
Remember me
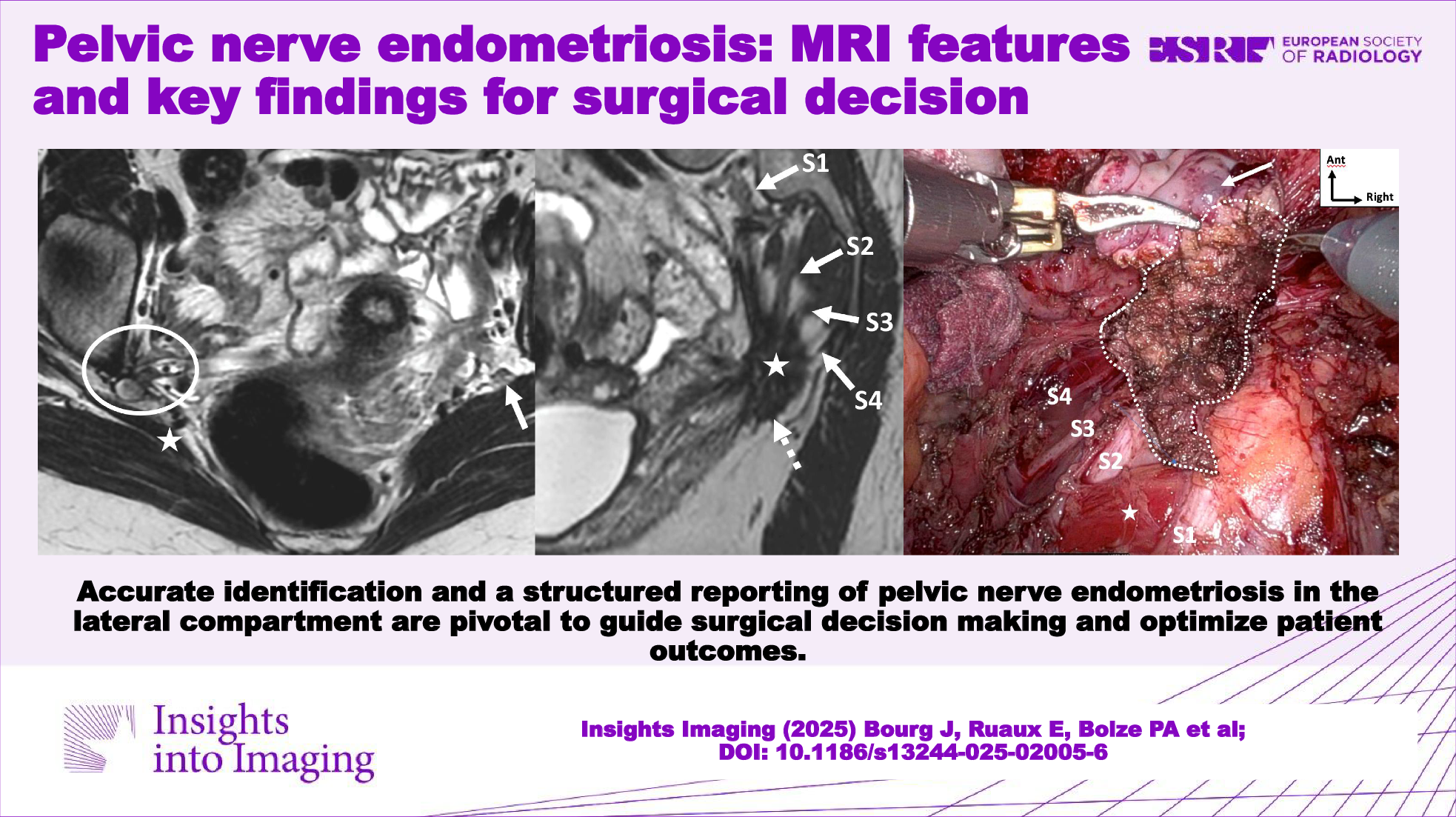

Accurate identification and a structured reporting of pelvic nerve endometriosis in the lateral compartments are crucial for guiding surgical decision making and optimizing patient outcomes (Table 1 and Fig. 1) [37].
