Although TBE was first reported as early as 1931 [22], and its clinical presentation is well characterized, precise and systematic data on CSF findings across different clinical manifestations or according to the duration of central nervous system involvement remain scarce. A PubMed literature search revealed only a few reports that link routine CSF parameters, predominantly protein concentration, to the severity of TBE [4, 5, 14, 23]. However, the severity of acute illness only roughly correlates with clinical manifestations. While meningitis is generally considered the mildest form of TBE, both meningoencephalitis and meningoencephalomyelitis can vary substantially in severity. As meningoencephalitis is considerably more common than meningoencephalomyelitis (with a ratio of nearly 11:1 in our cohort), its features dominate when findings are grouped by disease severity. Consequently, the question of which factors are associated with more severe acute illness is not equivalent to identifying factors linked to specific clinical forms of TBE.
The aim of this study was to assess and compare routine CSF findings in a large cohort of consecutive, well-defined adult patients hospitalized for TBE at a single institution, according to their principal clinical manifestations (meningitis, meningoencephalitis, or meningoencephalomyelitis). A further objective was to provide a detailed description of CSF abnormalities during the first 10 days after the onset of neurological signs or symptoms.
Clinical characteristics of the 717 consecutive TBE patients included in this study have been described elsewhere [20] and generally align with previously published data. However, compared with earlier reports [3, 6, 7, 14, 15], our cohort had a higher proportion of patients with meningoencephalitis and a lower proportion with meningitis.
The present analysis demonstrated that patients with meningitis were the youngest, had the lowest male predominance, were least likely to present with a monophasic disease course, and were least likely to have been vaccinated against TBE. In contrast, patients with meningoencephalomyelitis were the oldest, predominantly male, more likely to have a monophasic disease course, and most likely to present with breakthrough TBE.
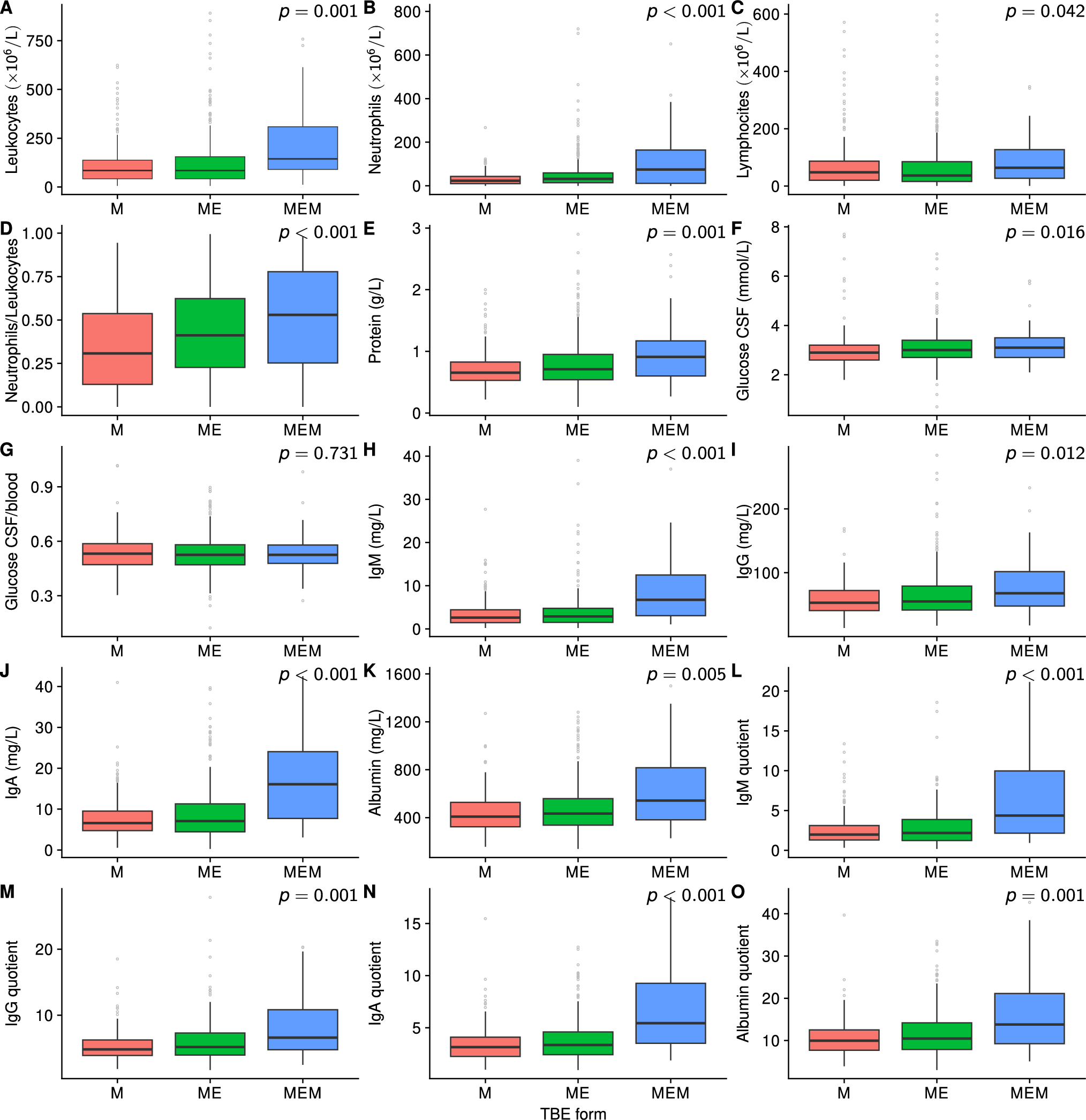
Among 15 routinely measured CSF parameters, significant differences were observed across the three clinical groups for all but the CSF/blood glucose ratio. Overall, CSF abnormalities were most pronounced in the meningoencephalomyelitis group and least in patients with meningitis. Notably, the CSF profiles of patients with meningoencephalitis more closely resembled those of patients with meningitis than those with meningoencephalomyelitis (Table 2, Fig. 1). Many differences between the groups were not only statistically significant but also clinically notable, with patients with meningoencephalomyelitis exhibiting 1.3- to over twofold higher or more abnormal values in most CSF parameters. The mechanisms underlying these differences are not yet understood. Two main explanations could account for the differences in CSF findings between different clinical manifestations of TBE: variations in pathophysiology and/or differences in the duration of neurological symptoms across groups. The median interval between the onset of neurological symptoms and lumbar puncture with CSF analysis was 5 days in patients with meningitis, and 4 days in both the meningoencephalitis and meningoencephalomyelitis groups. Although these between-group differences in symptom duration were small, they reached statistical significance, driven primarily by the longer duration in patients with meningitis. If the observed CSF differences were predominantly a consequence of symptom duration, one would expect the meningitis