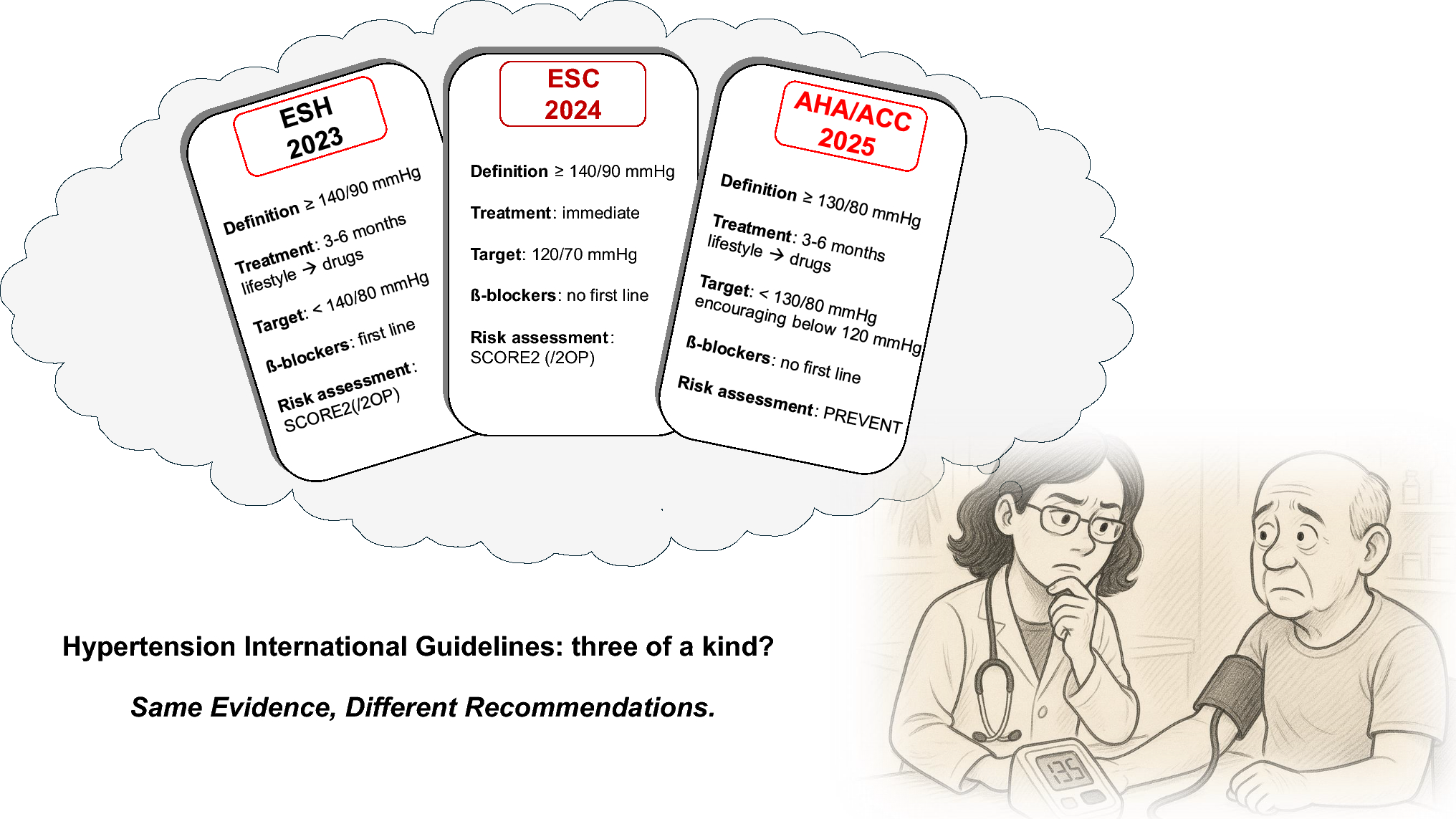
The care pathway for patients with hypertension has been developed based on the main international reference guidelines for hypertension by the European Society of Hypertension (ESH) in 2023 [11] and the European Society of Cardiology (ESC) in 2024 [1] and adapted to the healthcare model of the Italian National Health Service (NHS).