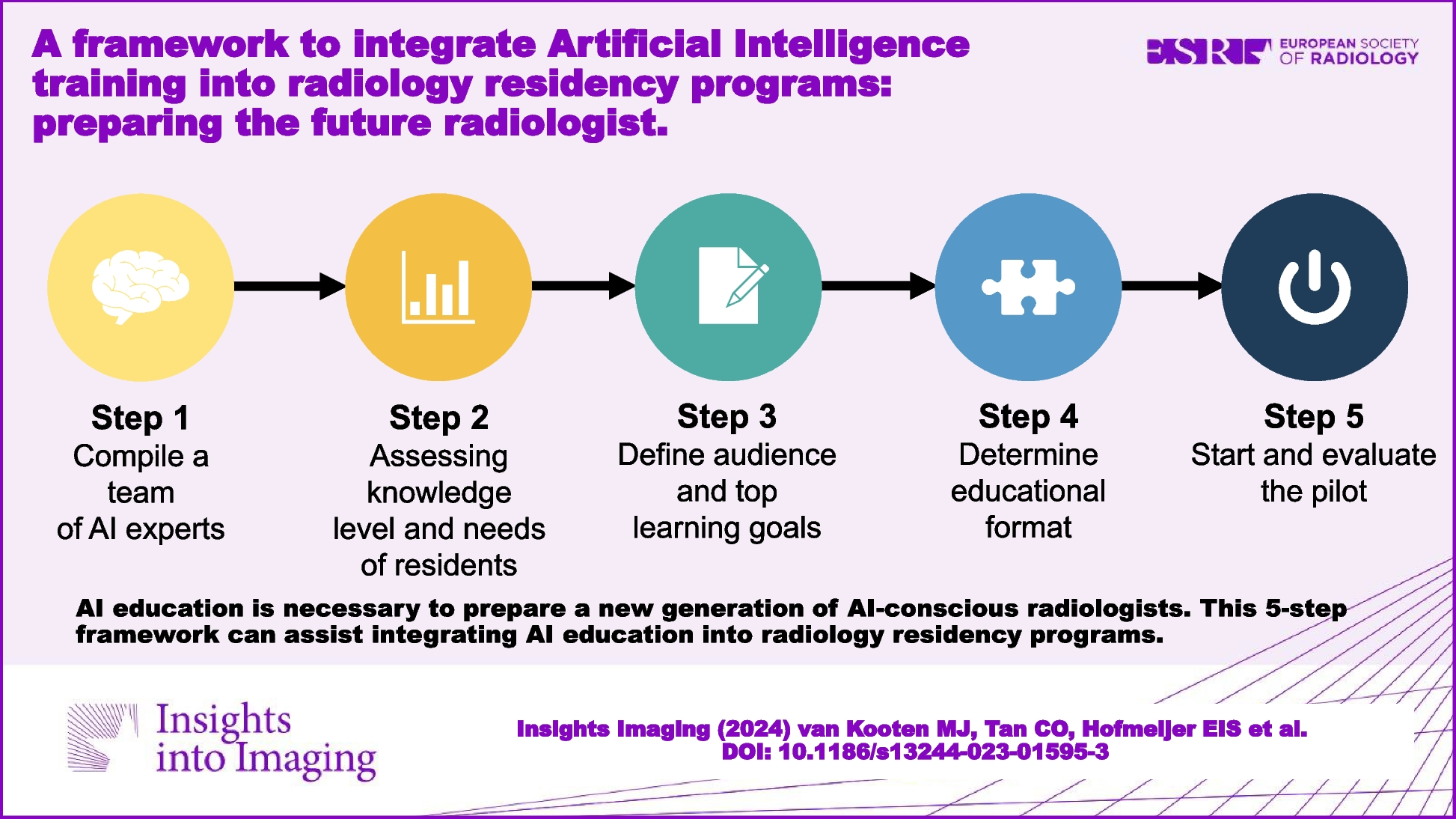
Table 1 Pelvic nerve endometriosis: anatomical landmarks, MRI features, and key points for surgical planningFig. 1
Anatomical illustration of somatic and autonomic pelvic nerves in a female pelvis (frontal view, adapted from Alkatout et al [37]). 1: inferior hypogastric plexus, 2: hypogastric nerve, 3: sympathetic trunk with chain of ganglia, 4: sacral roots (S1–S4), 5: sciatic nerve, 6: pudendal nerve, 7: obturator nerve, and 8: femoral nerve
Neural endometriosis lesions typically appear on MRI similarly to other DE lesions, presenting as T2-hypointense solid nodules or fibrotic thickenings. These lesions, may also show microcystic or hemorrhagic foci, indicative of active ectopic glandular tissue, and often involve the pelvic nerve, which may appear thickened, interrupted, or encased.
Inferior hypogastric plexusThe inferior hypogastric plexus is the most commonly affected structure within the lateral compartments in endometriosis [38]. This complex neural network provides autonomic innervation of the pelvic viscera. It is formed by the convergence of the hypogastric nerves (which arise from the superior hypogastric plexus), the pelvic splanchnic nerves (which arise from the anterior branches of the sacral roots S2–S4) and the sacral splanchnic nerves (which arise from the sacral sympathetic trunk at the S2 and S3 ganglia) [39]. The inferior hypogastric plexus branches into two main pathways: the anterolateral branch, which innervates the uterus and lower bladder, and a posteromedial branch, which targets the posterolateral aspect of the rectum and gives rise to the inferior rectal plexus [39].
The inferior hypogastric plexus spans from anterior to posterior through the lateral compartments, within the mediolateral and posterolateral parametrium (Supplemental Fig. 1) [40, 41]. It is located below the ureter and deep uterine vein, both of which serve as important landmarks during surgery [39]. It is typically characterized by a roughly triangular configuration with a posterior base (Supplemental Fig. 2) [40]. The sympathetic contingent (from the hypogastric nerves and S2–S3 ganglia) relaxes the detrusor muscle, contracts the internal urethral and anal sphincters, promoting continence. In contrast, the parasympathetic contingent (from the pelvic splanchnic nerves) stimulates the detrusor contraction, facilitating bladder emptying, and modulates the enteric nervous system of the left colon [40].
