The findings of this study offer valuable insights into the acute safety profile of intravenous neridronate administration in young children with OI. Our results demonstrate that the first neridronate infusion was generally well tolerated, with no severe adverse events reported in our pediatric OI cohort. An APR characterized by fever and skeletal pain was commonly observed, but it was of short duration and self-limiting. Furthermore, chronic skeletal pain markedly improved shortly after the APR, once again underscoring the effectiveness of BPs as a treatment for chronic pain in severe OI.
BPs have been used for decades, primarily in adult populations, and are generally considered safe and well tolerated with few long-term side effects [14, 15]. However, bone is a highly dynamic and metabolically active organ that plays a central role in calcium homeostasis. By inhibiting osteoclastic bone resorption, BPs effectively suppress a major source of circulating calcium, which may cause transient hypocalcemia. We did not measure post-infusion calcium concentrations in our patients. However, patients were admitted for a brief hospital stay of 2–3 nights, and no clinical signs of hypocalcemia, including paresthesia, muscle cramps or seizures occurred. All our patients received calcium supplementation during the BP infusion, which potentially reduced the likelihood of hypocalcemia. Patients and caregivers were also instructed how to recognize typical symptoms of hypocalcemia after hospital discharge, and only six families reported mild muscle cramps, potentially as a sign of hypocalcemia. As described in literature, severe, symptomatic hypocalcemia is generally rare in patients receiving BPs, even after the first infusion []. However, it should be noted that in most studies, calcium supplementation was administered prior to or immediately after BP infusion, similar to our protocol.
In our cohort of BP-naïve pediatric patients with OI, transient flu-like symptoms, particularly fever and skeletal pain, were the most common side effects. Following this acute phase, mean pain levels, as assessed by pain scales, decreased below the baseline level, regardless of the severity of the disease. Families assessed pain levels during a period using the same analgetic treatment as before the BP treatment.
Chronic skeletal pain is a key contributor to reduced quality of life in children with OI and represents a relevant target for supportive treatment strategies [16]. The effectiveness of BPs in reducing chronic pain in these patients has already been described well in OI [17,18,19] as well as other skeletal and neuromuscular diseases [3, 20,21,22,23,24, 25].
The acute reactions we observed have also been described in children receiving BPs for other indications associated with bone loss [26], as well as in adults with OI receiving their first dose of neridronate [27] and are often summarized as “flu-like symptoms.” Consistent with the findings of this study, a previous investigation by Idolazzi et al. reported a transient reaction with fever and arthralgia following the initial dose of neridronate in children with OI [13]. A British multi-center trial reported a high frequency of mild APRs after the first dose of zoledronate, another nitrogen-containing BP, in children with OI and osteoporosis [18]. Nasomyont et al. reported 2019 infrequent and mild APRs in children with OI, which were more severe in patients with secondary osteoporosis [28].
The underlying mechanism of APRs likely involves BP-induced activation of peripheral blood mononuclear cells, prompting the release of pro-inflammatory cytokines such as tumor necrosis factor-alpha, interleukin-1, and interleukin-6 [29,30,31]. As a marker of inflammation, C-reactive protein (CRP) levels increase after BP infusion and are associated with the occurrence of flu-like symptoms [29]. Variations in the magnitude of this cytokine response may contribute to the heterogeneous presentation of symptoms between different patients. Patients with underlying systemic inflammatory diseases, e.g., CRMO, have longer and more pronounced APR than, for example, patients with OI [32]. APRs are more commonly observed with amino-containing BPs like neridronate and zoledronate, whereas non-nitrogen-containing BPs, like clodronate, may even exhibit anti-inflammatory properties [33, 34]. Furthermore, the APR seems to be most frequent after the initial infusion of BPs and occurs only rarely in subsequent administrations of BPs [28, 31].
