
Remember me



Headaches are estimated to affect more than 90% of the global population at some point during their lifetime and represent one of the most common complaints encountered in primary care, urgent care settings, emergency departments, and neurology clinics. Although the majority of headaches are due to primary disorders, a significant minority are secondary, with infectious etiologies among the most important causes [1]. Headache is a nearly universal symptom across a wide range of infectious diseases involving the central nervous system (CNS), including meningitis, encephalitis, and brain abscesses. In some cases it may be the first or only clinical manifestation of a potentially life-threatening condition [2]. Epidemiological data suggest that up to 60% of individuals experience headache in association with an infectious illness at some point in their lives [2, 3]. Headache is a common feature of systemic infections, often related to factors such as inflammation, dehydration, or metabolic imbalance. Despite its frequency, identifying clinical patterns suggestive of an infectious origin can be challenging. It may present as an isolated symptom, as a key sign of a severe infection, or be entirely absent. Underlying mechanisms include meningeal irritation, elevated intracranial pressure, and activation of the trigeminovascular system [4]. This article provides an overview of headaches attributed to systemic and/or intracranial infection, with particular emphasis on diagnostic red flags and classification. Given the broad scope of this topic, specific treatment protocols are beyond the scope of this review.
Classification and Diagnostic CriteriaThe International Classification of Headache Disorders, 3rd edition (ICHD-3), classifies headache attributed to infection within Chap. 9, distinguishing between “9.1 Headache attributed to intracranial infection” and “9.2 Headache attributed to systemic infection.” It further differentiates acute and chronic headache attributed to active infection, and, where applicable, persistent headache attributed to past infection (Fig. 1.). This classification framework highlights the importance of the temporal association between headache onset and the infectious process and considers the evolution or persistence of symptoms after resolution of the infection.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.ICHD-3 classification of headache attributed to infection
According to the ICHD-3, headache attributed to infection is diagnosed when a headache occurs in the presence of an active infection or its sequelae known to be capable of causing headache. Evidence of causation must be demonstrated by at least two of the following:
The headache develops in close temporal relation to the onset of the infection;
The headache significantly worsens in parallel with worsening of the infection and/or improves or resolves with improvement or resolution of the infection;
The headache has characteristics typical for the underlying infectious disorder.
Finally, the diagnosis requires that the headache is not better accounted for by another ICHD-3 diagnosis [5].
The major subtypes of headache attributed to infection in ICHD-3 include headache attributed to intracranial infection (e.g., bacterial meningitis or meningoencephalitis; viral meningitis or encephalitis; intracranial fungal or parasitic infection; and localized brain infection such as abscess or empyema) and headache attributed to systemic infection (systemic bacterial, viral, or other systemic infection), each further categorized into acute or chronic forms and, where applicable, persistent forms depending on the temporal profile [5].
Of note, distinguishing between a primary headache exacerbated by infection and a true secondary infectious headache remains challenging. In such cases, dual coding (e.g., migraine and headache attributed to infection) may be appropriate [1].
These diagnostic categories are not only clinically relevant but guide therapeutic decision-making and imaging strategies. A lumbar puncture is often necessary to confirm intracranial infections, whereas systemic infections may be diagnosed through serologic, microbiologic, or imaging findings [6, 7].
Overview of the International Classification of Headache Disorders, 3rd edition (ICHD-3), Chap. 9, illustrating the hierarchical classification of headache attributed to infection. The classification distinguishes headache attributed to intracranial infection (9.1) from headache attributed to systemic infection (9.2). Within each category, headache is further classified according to its temporal relationship with the infectious process as acute or chronic headache attributed to active infection and, where applicable, persistent headache attributed to past infection. Emerging or clinically recognized entities, such as COVID-19–related headache, are not depicted as distinct diagnostic categories but are mapped onto existing ICHD-3 core diagnoses based on the underlying infectious mechanism.
Pathophysiology of Headache Attributed to InfectionHeadache in the context of infection arises from complex interactions between host immune responses, microbial toxins, vascular and meningeal involvement, and the activation of pain-generating pathways. Although clinical manifestations are often nonspecific, the underlying pathophysiological mechanisms vary substantially depending on the infectious agent and its anatomical localization.