Thus, inferior hypogastric plexus involvement usually presents with vegetative symptoms such as bladder or rectal dysfunction (e.g., dysuria, bladder fullness, dyschezia) and vaginal dryness. Sometimes, catamenial sciatica occurs due to traction on the sacral roots via connecting splanchnic fibers. The plexus itself is not visible on MRI due to its complex, spiderweb-like structure. Therefore, understanding its relationship with the pelvic viscera and key anatomical landmarks is crucial. MRI typically shows infiltration from a large retrocervical lesion (torus uterinum and the proximal and/or distal uterosacral ligaments) to the sacrorectal septum of the posterolateral parametrium, with possible associated involvement of the mediolateral parametrium [42]. These lesions are often severe, with involvement of the rectal wall [43]. On MRI, they present as fibrotic nodular infiltration with low signal intensity on T2W, and loss of the normal aspect of the subperitoneal pararectal cellular sheet beneath the uterosacral ligament level and lateral to the mesorectal fascia [38]. Spiculated margins, particularly visible in the sagittal plane, allow assessment of the posterior extension to the sacral roots and deep extension to the iliococcygeus muscle of the levator ani (Fig. 2) [38]. Preoperative MRI is crucial for predicting postoperative complications, as excision of these lesions can lead to urinary and rectal dysfunctions, often due to damage to the inferior hypogastric plexus [44]. The MRI report should specify the distance and relationship of the endometriosis lesion to the ureter and uterine artery anterolaterally, to the sacral roots posteriorly, to the levator ani muscle inferiorly and the parietal pelvic fascia laterally, extending to the piriformis muscle and the branches of the gluteal and/or internal iliac vessels [38]. Extension to the sciatic nerve is rare.
Fig. 2
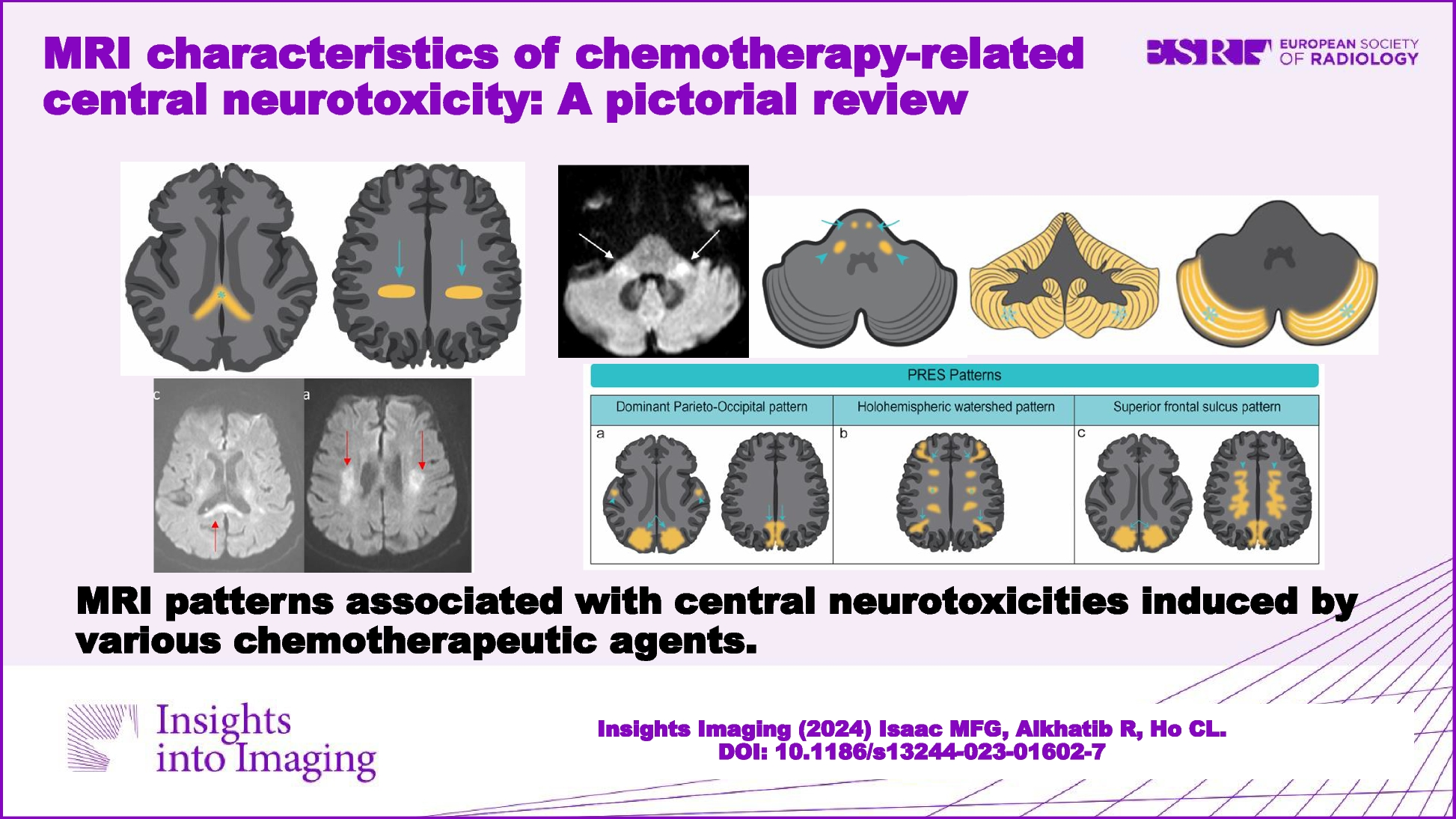
DE in a 29-year-old woman with dysmenorrhea, deep dyspareunia, and dyschezia. A Axial and (B) sagittal T2W MR images show a right subperitoneal infiltrative lesion (dotted lines) involving the anterolateral rectal wall and extending to the mesorectal fascia (A, white arrowhead) and beyond into the right posterolateral parametrium. The infiltration of the inferior hypogastric plexus shows spiculated margins (B, black arrows) but no extension to the sacral roots or the pelvic wall (A, dashed arrow). Note the safety fat line between the lesion and the iliococcygeus muscle of the levator ani muscle (B, white arrows). Laparoscopic surgery confirms the involvement of the inferior hypogastric plexus and a cleavage plane with the levator ani muscle and sacral roots
Sacral plexusThe sacral plexus, formed by the L4–S4 ventral rami, runs along the anterior surface of the piriformis muscle and serves as a significant anatomical landmark [45]. It provides motor and sensory innervation to the pelvis and the lower limbs.
