We show that Sample Entropy of overnight oxygen saturations has good discriminative accuracy to distinguish different forms of SDB. Sample Entropy SpO2 is simpler to measure as it only requires an oximeter compared to other diagnostic sleep disordered breathing parameters and thus has the potential to transform diagnostic pathways including in resource constrained settings including LMICs.
The significantly higher Sample Entropy SpO2 found in patients with sleep disordered breathing compared to normal sleep studies, is indicative of increased oxygen signal complexity and irregularity. This can be explained by the underlying pathophysiology of OSA, where patients have increased intermittent nocturnal hypoxia, leading to increased fluctuation of the oxygen saturation signal. Increased Sample Entropy SpO2 can also indicate enhanced engagement of physiological control system in response to hypoxia in OSA [9] which is compatible with our finding on Transfer Entropy analysis where HR → SpO2, RR → SpO2 and NF → SpO2 were higher in OSA than normal studies (Fig. 4). This is similar to previous work by Hornero et al., who found that the entropy of SpO2 was increased in patients with OSA. [17] While previous work has suggested that patients with OSA have decreased HR complexity, measured by Sample Entropy [18] and fuzzy entropy, [19] our work demonstrated no differences in the sample entropy of heart rate amongst the groups.
We found a strong positive correlation between AHI and Sample Entropy SpO2, which remained significant after adjustment for potential confounders. This suggests that patients with increasing severity of OSA have an increased Sample Entropy SpO2. This likely reflects patients with a higher AHI having increased nocturnal desaturations and thus increased complexity of the oxygen saturation signal. It also suggests that Sample Entropy SpO2 (using an SpO2 signal alone) can be used as a novel diagnostic tool in OSA.
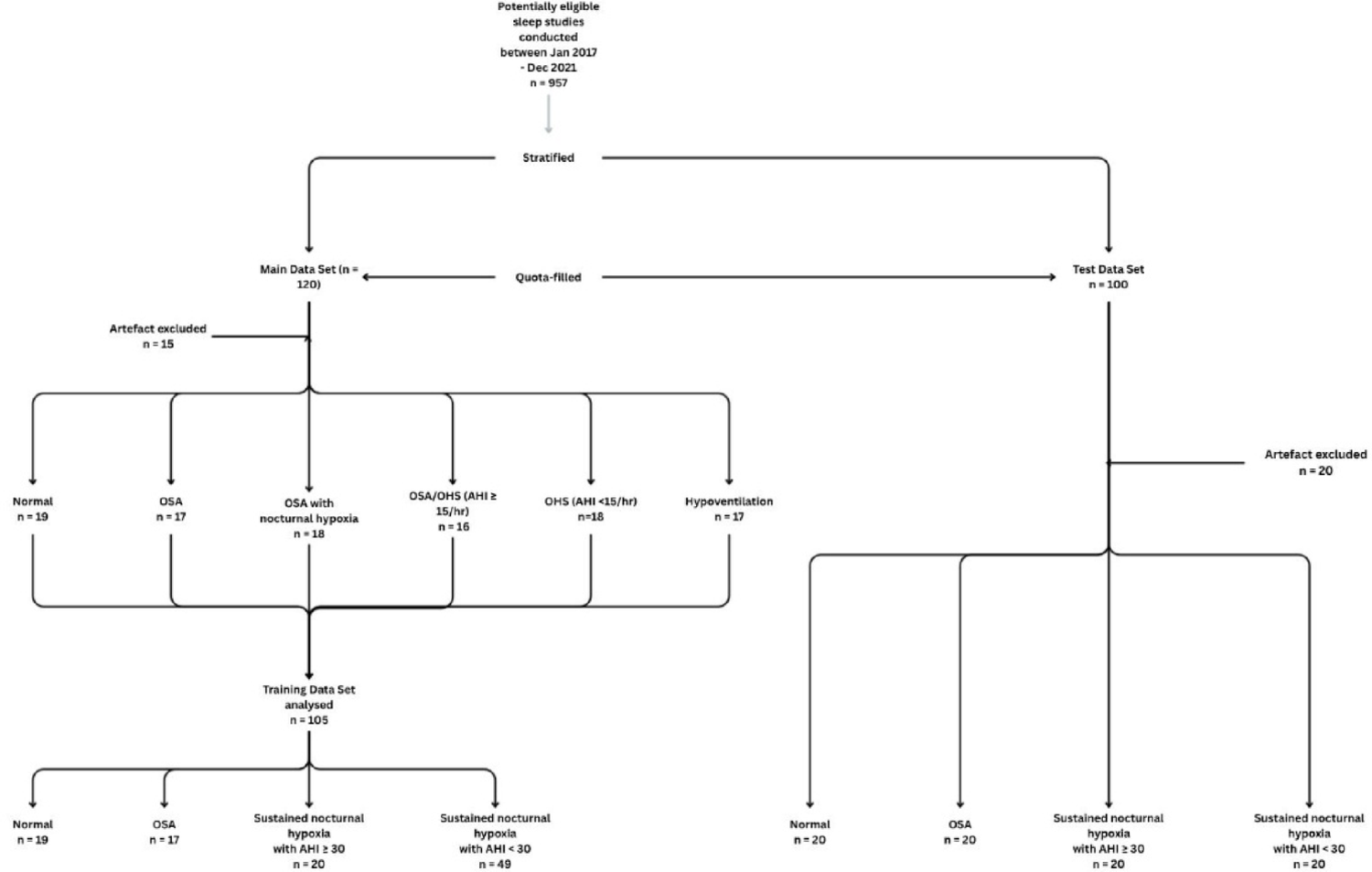