In the following section, a detailed description of the patient journey, structured according to the phases of the care process (diagnosis, treatment, and follow-up), is provided. A schematic representation of each phase is provided in the Supplementary Material.
2.1 Diagnostic Suspicion, Risk Stratification, and Diagnosis of Hypertension
Throughout their lifetime, an individual may have their Blood Pressure (BP) measured in different situations, such as routine visits to a general practitioner (GP), emergency room visits, pharmacy check-ups, or assessments for sports or work fitness.
Suppose systolic—and/or diastolic-BP is detected at or above 130–139/85–89 mmHg (SBP/DBP ≥ 130–139/85–89 mmHg) on any of these occasions. In that case, the patient should be referred to a GP for further diagnostic investigation (Table 1). Conversely, for SBP/DBP values are below 130–139/85–89 mmHg, it is advisable to evaluate whether GP referral is necessary to confirm or exclude the possibility of masked hypertension or white coat hypertension. If this assessment, as well as the search for organ damage and possible secondary causes of hypertension, gives a negative result, the condition of normotension can be confirmed.
Table 1 Assessment of patients with SBP/DBP ≥ 130–139/85–89 mmHg by the GPIn patients with confirmed high BP, repeated home blood pressure measurements (HBPM) are recommended, and ambulatory blood pressure monitoring (ABPM) may be tested if necessary. If the values are stable above the threshold (24-hour SBP/DBP ≥130/80 mmHg for ABPM and SBP/DBP ≥135/85 mmHg for HBPM), first and second-level diagnostic investigations are recommended for the initial work-up of the patient. Among the second-level examinations, it is possible to distinguish between those that can be performed as a diagnostic routine and those that must be carried out in case of specific need for further investigation. Details of the first and second level exams are illustrated in Table 2 [1, 11].
Table 2 List of recommended first- and second level testsThe tests aim to assess the presence of signs of HMOD, secondary hypertension, and evaluate cardiovascular disease (CVD) risk.
At the end of the diagnostic pathway, patients are diagnosed with:
Essential hypertension, with a specific degree of severity.
Suspected secondary hypertension (Table 3), requiring further investigation at a specialized hypertension center [11].
Table 3 Signs of possible secondary hypertension2.2 Evaluation of a Patient with Suspected White Coat or Masked Hypertension
In patients with high BP values (SBP/DBP ≥ 130–139/85–89 mmHg) detected in at least one BP measurement but not subsequently confirmed in the GP setting, it is suggested to verify the presence of white coat hypertension or masked hypertension [11].
Additional HBPM (and, if necessary, also ABPM) monitoring, first–level diagnostic tests (Table 2), and a cardiovascular (CV) risk assessment are conducted to estimate the probability of developing hypertension over time and assess the presence of HMOD.
The experts of the Scientific Committee highlighted the following aspects as topics of attention:
The 2023 ESH guidelines suggest considering potential treatment for patients at high and very high CV risk even without a confirmed diagnosis of arterial hypertension [11].
The 2024 ESC guidelines introduce a new category of elevated BP (120–139/70–89 mmHg) and recommend assessing CV risk to determine when to initiate therapy, particularly if values exceed 130/80 mmHg and patient has a comorbidities such as type 2 diabetes mellitus (T2DM), chronic kidney disease (CKD), or heart failure (HF) [1].
2.3 Treatment
Following the diagnosis of hypertension, GPs should assess whether to initiate therapy independently or refer the patient to a specialist and/or a hypertension center. The decision depends on the type of hypertension diagnosed and the clinical characteristics of the patient:
Essential hypertension—Grade 1: The GP directly manages the initiation of therapy.
Essential hypertension—Grade 2 or 3: The treatment should be initiated and supervised by a specialist (cardiological/ internist clinic or hypertension specialized center). Before setting up the therapy, the patient must undergo a specialist evaluation (by an internist, cardiologist, nephrologist, or other specialist for hypertension) and, if necessary, a multidisciplinary evaluation involving other specialists.