On MRI, the sacral roots, although decreasing in caliber from S1 to S4, are well traced at the level of the foramen and at least in their proximal course (Supplemental Figs. 3 and 4). They extend inferiorly, above, through, or below the piriformis muscle and then towards the greater ischial notch, except for S4. The S2 and S3 nerve roots pass through the piriformis muscle in most cases [46], with an indentation within the muscle, which facilitates their visualization. However, in the distal course, the S3 and S4 roots are not or barely visible.
The symptomatology is polymorphic and depends on the affected sacral roots. It may include pudendal and gluteal pain, sciatica, pelvic organ dysfunctions such as bladder hyperactivity, urinary urgency, constipation, and dyschezia [47].
Sacral plexus involvement typically results from direct infiltration by a large retrocervical lesion with posterior extension to the inferior hypogastric plexus and then through the connecting pelvic splanchnic nerves.
On MRI, sacral roots may appear thickened with fibrotic infiltration, extending continuously with the sacrorectal septum infiltration. It mainly affects the roots S3 and S4 due to their lower, more posterior course (Fig. 3), whereas S1 and S2 are generally located above the endometriotic extension (Fig. 4) [47]. While surgical findings often reveal endometriotic traction or extrinsic involvement, accurately assessing the degree of infiltration on MRI remains challenging due to the small caliber of these sacral roots [12].
Fig. 3
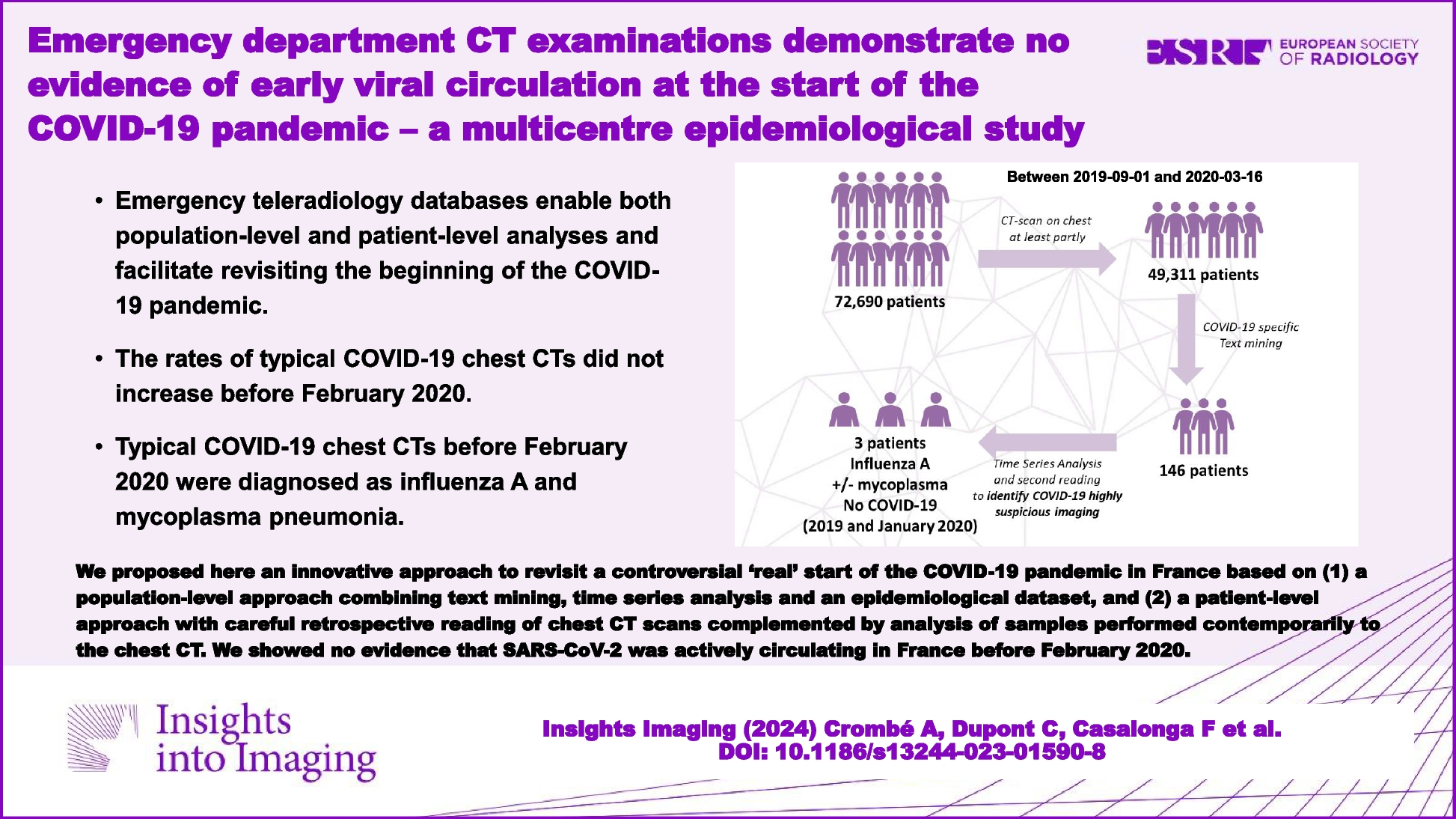
DE in a 42-year-old woman, with a history of rectal shaving 10 years ago, who presented with a recurrence of symptoms, in particular deep dyspareunia and right sciatica. A, B Axial T2 and (C) sagittal T2W MR images show right subperitoneal infiltrative lesion involving the anterolateral rectal wall (B, arrowhead), extending to the right posterolateral parametrium with inferior hypogastric plexus involvement (stars), up to the pelvic wall with encasement of hypogastric vessels (A, B, dashed arrows) and contact with the piriformis muscle. The posterior spiculated margins come into contact with the S3 and S4 sacral