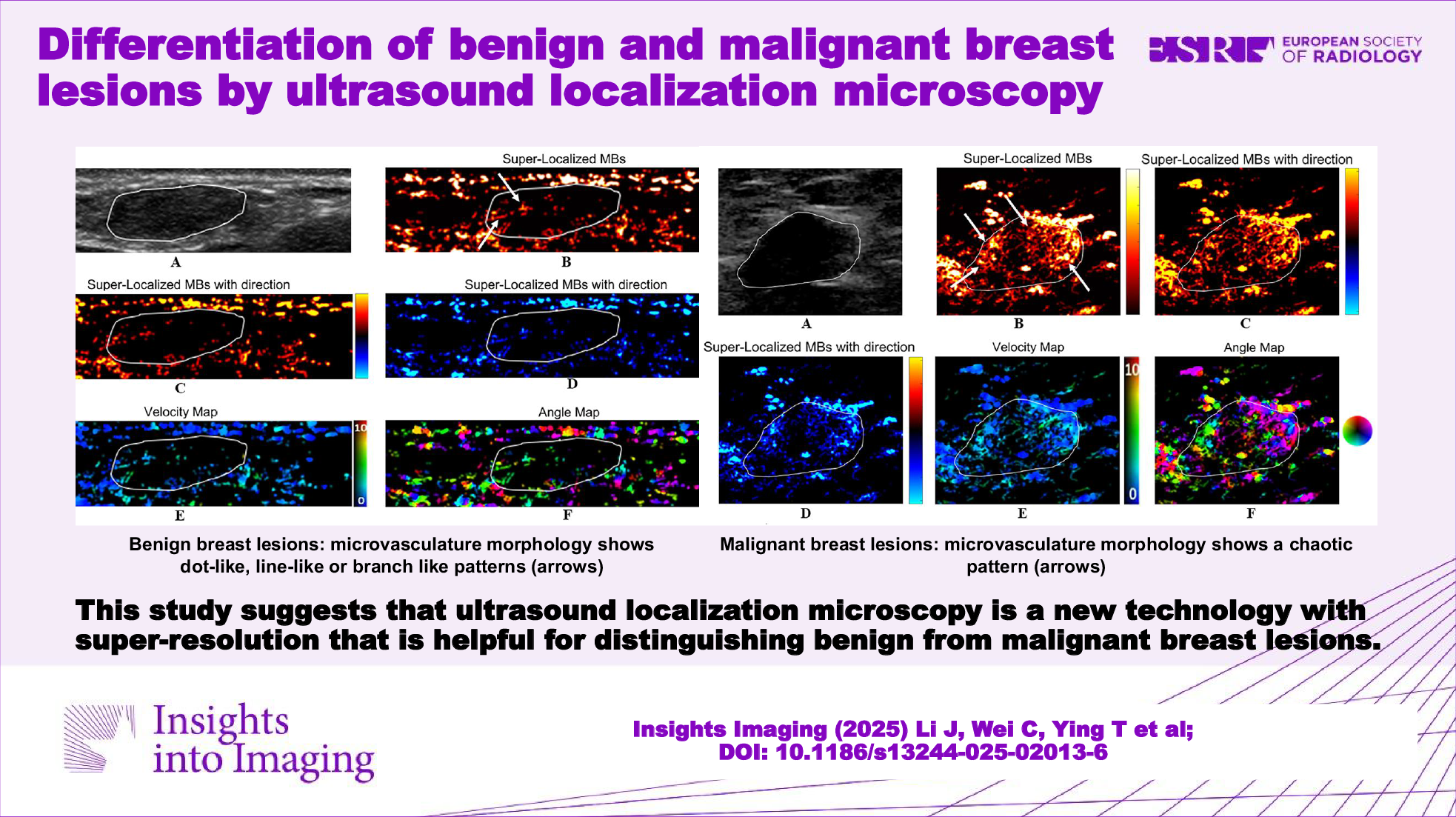
In the present study, the role of ULM qualitative and quantitative parameters in distinguishing benign from malignant breast lesions was evaluated. Our results revealed that dot-like, line-like, or branch-like patterns were significantly correlated with benign breast lesions and that chaotic patterns were significantly correlated with malignant breast lesions regarding qualitative parameters. With respect to quantitative parameters, the microvasculature density, mean diameter, largest diameter, and max tortuosity of malignant lesions were significantly greater than those of benign lesions; the microvasculature mean flow velocity of benign lesions was significantly greater than that of malignant lesions. Among quantitative parameters, the AUC was highest for the microvasculature’s largest diameter for the differentiation of breast lesions.