group to differ from both the meningoencephalitis and meningoencephalomyelitis groups, but not to observe differences between the latter two. For the abnormalities to be most pronounced in patients with shorter symptom duration (i.e., those with meningoencephalitis and meningoencephalomyelitis), they would need to peak within the first few days and then decline. However, most CSF abnormalities showed a different pattern: they increased over the first 4–5 days of neurological symptoms and subsequently either plateaued or gradually improved. Moreover, adjusting for sex, age, disease course (biphasic vs. monophasic), and duration of neurological involvement did not substantially alter the findings, suggesting that these variables are not the primary drivers of the observed distinctions.
A plausible, though simplified, explanation is that more pronounced inflammatory changes in meningoencephalomyelitis reflect the broader anatomical extent of central nervous system involvement – namely, that inflammation affects not only the meninges and brain but also the spinal cord. This may also be associated with differences in CSF flow dynamics in the spinal region. While this hypothesis could account for higher CSF protein, albumin, immunoglobulin levels, and corresponding indices, it does not fully explain the elevated leukocyte counts and, particularly, the more persistent and pronounced neutrophilic predominance observed in this group. These findings suggest that meningoencephalomyelitis may involve a distinct immunological or pathophysiological response compared to meningitis or meningoencephalitis.
When CSF findings were analyzed according to the duration of neurological symptoms, a consistent pattern emerged: most parameters were already abnormal on day 1, peaked between days 4 and 5, and then either plateaued or gradually declined through day 10. An exception was the proportion of neutrophils in the CSF. In the overall TBE cohort, as well as in patients with meningitis and meningoencephalitis, neutrophils predominated during the first two days, after which lymphocytes/monocytes became predominant (Fig. 4A). However, in patients with meningoencephalomyelitis, neutrophilic predominance persisted until day 5 and at higher absolute levels (Figs. 4B and 5), which indicates a different temporal evolution of CSF parameters in this subgroup. Nevertheless, on each day analyzed, CSF abnormalities were generally least pronounced in meningitis, slightly to moderately more pronounced in meningoencephalitis, and most pronounced in meningoencephalomyelitis.
The strengths of our study include the large number of TBE patients, prospectively collected clinical data, and rigorous application of clinical definitions. Nonetheless, despite the overall cohort size, the relatively small number of patients with meningoencephalomyelitis limits the robustness of day-by-day CSF analyses in this subgroup. Another limitation of the present study was concomitant Borrelia infection. Of 611 patients for whom the corresponding information was available, 22 (3.3%) patients with TBE also fulfilled criteria for concomitant definite Lyme neuroborreliosis [24]. Although rare, this concomitant Borrelia infection could potentially influence CSF findings in the present study; however, since Borrelia infections were approximately equally distributed among the three clinical presentations of TBE it is unlikely to have affected the comparative analyses between clinical groups. Additionally, because our study included only patients aged ≥ 15 years, findings may not be generalizable to pediatric populations. Lastly, all patients were from an endemic area where only the European subtype of TBE virus circulates; thus, our results may not fully apply to cases caused by other TBE virus subtypes.






Comments (0)