roots (C, arrows) and the posterior part of the right sciatic nerve (B, circle). D Axial fat-suppressed T1W MR image reveals T1-hyperintense endometriotic hemorrhagic microcysts (arrows). The surgical procedure confirmed extrinsic involvement and included a shaving of the right sacral roots and right sciatic nerve, as well as a section of the hypogastric vessels
Fig. 4
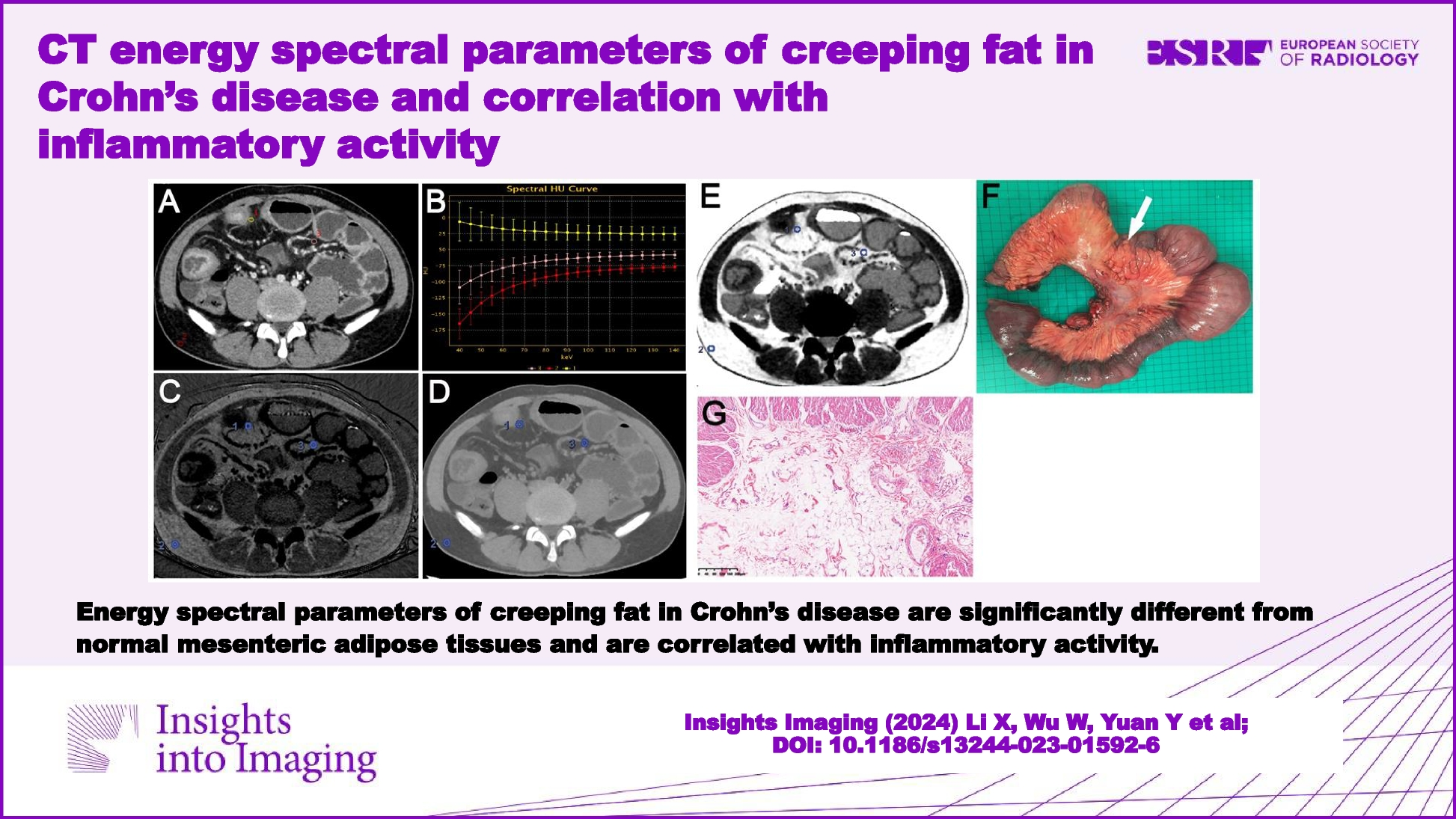
Severe endometriosis in a 31-year-old woman with dysmenorrhea, dyspareunia, and dysesthesia in the right lower extremity. A–C Axial 3D T2W images from top to bottom show endometriotic infiltration of the rectal wall (C, arrowhead) and posterior vaginal fornix (C, star), with complete extension to the right posterolateral parametrium including the inferior hypogastric plexus (black dashed arrows) with posterior attraction of S1 and circumferential involvement of S2, S3 and S4. Note the absence of extension of the ureter (B, C, white dashed arrow), the piriformis muscle, or internal iliac vessels. D Sagittal 3D reconstruction T2W image at the level of the right posterolateral parametrium showing involvement of the inferior hypogastric plexus (star) extending inferiorly to the levator ani muscle (dashed arrow), and posteriorly to sacral roots S2, S3, and S4, and with spiculation up to S1 but no involvement. E The robotic laparoscopic view shows a complete adhesion (white arrows) between the anterior rectal wall (star), the uterus and vagina, the peritoneal infiltration is being subperitoneal (dotted line). Note the hypogastric nerve (black arrow) passing through the inferior hypogastric plexus affected by the endometriosis and the course of the ureter (dashed arrows) distant from the endometriotic lesion. F The robotic laparoscopic photography view shows, after careful dissection, the upper part of the endometriotic lesion (dotted line) involving the rectal wall (star), S2, and partially attracting S1. Note the course of the ureter (dashed arrow). G Robotic laparoscopic view showing, after dissection of the endometriotic lesion (dotted line) from the rectal wall, involvement of the posterior vaginal fornix with a submucous hemorrhagic cystic component (arrow) after colpotomy, of S2, S3, and S4 and retraction of S1. Note the absence of involvement of the piriformis muscle (star). A complete nerve-sparing resection was performed, with S1 being retracted but removable from the lesion, and S2–S4 being circumscribed but without macroscopic intrinsic infiltration