Our test data set included four groups. Two groups had a SpO2 time below 90% of < 30% and represented either normal studies or those with OSA alone. In the other two groups, patients had a SpO2 time below 90% of ≥ 30 and thus had sustained nocturnal hypoxia. These groups were then split based on AHI. Patients with sustained hypoxia and a low AHI (< 30events/hr) had significantly lower sample entropy of SpO2 compared to those with sustained hypoxia and a high AHI. This is significant as suggests reduced system engagement, increased regularity, and therefore a sicker patient population, for whom a different treatment strategy may be necessary. ROC analysis of the test dataset using Sample Entropy SpO2 showed high sensitivity and specificity in predicting OSA from normal studies (AUC 0.943) and from sustained hypoxia with a high AHI (≥ 30events/hr), and sustained hypoxia with a low AHI (AHI < 30 events/hr) (AUC 0.785).
It is important to note that Sample Entropy SpO2 and time spent below 90% can both be calculated simply from an overnight single-channel oximetry. While many centres globally use overnight oximetry to diagnose OSA, limitations include under-diagnosis, poor performance in co-morbid patients and limited diagnostic utility in the hypoventilation population. [20] However, they are more cost-effective and easily accessible. Therefore, finding other measures that can accurately diagnose sleep disordered breathing using overnight oximetry are important. Sample Entropy SpO2 and time spent below 90% can potentially differentiate between OSA phenotypes (mild vs. moderate/severe) and OSA phenotypes with sustained hypoxia (severe vs. non-severe). While further work in this field is necessary to understand the treatment implications of this and whether this translates to a pure OHS population, this work is promising and could increase availability of accurate sleep diagnostic testing globally in a manner that is more affordable and acceptable to patients, and potentially means that patients do not have to undergo blood gas testing. Our work is suggestive that the use of sample entropy with a measure of overnight ventilation (e.g., venous bicarbonate) may pave the way to non-invasive diagnostic measures and initial treatment strategies in people with OHS with or without OSA.
