
Remember me



Patient selection and inclusion followed STROBE statement guidelines for observational studies (see Supplementary Material—STROBE Checklist). Figure 1 presents the patient flow diagram detailing the screening, exclusion, and final analysis cohort.
Fig. 1
Flow diagram depicting patient selection and inclusion process according to STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement guidelines (see Supplementary Material—STROBE Checklist). The diagram shows the screening and selection process for diabetic ketoacidosis (DKA) admissions at Tawam Hospital, Al Ain, UAE, from January 2019 to December 2023.
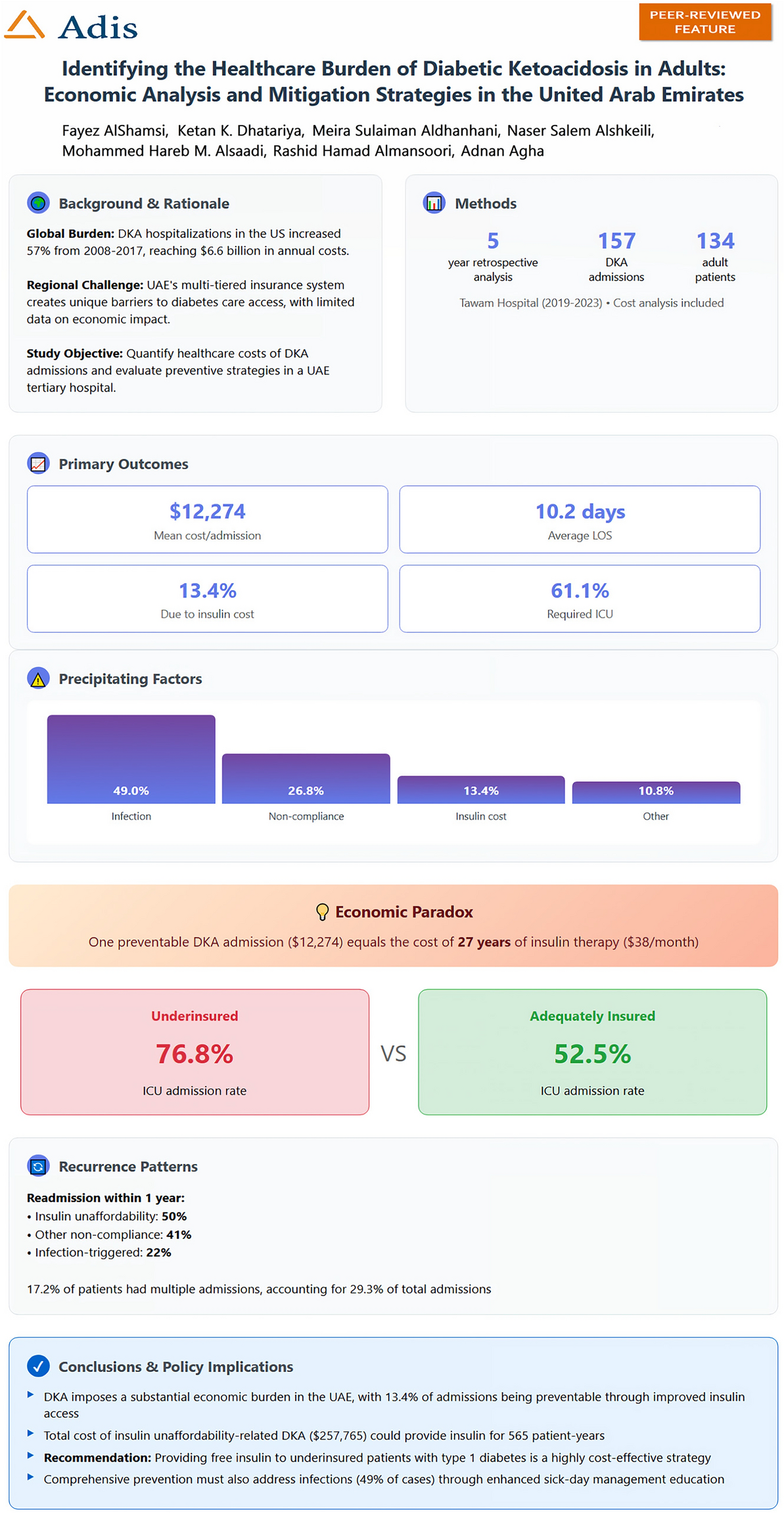
During this 5-year study period, 134 unique patients were admitted with DKA, accounting for 157 total admissions (mean 31.4 admissions/year, or one admission every 11.6 days). Among the 134 patients, 62 (46.3%) were male and 72 (53.7%) were female. Of these 157 admissions, 15 (9.6%) represented new-onset diabetes presenting as DKA, while 142 (90.4%) occurred in patients with previously diagnosed diabetes. The mean age was 36.4 ± 17.2 years. T1DM was present in 86 patients (64.2%), T2DM in 45 (33.6%), and other/unspecified diabetes in 3 (2.2%). Female patients had similar mean age (37.1 ± 16.8 vs 35.6 ± 17.6 years, p = 0.61) but showed trends toward higher HbA1c (10.8 ± 2.4% vs 10.2 ± 2.2%, p = 0.14) and ICU admission rates (64.6% vs 56.9%, p = 0.37) compared to male patients, though differences were not statistically significant. The median diabetes duration was 8.5 years (IQR 3–14 years). UAE nationals comprised 42.5% (57/134) of patients, with the remainder being expatriates from 23 different countries. See Table 1 for details.