Rarely, neural extension may progress along the sacral roots to the foramen, which can be better visualized on multiplanar sagittal plane reconstruction, especially in cases of hemorrhagic implants (Supplemental Fig. 5). In such cases, the lesion’s relationship with the foramen and the presacral fascia should be reported.
Sciatic nerveThe sciatic nerve, the largest peripheral nerve in the body, arises from the convergence of the ventral roots of L4–S3, anterior to the piriformis muscle. It exits the pelvis through the greater sciatic foramen, curves posteriorly above and out of the ischial spine, and runs laterally along to the common hamstring tendon between the ischial tuberosity and the greater trochanter [45]. It supplies motor innervation to the posterior thigh muscles and sensory innervation to the lower limb, except for the medial part.
On MRI, the sciatic nerve is clearly visible on both sides of the greater sciatic notch, with a “spaghetti-like” appearance. While its course is well traced in the axial plane, the coronal plane appears to be more relevant for detailed assessment (Supplemental Fig. 6).
The hallmark symptom is a cyclic sciatica associated with menstruation, and progressively shorter pain-free intervals. Patients usually report posterior thigh pain radiating down to the limb and the foot, sometimes accompanied by muscle weakness (foot drop), sensory loss, and reflex alterations [48].
Sciatic nerve involvement is typically identified at the sciatic notch [22]. It may result from endometriotic infiltration extending from the ovarian fossa towards the sciatic notch, or in a more isolated manner, without other identifiable pelvic endometriotic lesions. Isolated cases could be explained by the presence of a peritoneal diverticulum (pocket sign) [49] or the theory of perineural spread, especially in the absence of other endometriosis lesions.