The principal anatomical pain generators include the meninges (particularly the dura mater), large intracranial vessels, cranial nerves (notably trigeminal afferents), and pain-sensitive perivascular structures. These structures can be activated by mechanical traction (e.g., from raised intracranial pressure), chemical irritants, or inflammatory mediators [2].
Cytokine-Mediated Meningeal IrritationBacterial and viral pathogens induce a cascade of pro-inflammatory cytokines tumor necrosis factor-α, interleukin (IL)−6, and IL-1β within the cerebrospinal fluid (CSF) and meningeal vasculature. These cytokines increase blood–brain barrier permeability and stimulate nociceptive pathways, resulting in diffuse or pulsatile pain. Matrix metalloproteinases (e.g., MMP-9) further amplify leukocyte recruitment and vascular dysregulation, thereby contributing to headache severity [8]. This immune response causes blood-brain barrier disruption, vascular dysregulation, vasculitis and even occlusion of blood vessels which can all individually cause vasogenic brain oedema, loss of cerebrovascular autoregulation, and eventually increased intracranial pressure [2].
Raised Intracranial Pressure (ICP)Increased ICP is a common pathogenic mechanism seen in bacterial meningitis, tuberculous meningitis, cryptococcal meningitis, and encephalitis. Edema formation, inflammatory exudate accumulation, and impaired CSF resorption at the arachnoid granulations contribute to pressure elevation. The resultant meningeal traction activates stretch-sensitive trigeminal afferents, leading to headache. In cryptococcal meningitis, fungal polysaccharides may physically obstruct CSF pathways, while tuberculous exudates can cause fibrin-mediated obstruction and chronic hydrocephalus [2, 6].
Direct Pathogen Effects and Toxin ReleaseSome organisms produce toxins (e.g., pneumolysin, streptolysin O, alpha-hemolysin) that directly activate nociceptors or potentiate inflammation [6]. In bacterial meningitis, lipopolysaccharide and peptidoglycan activate Toll-like receptors on meningeal macrophages and microglia, resulting in the release of prostaglandins and nitric oxide, which are key pain mediators [1, 2, 6].
Trigeminovascular System ActivationKey mediators (CGRP, substance P, neurokinin A) are released from trigeminal neurons in response to inflammation and play a central role in both primary and secondary headaches. The overlap in pathophysiology may explain why infection-related headaches can mimic migraine in some patients [2, 9].
Additional ContributorsSystemic factors, including fever, dehydration, electrolyte imbalance, and metabolic derangements may exacerbate headache during systemic infections even in the absence of direct central nervous system (CNS) involvement. These influences further blur the clinical distinction between primary and secondary headache presentations [1, 2, 9].
Clinical Syndromes of Infection-Associated HeadacheHeadaches secondary to infections of the CNS can present with varied intensity, localization, and accompanying features depending on the causative pathogen and site of involvement. They may occur in isolation or alongside systemic and neurological symptoms, such as fever, meningismus, or altered consciousness [2].
These shared pathways provide a mechanistic scaffold for interpreting the syndrome-specific phenotypes described below.
Bacterial MeningitisHeadache is often the earliest and most prominent symptom in bacterial meningitis. It is typically severe, diffuse or occipitonuchal, and associated with photophobia, phonophobia, nausea, and neck stiffness [1]. Patients often describe a worsening of headache during sudden movements, particularly with rapid side-to-side head turns (2–3 times per second), known as jolt accentuation. To reduce discomfort, they may instinctively assume a flexed posture, due to reflex muscle spasms in the neck and spine that serve to shield the head and neck [10]. The typical symptom triad of bacterial meningitis includes fever, neck stiffness, and altered mental status; however, this combination is missing in up to half of all meningitis cases [11]. In infants and young children, headache is often not reported; rather, the clinical picture may include fever, fontanelle bulging, somnolence, altered consciousness, and seizures [12].
In bacterial meningitis, headache primarily reflects direct inflammatory involvement of the meninges, leading to sensitization of meningeal nociceptive pathways. This infectious meningeal inflammation underlies the characteristic association with neck stiffness, photophobia, and phonophobia, and may partly account for migraine-like headache features observed in some patients [1].