To date, the microvasculature morphology of ULM has not been studied in human breast lesions. Other US imaging techniques, such as CDFI, power Doppler imaging (PDI), superb microvascular imaging (SMI), and CEUS, have reported the value of vessel morphology in the differential diagnosis of breast lesions. However, the findings varied between studies. Gokalp et al [28] demonstrated that a line-like pattern was associated with benign breast lesions and that a branch-like or chaotic pattern was associated with malignant breast lesions using PDI. Diao et al [29] reported that a line-like pattern was present mainly in benign breast lesions, and a branch-like pattern was also present mainly in benign breast lesions with SMI and CEUS. They also revealed that vessel morphology was not significantly different between benign and malignant breast lesions according to the CDFI and PDI. Our study revealed that dot-like, line-like, or branch-like patterns were significantly correlated with benign breast lesions and that chaotic patterns were significantly correlated with malignant breast lesions using ULM. One possible explanation for the discrepancy in vessel morphology in different studies is the difference in US imaging techniques, resulting in different sensitivities to vessels. We further assessed the diagnostic performance of microvasculature morphology and found that it achieved a relatively high AUC (0.935), sensitivity (94.1%), and specificity (92.9%). These findings suggest that microvasculature morphology based on ULM can be a good indicator for the differential diagnosis of breast lesions.
Compared with conventional US imaging techniques, quantitative parameters based on ULM can not only obtain information at the microvasculature level but also directly compute these parameters. We evaluated seven quantitative parameters, including microvasculature density, mean diameter, largest diameter, mean tortuosity, max tortuosity, mean flow velocity, and max flow velocity. Among them, microvasculature density has become the gold standard for evaluating tumor angiogenesis [30]. In the present study, the microvasculature density of malignant breast lesions was significantly greater than that of benign lesions (p < 0.05). The result was in agreement with that of a previous study [26]. In fact, malignant breast lesions often exhibit hypervascularity [31, 32]. Thus, it is not surprising that malignant lesions have higher microvasculature density than benign lesions.
In this study, we found that the microvasculature’s largest diameter and mean diameter in malignant breast lesions were significantly greater than those of benign lesions (all p < 0.001). This can be attributed to the fact that dilated large vessels are commonly observed in malignant breast lesions [33]. These results were in line with those of a previous study by Gu et al [34] in which US high-definition microvasculature imaging was used. However, compared with that study, our study was superior in terms of the precision of microvascular measurement, as the microvascular diameter was measured on a micrometer scale. In that study, the microvascular diameter was measured in millimeters. In other words, ULM can offer more information on the microvasculature. Additionally, the diagnostic performance of the microvasculature's largest diameter and mean diameter was first evaluated in this study. We found that the AUC of microvasculature largest diameter was greater than that of microvasculature mean diameter (0.962 vs 0.941), suggesting that the diagnostic value of microvasculature largest diameter was better than that of microvasculature mean diameter.
Vessel tortuosity is used to assess the degree of vessel bending, which is likely correlated with growth factor-related alterations in the vessel wall, such as epithelial cell proliferation, changes in the basement membrane, and loss of pericytes and smooth muscle [35]. Other US imaging techniques have revealed that an increase in vessel tortuosity is significantly associated with malignant breast lesions [36, 37]. Ternifi et al [37] investigated microvasculature tortuosity, including microvasculature mean tortuosity and max tortuosity, using US high-definition microvasculature imaging and found that the microvasculature max tortuosity of malignant breast lesions was greater than that of benign lesions, but the microvasculature mean tortuosity was not significantly different. These findings are consistent with those in our study. However, our study was the first to evaluate the diagnostic performance of microvasculature max tortuosity and mean tortuosity. Similar to microvasculature diameter, the AUC of microvasculature max tortuosity was also greater than that of microvasculature mean tortuosity (0.727 vs 0.649), suggesting that the diagnostic value of microvasculature max tortuosity was better than that of microvasculature mean tortuosity. Based on the above results, more consideration needs to be given to the max values of microvasculature diameter and tortuosity.