MRI typically reveals fibrotic infiltration of the sciatic nerve, often with hemorrhagic cystic foci, leading to thickening and loss of its characteristic “spaghetti-like” appearance. In cases of chronic nerve involvement, fatty muscle atrophy may be observed, affecting muscles innervated by the sciatic nerve, such as those of the posterior thigh, leg, and foot [6, 50]. Atrophy also may affect the glutal and piriformis muscles, which are innervated by the posterior branches of the sacral plexus and have a close anatomical relationship to the sciatic nerve at the level of the greater sciatic notch. Similarly, the internal obturator muscle, innervated by the anterior branches of the sacral plexus, may be involved (Fig. 5). Muscle atrophy is mainly non-reversible and has a significant impact on the functional prognosis [51].
Fig. 5
DE in a 31-year-old woman with right catamenial sciatica. A Axial T2W MR image shows fibrotic thickening in the right sciatic notch involving the right sciatic nerve (circle) with loss of its spaghetti aspect compared to the left sciatic nerve (arrow). This lesion is isolated without involvement of the ovarian fossa or the sacrorectal septum, and could illustrate the potential existence of a peritoneal diverticulum. Note the hypertrophy of the piriformis muscle (star). B Axial fat-suppressed T1W MR image shows diffuse T1-hyperintense endometriotic hemorrhagic microcysts (dashed arrow). C Axial T2W MR image shows fatty atrophy of the right obturator internus muscle (black arrow), indicating a concomitant involvement of the nerve to the obturator internus muscle passing through the sciatic notch. The patient was medically treated with an LHRH analog
Assessing intrinsic or extrinsic nerve involvement remains challenging on MRI. However, intraneural endometriosis may be suspected when the sciatic nerve appears abnormally thickened and hyperintense on T2W MR images, with visible interruption and fiber discontinuity (Fig. 6) [50].
Fig. 6
DE in a 31-year-old woman with right sciatica initially cyclical, then became chronic with walking difficulties. A Axial and (B) coronal T2W MR images show an infiltrative endometriotic mass of 5 cm (measure not shown) (dotted line) centered on the right sciatic notch with involvement of the sciatic nerve. Note the hypertrophy of the piriformis muscle (A, star). C Axial fat-suppressed T2W MR image shows denervation of the gluteus medius and minimus muscles (stars), indicating the involvement of the superior gluteal nerve in the sciatic notch, as well as the piriformis muscle. D Axial fat-suppressed T1W MR image shows a right-sided endometrioma (arrow) and hemorrhagic implants of the left ovary (dashed arrow). Surgical intervention was not possible due to the intrinsic involvement of the sciatic nerve, which could risk nerve damage. The patient was treated medically with an LHRH analog
In the preoperative assessment, it is crucial to report the lesion’s size, its relationship to the obturator nerve and the inferior gluteal vessels, and most importantly, its relationship to the greater sciatic notch and any extra-pelvic extension through the greater sciatic foramen. Indeed such cases, a combined laparoscopic and transgluteal approach may be necessary to achieve complete excision of the lesion and adequate neurolysis (or decompression) of the sciatic nerve [52].
In most cases, the nerves are embedded but not infiltrated within the epineurium, and complete release results in significant or complete relief of pain and motor issues [53]. However, if the lesion infiltrates the nerves within the epineurium, excision may involve the nerve itself, thereby increasing the complexity of surgery. Patients are more likely to experience neuropathic pain and sensorimotor disorders after surgery. Most patients with isolated sciatic nerve endometriosis who present motor symptoms, such as foot drop, experience little to no significant improvement [9, 53].
Pudendal nerveThe pudendal nerve is formed by the ventral rami of the S2-S4 nerve roots. It has a short intrapelvic course and exits the pelvis through the greater sciatic foramen, between the piriformis muscle and the ischio-coccygeal ligament. It then curves medially along and under the ischial spine before re-entering the pelvis through the lesser sciatic foramen. It joins the internal pudendal vessels and runs along the lateral ischiorectal fossa within the pudendal (Alcock’s) canal, bounded by the obturator fascia [45]. The pudendal nerve provides motor innervation to the levator ani muscle, clitoral muscles, external anal and urethral sphincters, as well as sensory innervation of the perineum and anus [54].
Even with 3DT2 sequences, the proximal pudendal nerve is not easily visualized. It is necessary to identify anatomical landmarks of its course in order to accurately diagnose its involvement. Namely, the nerve emerges at the junction of the middle and distal third of the piriformis muscle, then passes through an anatomical window between the sacrotuberous and sacrospinous ligaments. In Alcock’s canal, the pudendal vascular pedicle serves as the landmark (Supplemental Fig. 7).
Pudendalgia presents as perineal pain or burning sensation, often worsened by sitting. Other symptoms, such as dyspareunia, dyschezia, or dysuria, are also commonly reported.
The pudendal nerve is primarily involved at three different levels.
At the level of the piriformis muscle, proximal pudendal nerve involvement may result from infiltration of the inferior hypogastric plexus, with posterior extension to the S3 and/or S4 roots (Fig. 7).