Disturbance of cerebrospinal fluid (CSF) dynamics with secondary elevation of intracranial pressure represents an additional mechanism contributing to headache in bacterial meningitis. This typically results in posture- and Valsalva-sensitive pain that worsens with coughing, bending forward, or lying flat and is often most pronounced in the morning. In bacterial infections associated with inflammatory obstruction of cerebrospinal fluid pathways, such as Mycobacterium tuberculosis, this mechanism may contribute to severe or persistent headache phenotypes. These are typically dominated by features of intracranial hypertension. In tuberculous meningitis, headache is commonly described as diffuse (holocephalic, ~ 60%) and throbbing (48.4%), with varying levels of severity ranging from mild (23.2%) to moderate (23.2%), severe (36.8%), or even intolerable (16.8%) [2].
In suspected bacterial meningitis, lumbar puncture (LP) is essential to obtain cerebrospinal fluid (CSF) for analysis, including cell count, glucose and protein levels, Gram stain, and culture. Typical CSF findings include low glucose concentration, elevated protein, and neutrophil-predominant pleocytosis. Because CSF glucose reflects serum glucose, the CSF-to-serum glucose ratio is a more reliable diagnostic marker than absolute CSF glucose values. Microbiological confirmation is achieved by identification of the causative pathogen on Gram stain or culture [8, 11]. A non-contrast computed tomography (CT) scan should precede LP in patients at increased risk of cerebral herniation, such as those with papilledema, new-onset seizures, focal neurological deficits, or immunosuppression. LP should be deferred in clinically unstable patients or in the presence of significant coagulopathy; however, empirical antibiotic therapy must not be delayed. Blood cultures are recommended, as concurrent bacteremia is present in approximately 53% of cases [13,14,15]. Multiplex polymerase chain reaction (PCR) assays performed directly on CSF provide a rapid alternative diagnostic approach, demonstrating high sensitivity and specificity (> 90%) for common bacterial pathogens (e.g., S. pneumoniae, N. meningitidis, H. influenzae, S. agalactiae), even when conventional cultures are negative [16].
Viral MeningitisViral meningitis is a common cause of secondary headache and is classified in the ICHD-3 under headache attributed to viral meningitis or encephalitis. The clinical onset is typically acute or subacute and is often preceded by a flu-like prodromal phase. The most frequent symptoms include headache, fever, and neck stiffness. Headache is usually moderate to severe in intensity, commonly frontal, retro-orbital, or holocranial, and is frequently accompanied by nausea, photophobia, and malaise. These features reflect meningeal irritation and the associated inflammatory response [1]. The ICHD-3 describes the headache phenotype in viral meningitis as holocranial or nuchal, often associated with neck stiffness, clinically overlapping with bacterial meningitis but generally following a milder course [5]. Compared with bacterial meningitis, viral meningitis generally follows a milder clinical course [2].
In viral meningitis, cerebrospinal fluid (CSF) typically demonstrates a mild to moderate pleocytosis (approximately 80–100 cells/µL) with lymphocytic predominance (> 80%). In the early phase of disease, however, neutrophil-predominant pleocytosis may be observed before evolving toward a lymphocytic pattern. Glucose and protein concentrations are generally within normal limits [17]. Importantly, CSF lymphocytosis accompanied by headache is not specific to viral meningitis and may also be seen in partially treated bacterial meningitis, Mycoplasma pneumoniae, Listeria spp., brucellosis, spirochetal and rickettsial infections, tuberculosis, as well as fungal or parasitic diseases [18]. Non-infectious causes should likewise be considered, including drug-induced aseptic meningitis (e.g., NSAIDs, antibiotics, immunosuppressants, intravenous immunoglobulins, chemotherapeutic agents), chemically induced meningitis, and meningitis associated with systemic inflammatory or infiltrative conditions such as vasculitis, sarcoidosis, connective tissue diseases, or meningeal carcinomatosis [19]. Polymerase chain reaction (PCR) analysis of CSF remains the diagnostic gold standard for confirming viral meningitis, allowing sensitive and specific detection of viral DNA or RNA [19,20,21].