Microvasculature flow velocity is another quantitative parameter obtained by ULM. In clinical practice, vessel flow velocity is often detected by Doppler US. However, Doppler US only detects fast flow (greater than 1 cm/s) [6]. In contrast, ULM is a new imaging method that has high sensitivity for detecting low flow. Furthermore, ULM can clearly visualize the magnitude of the microvasculature flow velocity of breast lesions by a velocity map. Evaluating the blood flow status of tumors accurately can help identify malignant tumors [38, 39]. Max flow velocity has been reported to be associated with the protein expression of genes related to angiogenesis in breast cancer. Niu et al [40] reported that the protein expression of VEDGF165, NRP-1, SphK1, CD31, YAP, CTGF, and Gli2 was positively correlated with the max flow velocity; however, the protein expression of PTEN and MFN2 was negatively correlated with the max flow velocity. Our study showed that the microvasculature max flow velocity was not significantly different for the classification of breast lesions (p > 0.05), which was inconsistent with the findings of a previous study [26]. Unlike the max flow velocity, the microvasculature mean flow velocity of benign breast lesions was significantly greater than that of malignant lesions (p < 0.05). To date, no studies have explored the diagnostic value of the microvasculature mean flow velocity based on US imaging between benign and malignant breast lesions in humans.
PTs and fibroadenomas of the breast need to be distinguished because they have similar features in terms of histopathology, clinical findings, and radiological findings [41]. Clinically, the approach to PTs and fibroadenomas includes different treatment modalities. In the US, classification of PTs and fibroadenomas is challenging because substantial overlap exists between the two diseases [42, 43]. In the present study, there was 1 case of benign PT and 8 cases of fibroadenoma. These lesions had different microvasculature morphologies on ULM. Benign PTs exhibited a chaotic pattern, whereas fibroadenomas exhibited dot-like, line-like, or branch-like patterns. These findings indicate that ULM could provide a new method for differentiating between benign PTs and fibroadenomas.
ULM, with the ability to provide high spatial resolution for visualizing microvasculature, has widespread potential clinical applications for managing breast diseases. For example, ULM can identify the richest area of vessels, which could be used to increase the accuracy of biopsy and decrease biopsy rates. Furthermore, ULM has the greatest value in appropriately identifying low-suspicion benign lesions, which have a high rate of misdiagnosis as malignant lesions on CEUS. In our study, six lesions were characterized as malignant lesions via CEUS, whereas ULM revealed a benign appearance. Therefore, ULM has the potential to reduce unnecessary biopsies of benign lesions. In addition, the intra- and inter-operator reliabilities of ULM quantitative parameters were excellent (ICC greater than 0.90) in our study. It is indicated that ULM is reproducible. However, ULM has several limitations. It is affected by the MB concentration and tissue motion, which play significant roles in localization accuracy. A high concentration of MB makes it difficult to identify each MB in successive frames [44]. For tissue motion, mild in-plane motion can be corrected, but relatively large motion is difficult to correct [8]. In this study, the reason for the suboptimal imaging was the high concentration of MB and the large motion due to patient cooperation. In this case, alternative techniques, such as CEUS and contrast-free super-resolution power Doppler (CS-PD) based on deep neural networks, can be considered for evaluating the microvasculature [45].
Our study had several limitations. First, a larger sample size is necessary, especially for analyzing diagnostic performance. Although 31 lesions were ultimately included in this study, the number of samples remained small, and a larger sample size will be necessary. Second, we performed the study with 2-dimensional US, which may not fully reflect the vessels of the whole lesion in comparison with 3-dimensional US. To obtain more vessels, we selected the plane with the richest density of vessels to perform CEUS examination and consequently to perform ULM.
In conclusion, ULM is useful for distinguishing benign from malignant breast lesions. ULM can offer a new diagnostic method for breast lesions, which deserves further research.


Comments (0)