In this study of patients with resected lung cancer associated with IP, the low CALLY group was significantly associated with several clinicopathological characteristics and perioperative outcomes, including a %VC lower than 80%, prolonged postoperative hospital stay, and a higher incidence of postoperative pneumonia, compared to the high CALLY group. Furthermore, the CALLY index significantly stratified both the RFS and OS. These findings align with previous reports showing associations between the CALLY index and postoperative pneumonia in esophageal cancer [18] and postoperative prognosis in several types of cancer [11,12,13,14]. Importantly, our results indicate that the CALLY index may be useful for stratifying the postoperative risk in such patients. This index is calculated using readily available variables, including serum albumin, lymphocyte count, and CRP, and can be easily and inexpensively applied in clinical settings. Moreover, patients with a low CALLY index might benefit from preoperative interventions, such as anamorelin [24], a ghrelin receptor agonist approved for the treatment of cachexia, characterized by weight loss in certain types of cancer, to improve their nutritional status. Nerandomilast, a phosphodiesterase 4 B inhibitor with antifibrotic and immunomodulatory effects, is also expected to improve immune competence and the inflammatory response [25].
As defined by Iida et al., the CALLY index includes serum albumin, lymphocyte count, and CRP and can reflect the status of nutrition, the immune system, and inflammation [8]. Their design for establishing the CALLY index was based on combining the PNI and mGPS, and the superiority of the CALLY index over the PNI was demonstrated in predicting the prognosis after hepatectomy for hepatocellular carcinoma. In the present study, there was no significant difference in OS between the high and low PNI groups, and the ROC-AUC of the PNI for predicting OS was lower than that of the CALLY index. Furthermore, there was no significant difference in the OS between the mGPS 0 and mGPS 1 or 2 groups. Additionally, no significant difference was observed in the OS based on CRP or albumin levels. These findings highlight the significance of adding CRP to the serum albumin levels and lymphocyte counts in patients with resected lung cancer associated with IP.
In the original report by Iida et al., the albumin level, lymphocyte count, and CRP value were included in the CALLY index to reflect the patients’ nutritional status, immune status, and inflammation level, respectively [8]. Although PNI and mGPS are established indices associated with the postoperative prognosis in certain types of cancer, including lung cancer [26, 27], our results indicate that only the CALLY index, and not PNI or mGPS, was associated with the postoperative prognosis. Therefore, all three factors—nutritional status, immune status, and inflammation level—may be important in predicting RFS and OS in patients with resected lung cancer associated with IP.
The cutoff value for the CALLY index varies from study to study. The original report by Iida et al. defined a cutoff value of 5 [8]. For resected esophageal squamous cell carcinoma, gastric cancer, breast cancer, and non-small cell lung cancer, the respective cut-off values have been reported to be 1.7, 6.96, 2.285, and 6.2, respectively, all of which were derived from the analysis of the ROC curve for OS [11,12,13,14]. In a study demonstrating the predictive role of the CALLY index for postoperative pneumonia in esophageal cancer, the optimal cut-off value was defined as 3.47 [18]. In contrast, the present study defined the cutoff value as 0.97, suggesting that the optimal cutoff value for the CALLY index varies according to the type of disease and type of cancer. The reason for our lower cutoff value may also lie in the particularly poor nutritional status [28] and more elevated inflammatory status [29] in patients with lung cancer associated with IP. This is partially supported by a comparison of the median CALLY index of our cohort with that reported by Mizota et al. (3.98 [IQR 1.10, 10.93] vs. 7.85 [IQR 2.67, 19.04]) [14]. However, caution is advised with this comparison, as the report by Mizota et al. did not specify the number of lung cancer cases associated with IP in their cohort and statistical analyses were not feasible for this comparison.
IP-AE is a major concern in the postoperative management of resected lung cancer associated with IP because of its high mortality rate (43.9%) [6]. Risk scores for IP-AE have been established in Japan and are widely used [6]. The present study found a potential association between low CALLY and the incidence of IP-AE, although this association was not statistically significant. Matsubara et al. demonstrated a significant association between the controlling nutritional status derived from serum albumin, lymphocyte count, total cholesterol, and IP-AE [30]. These findings suggest that dysregulation of the nutritional status, the immune system, and inflammation might be associated with an increased risk of IP-AE and that the CALLY index could be useful in the preoperative stratification of patients at higher risk of developing IP-AE.
The present study is associated with several limitations. First, it had a retrospective design and was conducted at a single institution. Second, although there were 85 patients in the study, only 20 patients were included in the low CALLY group. Third, the number of OS and RFS events was 45, limiting the number of variables in the multivariate analysis. Fourth, although our study aimed to predict postoperative survival using preoperative variables, data from positron emission tomography/CT were not included because of the lack of data for 36 patients (42.4%). Fifth, our findings are yet to be validated in another cohort of patients. Sixth, the AUC value of 0.577 was relatively low for prediction, which may be due to the small number of events. However, the cutoff value of the CALLY index (0.97) effectively stratified the survival curve and was identified as an independent prognostic factor for RFS and OS in the multivariate analysis. Larger studies with more patients are needed to address these limitations.