EncephalitisIn contrast to meningitis, which involves inflammation of the meninges, encephalitis refers to inflammation of the brain parenchyma itself. While the process is often diffuse, it may also localize to specific regions, such as the medial temporal lobes in cases of herpes simplex encephalitis. Clinically, encephalitis usually presents as an acute febrile illness characterized by headache along with varying degrees of altered mental status, seizures, and/or focal neurological deficits [22].
Encephalitis can result from a primary infection caused by viruses, bacteria, fungi, or parasites, or may develop secondarily following a prior viral illness or vaccination. While the majority of encephalitis cases stem from primary viral infections, the causative pathogen can be definitively identified in only a subset of patients [22, 23]. Common viral agents include herpes simplex virus, other herpesviruses (such as varicella-zoster and Epstein-Barr), adenoviruses, influenza A virus, enteroviruses, and various arboviruses (e.g., Japanese encephalitis virus, St. Louis encephalitis virus, and West Nile virus). Nonviral infectious encephalitis can be caused by a range of pathogens, including bacteria (such as Mycobacterium tuberculosis, Mycoplasma pneumoniae, Listeria monocytogenes, Borrelia burgdorferi, Leptospira spp., Brucella spp., Legionella spp., Tropheryma whipplei, and Treponema pallidum), rickettsiae (e.g., Rickettsia rickettsii, Coxiella burnetii, and Ehrlichia spp.), fungi (e.g., Cryptococcus spp., Aspergillus, and Coccidioides), and parasites (e.g., Plasmodium falciparum, Toxoplasma gondii, or Trypanosoma spp.) [22]. A comprehensive discussion of these etiologies is beyond the scope of this article.
Although encephalitis most often presents with focal neurological deficits and cognitive disturbances, headache may occur early, particularly in the presence of meningeal involvement or associated cerebral vasculitis, and in some cases may represent the initial or sole clinical manifestation. The headache phenotype reflects combined parenchymal and meningeal involvement and should be interpreted within the general pathophysiological framework outlined in Sect. 2.2 [1].
Encephalitis-related headache is typically diffuse, often frontal or retro-orbital, severe or extremely intense, and may present as throbbing or pressure-like pain, sometimes accompanied by neck stiffness when meningeal irritation is present [2].
In viral encephalitis, lumbar puncture may reveal elevated opening pressure. Cerebrospinal fluid analysis typically shows lymphocytic pleocytosis, a mild increase in protein, and normal glucose levels. While brain magnetic resonance imaging (MRI) can appear normal, pathogen-specific changes, particularly in herpes simplex virus (HSV) encephalitis are frequently observed. Electroencephalography (EEG) abnormalities are observed in over 80% of cases, most commonly diffuse slowing and/or focal epileptiform discharges. In selected patients, continuous EEG monitoring is required to detect non-convulsive status epilepticus [23].
Brain AbscessBrain abscesses are localized intracerebral infections characterized by a collection of pus and inflammatory cells, most often caused by bacteria or fungi. They represent a serious medical condition with significant risk for neurological sequelae and mortality, even with appropriate treatment. Mortality has declined over recent decades but remains notable. Abscesses may arise secondarily after neurosurgical procedures or primarily via hematogenous spread from distant infections, such as sinusitis, otitis, dental or pulmonary infections [24].
Headache is the most frequently reported initial symptom in brain abscesses. Other common clinical signs include confusion, altered mental status, nausea, vomiting, focal neurological deficits, fever, and seizures. Although the classic triad of headache, fever, and focal neurological signs is well known, it is uncommon at the time of presentation. From a headache perspective, brain abscess typically manifests as a subacutely evolving space-occupying lesion, consistent with the general mechanisms discussed in Sect. 2.2 [1].
Headache associated with brain abscess is reported in approximately 49–81% of cases and is usually progressive and localized. It is commonly exacerbated by coughing or Valsalva maneuvers, reflecting increased intracranial pressure and local mass effect [25].
Radiologic imaging plays a crucial role in diagnosis. Contrast-enhanced MRI is the modality of choice, typically revealing ring-enhancing lesions with surrounding edema and mass effect. CT scan may be used as an initial screening tool, especially in acute settings. Diffusion-weighted imaging (DWI) helps differentiate abscess from necrotic tumors. In uncertain cases, stereotactic aspiration may provide both diagnostic material and therapeutic benefit [26].