Suspected secondary hypertension: Before proceeding with the therapy setting, the patient should be referred to the hypertension specialized center for further evaluation to rule out or confirm a diagnosis of secondary hypertension. Following further evaluation, suspected secondary hypertension can be:
Confirmed with a treatable underlying cause: The patient is referred to an alternative care pathway to address the underlying condition.
Confirmed with a non-treatable underlying cause: Proceed with the therapy setting.
Not confirmed: A diagnosis of essential hypertension (grade 1, 2, or 3) is established, and therapy is initiated accordingly.
The therapy approach for hypertension combines several strategies:
Non-pharmacological treatment (lifestyle modifications, including diet, physical activity, stress reduction, etc.).
Drug treatment
Management of other CV risk factors and concomitant clinical conditions.
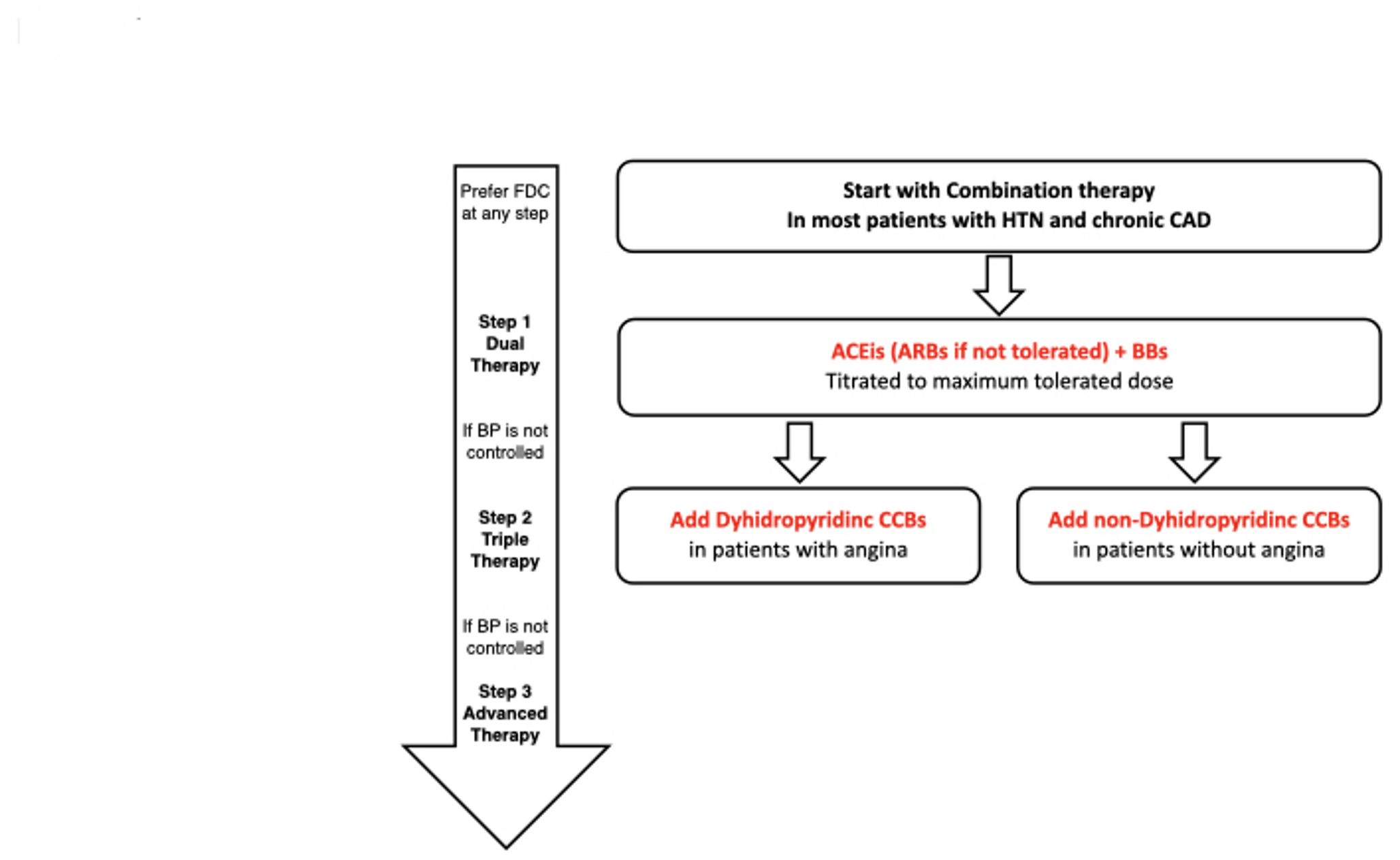
Pharmacological treatment follows a gradual approach in different steps to reach the BP target within 4–6 weeks:
1.