From our training data set cut-off values for Sample Entropy SpO2 were chosen to represent clinical importance, for example the value chosen to distinguish OSA from normal studies was 100% sensitive, so as not to miss any potential patients with OSA. The value chosen to distinguish sustained nocturnal hypoxia with a high AHI (≥ 30events/hr) from sustained nocturnal hypoxia with a low AHI (< 30events/hr) was 92% specific, such that there were few false positives. We validated this pathway on a different set of test patients and showed that a Sample Entropy SpO2 ≥ 0.1456 had 100% sensitivity and 60% specificity in predicting OSA from normal; and a Sample Entropy SpO2 ≥ 0.3504 had 60% sensitivity and 85% specificity for predicting sustained nocturnal hypoxia with a high AHI compared to hypoventilation with a low AHI. While this needs further validation in a larger dataset, it suggests that SE SpO2 is a useful potential future metric to aid both diagnosis and management of sleep disordered breathing with easy world-wide applicability.
To our knowledge, no prior study has looked at using Transfer Entropy to create a network physiology map in patients with sleep disordered breathing. This data supports the existence of multiple feedback loops and bi-directional interactions between nasal flow, heart rate, respiratory rate, and oxygen saturation during normal sleep. This highlights that sleep is not a passive state but involves significant information transfer between different physiological time-series that are dependently linked to each other.
Patients with OSA had significantly increased directed Transfer Entropy from HR → SpO2, RR → SpO2 and NF → SpO2; and significantly decreased Transfer Entropy from SpO2 → RR. The differences in information transfer between RR and SpO2 provide further evidence of an aberrant loop gain pathway that is known to exist in OSA. [21, 22] Ventilatory loop gain reflects the ratio between the ventilatory response to the disturbance, i.e., when breathing deviates from a normal level, the response of the system matches this to ensure status quo. However, in OSA, there is higher loop gain with a disproportionately larger response. [23] This may be reflected in an increase in information transfer from RR → SpO2 (i.e., larger response) and a decrease in information transfer from SpO2 → RR (i.e., reduced acknowledgement of the respiratory disturbance). Reduced information transfer between SpO2 → RR may indicate that hypoxia may not initially increase respiratory drive in OSA and gives pathophysiologic insight about the disease process using non-invasive method. Moreover, non-invasive assessment of loop gain is not currently straightforward in clinical practice, and our findings suggest that a Network Physiology approach has a potential application in assessment of loop gain function for individual patients, which can potentially lead to individualised treatment pathways in the future. Network physiological mapping could also lead to non-invasive endotyping of OSA which will also have an impact on treatment decisions and potentially open the door to other treatment strategies including medication.
Patients with sustained nocturnal hypoxia and non-severe OSA had significant increases in their directed Transfer Entropy nearly across the whole network map. This suggests a system that is stressed with increased information exchange. This provides further evidence that this patient group is likely to represent a more severe disease process with increased morbidity and mortality. Furthermore, Transfer Entropy between HR and SpO2 can be calculated from an overnight oximetry and therefore add and support a diagnosis of sustained nocturnal hypoxia and non-severe OSA compared to sustained nocturnal hypoxia with severe OSA.
There are some limitations to this work. Firstly, our dataset consists of mainly a UK white population, and the conclusions need to be tested in a more diverse dataset given we know that skin pigmentation can affect oxygen saturation measurement. [24] Second, the retrospective nature of this study, makes firm conclusions difficult and future prospective studies are needed. Third, all the sleep studies used a Nonin oximeter™ (Nonin Xpod Oximeter, USA) and it is possible that different oximeters may generate different sample entropy results. Fourth, as not all patients had blood gas measurements we were unable to draw conclusions on patients with OHS based on current standard guidance.
In conclusion, we have shown that Sample Entropy of oxygen saturation along with Transfer Entropy can help distinguish between different types of sleep disordered breathing. In combination with current widely used parameters such as mean saturations and time spent with saturation below 90%, this new metric has the potential to create a new, simplified and inexpensive diagnostic pathway for sleep disordered breathing.




Comments (0)