Subdural EmpyemaSubdural empyema is a rare, but life-threatening intracranial infection characterized by purulent collection between the dura mater and arachnoid mater. It typically presents with severe, often lateralized headache, fever, focal neurological deficits, and seizures, and constitutes a neurosurgical emergency. In infants, it most commonly complicates meningitis, whereas in older children and adults it usually results from contiguous spread of sinusitis, otitis media, or mastoiditis, particularly via the frontal or ethmoid sinuses. Intracranial extension may occur through venous thrombophlebitis or direct bony erosion, while hematogenous spread or post-traumatic and post-surgical cases are less frequent. Causative organisms generally reflect the source and include anaerobes, Streptococcus spp., Staphylococcus spp., Haemophilus influenzae, Streptococcus pneumoniae, and gram-negative bacilli [1, 6]. The headache phenotype reflects combined meningeal inflammation and local mass effect [2, 6].
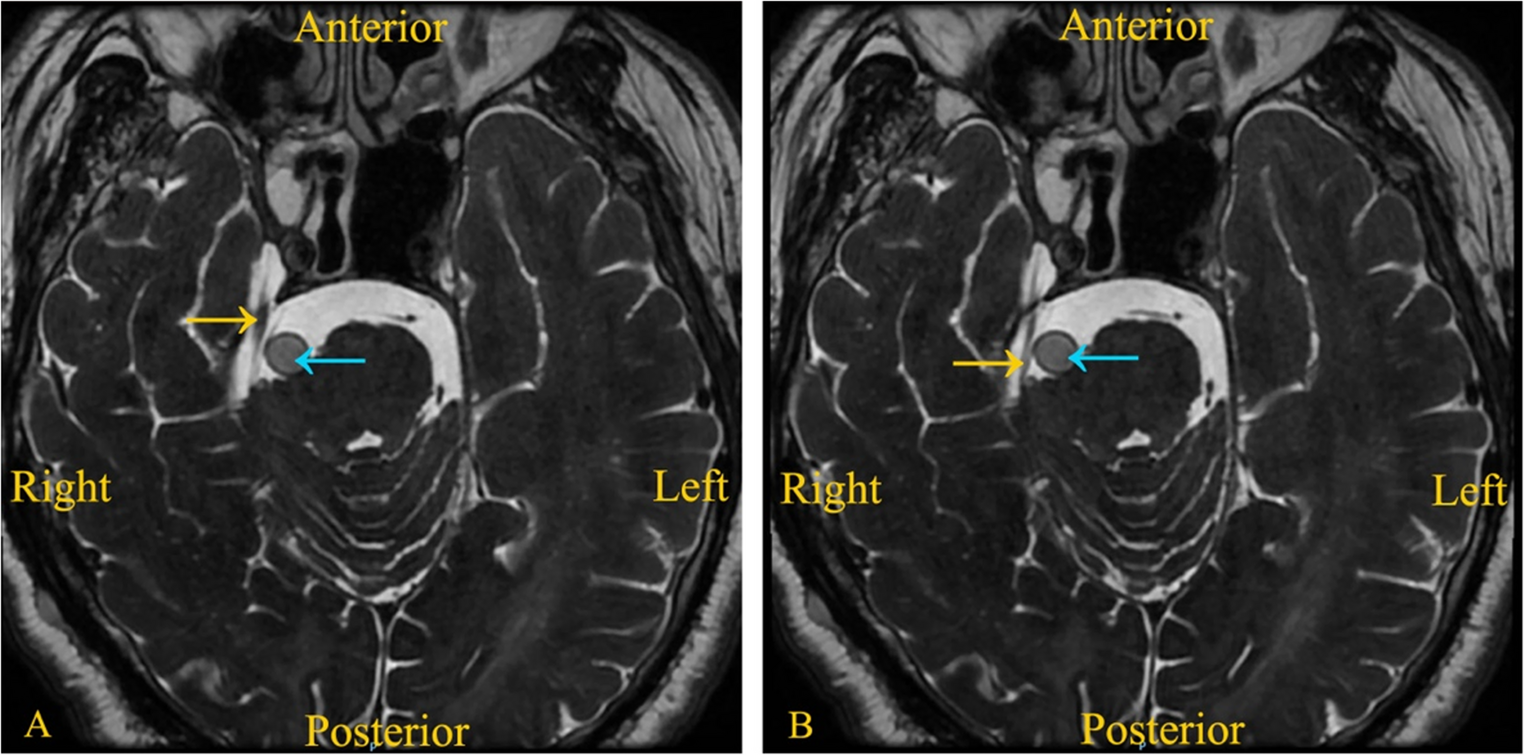
MRI with gadolinium contrast is the preferred modality for diagnosing intracranial subdural empyema. Contrast-enhanced MRI clearly delineates even small or interhemispheric collections, typically appearing as crescent-shaped hypointensities on T1-weighted images. DWI offers superior sensitivity and should be routinely included [27].