First step (initial step):
Double combination therapy: Angiotensin-Converting Enzyme Inhibitor (ACEi) or Angiotensin II Receptor Blocker (ARB) + Calcium Channel Blocker (CCB) or thiazide diuretic [1, 11].
Initial monotherapy preferred for frail and/or elderly (≥ 85 years) patients, or with low hypertension and BP < 150/95 mmHg, or high-normal BP with high CV risk [11].
2.
Second step (if BP is not on target after 4–6 weeks):
For all therapeutic steps, we suggest:
Prefer Single Pill Combinations (SPCs).
Titration until the maximum tolerated dose is reached.
The use of β-blocker (BB) as monotherapy or at any step of combination therapy in concomitant clinical conditions in which indicated, both for cardiovascular disease (e.g., ischemic heart disease, tachycardia, ectopic disease, etc.), and non-cardiovascular (e.g., hyperthyroidism, tremors, headache, etc.) [11].
If, even after 4–6 weeks from the start of the second therapeutic step, BP is still not within the recommended limits, the presence of resistant hypertension may be suspected. In this case, the patient should be referred to the specialized hypertension center for confirmation of the diagnosis of resistant hypertension.
The patient who achieves and maintains the recommended BP target for at least 3 months is subsequently referred to the follow-up phase.
Again, the scientific committee identified the following aspects as key points of interest:
Immediate initiation of therapy is suggested for patients with grade 3 hypertension, grade 2 hypertension with high CV risk or organ damage, and hypertension associated with chronic kidney disease (CKD) or Type 2 Diabetes Mellitus (T2DM) [1].
In the treatment of hypertension, therapeutic strategies may be adjusted based on age and the presence of comorbidities. In elderly patients (age > 80 years), therapy is recommended if systolic BP is ≥ 160 mmHg, provided they are in sufficiently good general health to benefit from the reduction of CV risk [1].
For patients with comorbidities such as Heart Failure (HF), CKD, T2DM, and obesity, it is suggested to consider adding sodium-glucose cotransporter-2 inhibitors (SGLT2i)/glucagone-like-peptide-1 receptor agonist (GLP1RA) /angiotensin-receptor-neprilysin inhibitor (ARNI)/mineralocorticoid receptor antagonist (MRA) to the basic treatment, by the specific prescribing indications of each drug [1].
The 2024 ESC guidelines recommend a target systolic BP between 120 and 129 mmHg, provided the treatment is well tolerated [1].
2.4 Confirmation of Diagnosis of Resistant Hypertension
Patients with suspected resistant hypertension are referred to specialized centers to rule out a form of pseudo-resistance and confirm the diagnosis of resistant hypertension.
In hypertension centers, an in-depth analysis is carried out to rule out a form of pseudo-resistance, through:
Assessment of therapeutic adherence to rule out poor compliance with treatment;
Search for other causes of hypertension, including those attributable to secondary forms of hypertension;
ABPM and HBPM monitoring.
If, following the patient’s evaluation, causes potentially responsible for the lack of BP control are identified, the first step is to intervene to correct them and re-evaluate the patient after 4–6 weeks. If, as a result of the suggested actions, BP returns to target values, the patient is reclassified with essential hypertension of grade 1, 2, or 3.