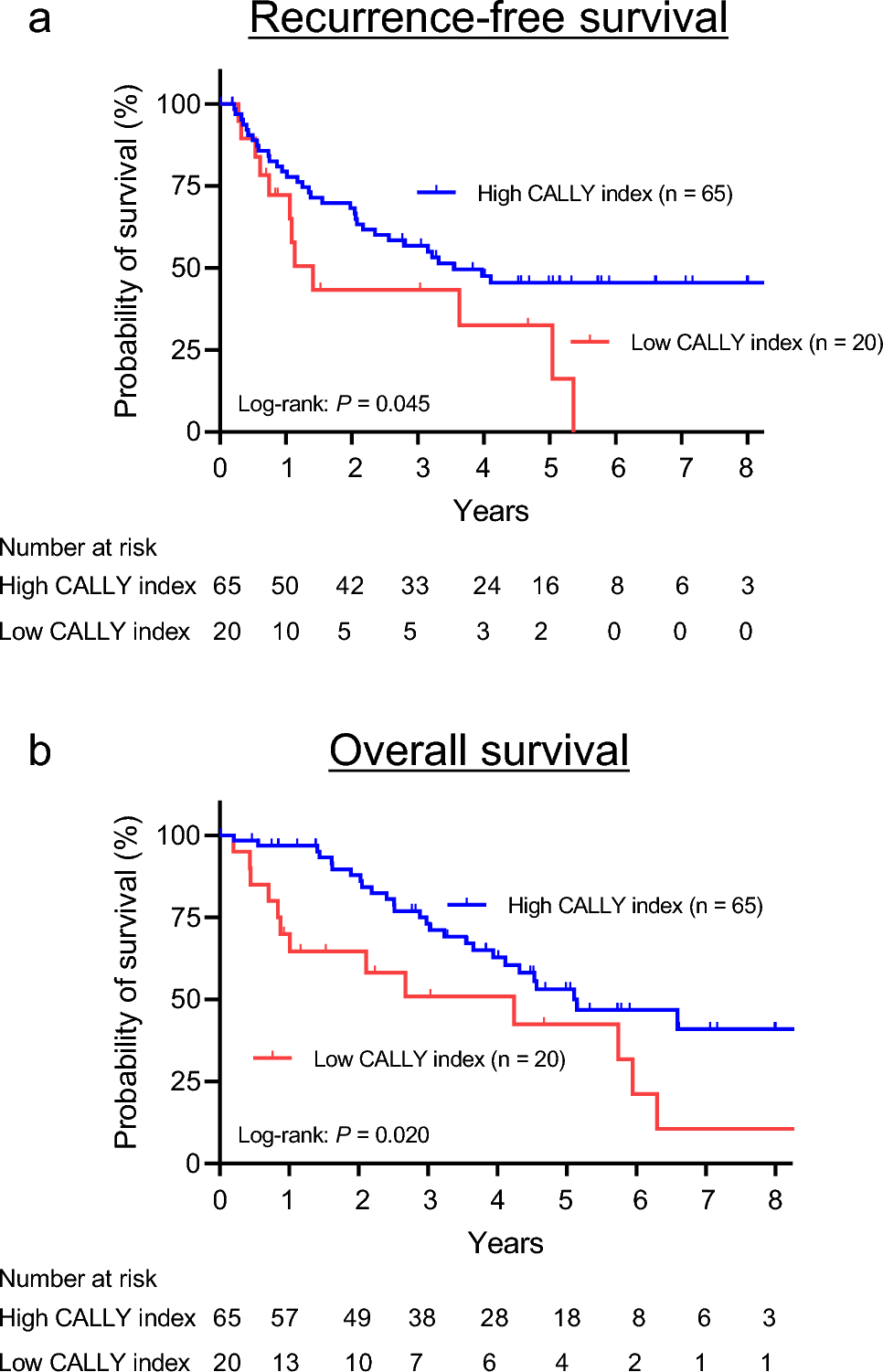
This study identified CALLY index as an independent prognostic marker for both RFS and OS in patients with resected lung cancer associated with IP. Furthermore, we found that the postoperative hospital stay was significantly longer, and the incidence of postoperative pneumonia was significantly higher in the low CALLY group than in the high CALLY group. Although studies that include more patients are required, these findings may assist in the postoperative management of patients with resected lung cancer associated with IP, particularly through close follow-up that may lead to the early detection of recurrence, timely treatment intervention, and ultimately improved post-recurrence survival.




Comments (0)