Headache Attributed to Intracranial Fungal or Parasitic InfectionIntracranial fungal or parasitic infections represent a rare but clinically relevant cause of secondary headache, categorized as ICHD-3 9.1.3. This diagnosis should be considered in immunocompromised patients and those exposed to endemic pathogens. The pathogenesis is typically related to inflammatory responses within the meninges or brain parenchyma, with or without associated mass effect or increased intracranial pressure [5, 6].
Cryptococcus neoformans is the most frequently implicated fungal pathogen in immunocompromised hosts, especially in HIV/AIDS patients. Its tendency to accumulate in the arachnoid granulations and obstruct CSF outflow can lead to raised intracranial pressure and chronic daily headache. Unlike bacterial meningitis, the CSF profile may reveal mild lymphocytic pleocytosis with elevated opening pressure and positive cryptococcal antigen testing. Other fungal agents, such as Aspergillus or Candida species, may cause cerebral abscesses or vasculitic complications, particularly in neutropenic or post-transplant patients. Invasive fungal infections may produce focal neurological deficits, seizures, or altered mental status, depending on the site of involvement [2, 5, 6].
Among parasitic infections, neurocysticercosis is the most common parasitic infection of the central nervous system worldwide and a frequent cause of secondary headache, particularly in endemic regions [28]. The pain may be associated with cyst degeneration, perilesional edema, or hydrocephalus due to ventricular obstruction. Other parasitic infections, including echinococcosis and toxoplasmosis, are less common but may mimic space-occupying lesions with raised intracranial pressure. Neuroimaging plays a central role in diagnosis, with characteristic findings such as cystic lesions, calcifications, perilesional edema, or hydrocephalus depending on the stage of the parasite and host immune response. Serological tests (e.g., enzyme-linked immunoelectrotransfer blot for Taenia solium) and CSF analysis may support the diagnosis but lack sufficient sensitivity or specificity on their own [1, 2, 5, 6].
Headache Attributed to HIV/AIDSHeadache is reported in over 50% of individuals living with HIV/AIDS and may occur during both acute and chronic phases of infection, often as part of aseptic meningitis or related immune-mediated mechanisms. In the ICHD-3, headache attributed to HIV infection is listed as a distinct diagnostic entity in the Appendix, reflecting its specific clinical context rather than being classified solely as a subtype of headache attributed to infection [5]. In most cases, the headache phenotype resembles primary headache disorders typically bilateral, dull, and tension-type in nature, though migraine-like features are reported in a minority. Clinical studies suggest that headache severity and frequency are more closely associated with indicators of HIV disease activity namely CD4 + T-cell count and viral load than with infection duration or the extent of antiretroviral therapy [2, 5].
Although primary-like headaches are the most common, secondary causes must be carefully excluded, particularly in patients with advanced immunosuppression. Opportunistic infections such as cryptococcal meningitis and cerebral toxoplasmosis remain the most common secondary etiologies of headache in HIV-positive individuals. In such cases, the headache is usually accompanied by focal neurological signs or signs of raised intracranial pressure, and should be classified under the respective underlying condition [5].
Headache Attributed to Systemic InfectionHeadache is a common but often nonspecific manifestation of systemic infections. Typically, diffuse and mode
Comments (0)