Fig. 7
DE in a 29-year-old woman with deep dyspareunia and left pudendalgia. A–C Axial and (D) sagittal T2W MR images show fibrotic nodular infiltration of the left posterolateral parametrium (stars) extending to the pelvic wall and to the iliococcygeus muscle of the levator ani muscle (D, black arrows), involving the left inferior hypogastric plexus, the left sacral nerves courses S3 and S4, and the level of origin of the left proximal pudendal nerve (C, circle). The patient was treated medically with hormone therapy
At the level of the pelvic wall near the ischial spine, at the entrance of Alcock’s canal, mid-course of the pudendal nerve involvement is often more isolated. This may be associated with a peritoneal diverticulum, similar to sciatic nerve involvement (Fig. 8) [55]. It is essential to describe the lesion’s relationship to the pudendal vascular pedicle, the sciatic nerve, and the obturator internus muscle sling posterior to the ischial spine.
Fig. 8
DE in a 43-year-old woman with dyspareunia and perineal pain. A Axial and (B) coronal T2W MR images show an endometriotic lesion (circle) of the right distal mediolateral parametrium extending to the pelvic wall in contact with the pudendal vascular-nerve bundle at the level of arcus tendineus of the levator ani muscle (B, arrowhead). The right ureter passes quite widely inside this lesion (A, arrow). This lesion is located in front of the right ischial spine mark (A, dashed arrow) and the sciatic nerve. This lesion is isolated without involvement of the ovarian fossa or the posterolateral parametrium. C Axial fat-suppressed T1W MR image showing diffuse T1-hyperintense endometriotic hemorrhagic microcysts (arrows). The patient was treated medically with hormone therapy
At the level of the perineal region, pudendal nerve involvement may result from endometriosis of an episiotomy scar extending into the ischiorectal fossa (Fig. 9) [56]. MRI can assess DE pattern in this region and evaluate the lesion’s relationship to the levator ani muscle, obturator internus muscle, vagina and anal canal. However, episiotomy scar endometriosis remains rare and MRI is also crucial to exclude differential diagnoses such as granuloma, chronic inflammation, or anal fistula.
Fig. 9
DE in a 34-year-old woman with pudendalgia after vaginal delivery with forceps extraction and bilateral mediolateral episiotomy. A Axial and (B) coronal T2W MR images show a bilateral fibrotic infiltration (arrows) of the levator ani muscle at the level of the distal course of bilateral pudendal nerves, as well as infiltration of the left part of the vagina (A, arrowhead). C Axial fat-suppressed T1W MR image reveals some T1-hyperintense endometriotic hemorrhagic microcysts (arrows). D Axial T1W post-contrast MR image shows a better delineation of the left vaginal (sub) mucosal involvement (arrow). E Axial T2W and (F) axial fat-suppressed T1W post-contrast MR images show a right vulvar lesion (arrows) correlating with clinical photographs (G). The patient was treated medically with hormone therapy
Pain management in patients with pudendal neuropathy includes medical treatment with drugs (antidepressants or neuromodulators) and perineural injection of corticosteroids and lidocaine or bupivacaine [55]. In most cases, these injections offer temporary symptom relief. Pudendal nerve decompression surgery may be considered for patients who do not respond to medical treatment.
Treatment of episiotomy scar endometriosis may require surgical excision to minimize the risk of recurrence. Recently, image-guided percutaneous treatments using cryotherapy have been considered [57].
Lumbar plexusThe lumbar plexus is formed by the ventral rami of the L1–L4 nerve roots. It descends within or posterior to the psoas major muscle, anterior to the L2–L5 transverse processes, before exiting into the pelvis [45]. Key nerves arising from this plexus include the obturator nerve and the femoral.
Obturator nerveThe obturator nerve is formed by the ventral rami of L2–L4. It arises from the medial border of the psoas major muscle and descends along the pelvic brim. It joins the obturator vessels and passes through the superolateral aspect of the obturator foramen within the obturator canal [45]. The obturator nerve provides motor innervation to the adductor muscles of the hip and sensory innervation to the medial thigh and knee.
Although relatively small, this nerve is of sufficient caliber to be visualized on MRI, particularly using 3D T2W sequences. It is well depicted in its proximal course, medial to the psoas major at L5, and then follows a descending, anterior course to join the obturator vascular pedicle, which is easily identified by its characteristic flow void appearance (Supplemental Fig. 8).
Symptomatic obturator nerve endometriosis is rare and manifests with inner thigh pain, thigh adduction weakness, or difficulty in walking [58].
Endometriotic involvement of the obturator nerve is rare, it is commonly described in the obturator fossa [59,60,61,62]. It often results from the extension of a large endometriotic lesion from the ovarian fossa going through the mediolateral parametrium up to the obturator nerve (Fig. 10). MRI features include a retractile fibrotic infiltration with possible hemorrhagic cystic areas along the pelvic wall, tracking the course of the nerve. The MRI report should specify the relationship of the endometriosis lesion to the ureter and the obturator internus muscle. In chronic cases, nerve involvement may result in atrophy and fatty degeneration of the adductor muscles [59].
Fig. 10
DE in a 29-year-old woman with deep dyspareunia, right sciatica, pain in the right inner thigh, and difficulty in walking. A–C Axial and (D) coronal T2W MR images show subperitoneal endometriosis lesion along and from the right adnexa (A, B, white arrows), extending to the right distal mediolateral parametrium (C, D, dashed arrows) and to the right obturator nerve (
Comments (0)