If, on the other hand, BP remains high and no identifiable cause for the lack of BP control is found (including a form of secondary hypertension), the diagnosis of resistant hypertension is confirmed, followed by a re-evaluation of drug treatment.
2.5 Treatment of Patients with Resistant Hypertension
In cases of resistant hypertension, therapy should be reviewed and managed by a specialized hypertension center.
Before proceeding with the review of the therapy in use, it is recommended to proceed with an evaluation of the eGFR:
If eGFR < 30 ml/min/1.73m2:
Replace thiazide diuretics with loop diuretics.
Chlorthalidone (first choice) may be added or other thiazide-like diuretics, β-blockers, α-blockers, or centrally acting agents [11].
If eGFR ≥ 30 ml/min/1.73m2:
Spironolactone (25–50 mg), or another MRA, is added to the basic treatment (first choice) [11].
In patients receiving spironolactone, it is critical to monitor tolerance to the drug, with particular attention to the risk of hyperkalemia. If spironolactone is not well tolerated, it can be replaced with:
The ESH 2023 guidelines suggest, in eligible patients, to consider the addition of SGLT2i (currently indicated for the treatment of patients with HF, CKD, and T2DM), as their use may add a moderate BP-lowering effect to background antihypertensive therapy for patients with resistant hypertension [11].
Following the review of the therapy and the achievement of the BP target for at least 3 months, the patient can be referred to the follow-up phase.
2.6 Follow-Up
Patients with stable BP within the target for at least 3 months should be monitored periodically in the follow-up phase. The frequency of follow-up and the specialist involved are different according to the diagnosis of hypertension:
Patients with grade 1, 2, or 3 essential hypertension and secondary hypertension are suggested to be followed by the GP, with a monitoring frequency ranging from every 3 months to once per year. Patients with resistant hypertension and those with high complexity (e.g., with high/very high CV risk or comorbidities) are suggested to be followed by the specialist or by the hypertension center, with a monitoring frequency ranging from a minimum of 3 to a maximum of 6 months.
The Scientific Committee emphasized the following aspects as focus areas:
The management of patient follow-up, even when primarily the responsibility of the specialist/Hypertension Centre, should be supported by the GP, who often has more frequent contact with the patient.
It is advised that the GP consult the specialist at any time during follow-up if needed, also via teleconsultation. Such consultation can be particularly useful during the therapy adjustment (e.g., in the summer season).
Consider drafting the Individual Care Plan for complex patients with comorbidities and sharing it with the specialist/hypertension center, to coordinate the treatment plan and monitoring.
The frequency of follow-up visits depends on the patient’s health. It is important to ensure that the patient is visited at least once within the maximum identified period.
Regardless of the care setting and frequency of check-ups, periodic patient assessment in the follow-up phase includes:
BP and heart rate measurement;
Lifestyle analysis;
Monitoring of possible adverse effects;
Assessment of adherence to therapy;
First-level work-up examination;
Reassessment of CV risk (including assessment according to the SCORE-2 model);
Verification of the presence of organ damage;
Monitoring of symptoms related to any comorbidities;
Counseling and training of the patient on lifestyles.
Monitoring of the BP target is also carried out during the follow-up phase: if the BP target is maintained, the patient is considered “controlled” and can be referred to the next periodic assessments; if the BP target is not reached, it is necessary to investigate the possible causes related and correct them.
Among the factors to be analyzed in the case of non-target BP are:
Poor adherence to therapy;
Side effects or intolerance to drugs;
Use of substances that increase BP;
Other conditions that can contribute to high BP.
After a maximum of 30 days, a new BP measurement should be performed: if the BP is within target values, the patient is considered “controlled” and can be referred to the next periodic assessments. If BP remains above the target, treatment should be re-evaluated and modified until target BP values are reached. In the case of an “uncontrolled” patient, it is suggested that the GP consult the specialist (also via teleconsultation) to discuss therapeutic strategy and the need for referral to the specialist.



Comments (0)