Table 1 Demographics, clinical severity, and outcomes of patients admitted with DKA by insurance statusClinical Presentation and SeverityAt presentation, mean plasma glucose was 468 ± 156 mg/dL (26.0 ± 8.7 mmol/L), pH 7.14 ± 0.13, bicarbonate 10.2 ± 4.8 mEq/L, and anion gap 24.3 ± 6.2 mEq/L. DKA severity distribution was mild in 31 (19.7%), moderate in 88 (56.1%), and severe in 38 (24.2%) admissions. ICU admission was required for 96 admissions (61.1%), with mean ICU stay of 3.8 ± 4.2 days. Overall mean length of stay was 10.2 ± 11.7 days. Seven patients (4.5% of admissions) died during hospitalization, all with severe DKA and multiple comorbidities.
Economic BurdenThe mean total cost per DKA admission was 12,274 ± 10,213 USD (45,461 ± 37,826 AED), with a median of 9156 USD (33,902 AED). Daily hospitalization cost averaged 1203 USD (4457 AED). ICU-requiring admissions cost significantly more than ward-only care: 16,006 ± 10,847 USD (59,283 ± 40,171 AED) versus 6125 ± 3892 USD (22,685 ± 14,413 AED), p < 0.001. The cumulative 5-year cost for all DKA admissions was 1,927,018 USD (7,137,219 AED).
Precipitating FactorsInfections were the most common precipitating factor (77 admissions, 49.0%), followed by insulin non-compliance unrelated to cost (21 admissions, 13.4%), insulin unaffordability (21 admissions, 13.4%), new diabetes diagnosis (15 admissions, 9.6%), pump failure (6 admissions, 3.8%), and other/undetermined causes (17 admissions, 10.8%). See Table 2 for details on precipitating factors and their associated healthcare costs. Among the 21 admissions precipitated by insulin unaffordability, 18 occurred in unique patients, with 3 patients having repeat admissions for the same reason. These preventable admissions accumulated 257,765 USD (954,686 AED) in total costs over the study period. See Table 3 for more details regarding the 21 admissions related to insulin unaffordability as a primary precipitant.
Table 2 Precipitating factors for DKA admissions with associated healthcare costs (n = 157 admissions)Table 3 Analysis of DKA admissions secondary to insulin unaffordability in comparison with DKA admissions due to other reasonsInsurance Status and OutcomesComprehensive insurance coverage (government or enhanced private) was present in 101 admissions (64.3%), while 56 admissions (35.7%) involved underinsured patients. Underinsured patients had significantly higher rates of ICU admission (76.8% vs 52.5%, p < 0.01), longer ICU stays (5.2 ± 5.1 vs 3.1 ± 3.4 days, p = 0.02), and showed a trend toward higher mean costs (14,269 USD [52,847 AED] vs 11,133 USD [41,235 AED], p = 0.07). Notably, 75% (15/20) of insulin unaffordability cases occurred in underinsured patients. Figure 2 illustrates the healthcare impact of these preventable DKA admissions.
Fig. 2
Clinical and economic impact of preventable diabetic ketoacidosis due to insulin unaffordability (n = 21 admissions in 18 patients). a Economic comparison showing that the cost of one DKA admission [12,274 USD (45,461 AED)] equals 27 years of insulin therapy. b Clinical severity indicators demonstrate that preventable DKA is not mild, with high rates of ICU admission and severe acidosis. c One-year readmission rates vary significantly by precipitating factor, with insulin unaffordability showing the highest recurrence. d Resource utilization comparison reveals higher ICU usage and costs among preventable cases
Recurrence PatternsAnalysis of recurrence patterns revealed significant disparities based on precipitating factors and insurance status. During the 5-year study period, 23 of the 134 patients (17.2%) had multiple DKA admissions, accounting for 46 of the 157 total admissions. Among these 23 patients with recurrent DKA, 15 individuals (11.2% of all patients) had three or more episodes during the study period. These 15 high-utilizers with three or more admissions were predominantly young adults (mean age 32.4 ± 14.7 years) with T1DM (80%), limited insurance coverage (73.3%), and documented psychosocial challenges including depression (46.7%), substance use (20%), or unstable housing (26.7%).
Recurrence rates within 1 year varied dramatically by precipitating factor: among the 18 patients whose initial DKA was precipitated by insulin unaffordability, 9 (50%) were readmitted within 1 year, compared to 40% for other non-financial non-compliance and only 22% for infection-triggered DKA (p < 0.01). Insurance status was also strongly associated with recurrence: underinsured patients had a 43.8% readmission rate compared to 20.9% for adequately insured patients (p < 0.01).
Additional details are provided in Supplementary Tables S1 and S2.
Comments (0)