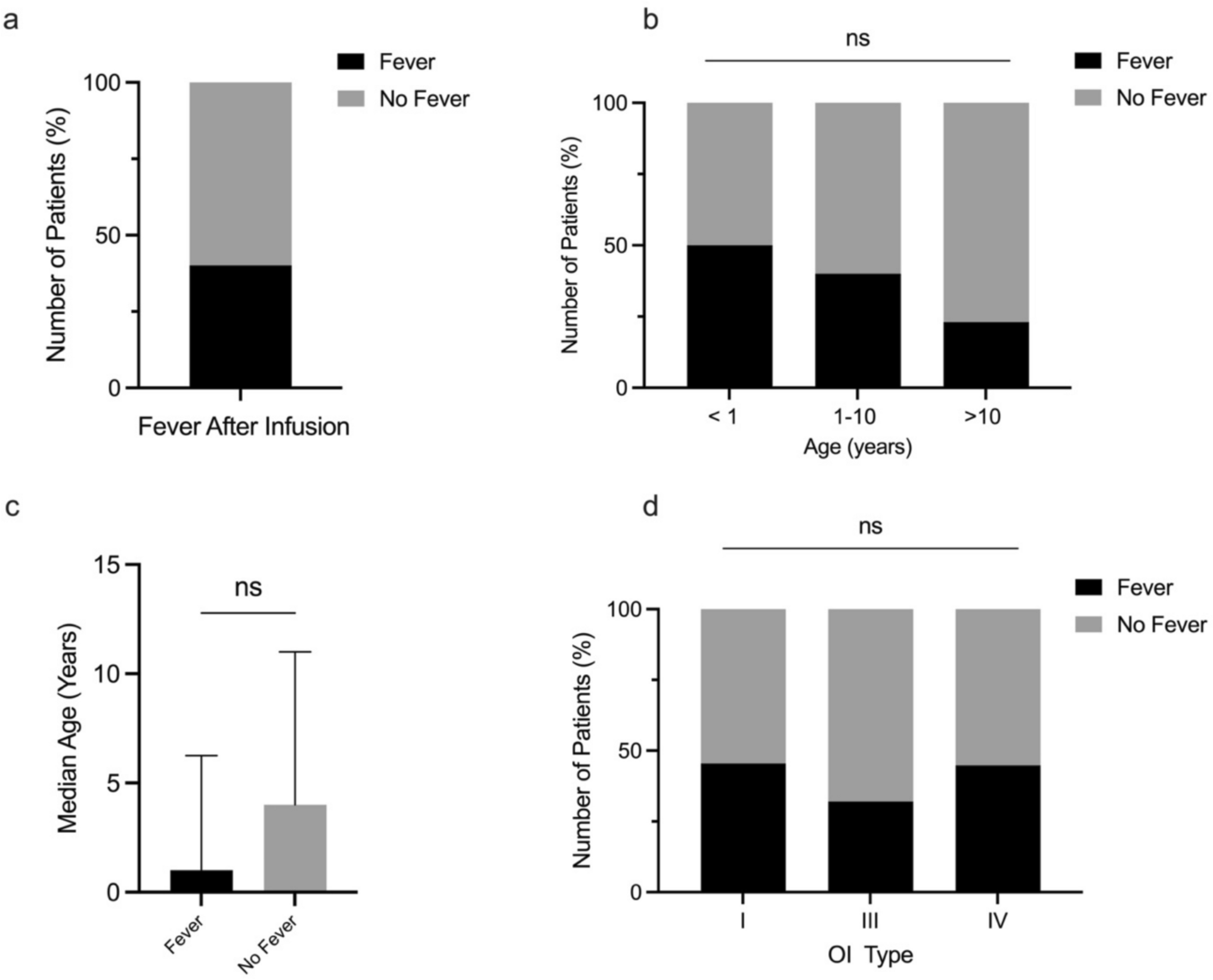
Despite administering the dose over 2 consecutive days to minimize this risk, 50% of infants in our cohort developed fever—most of them within the first 12 h—compared to only three patients older than 10 years. These results complement the study by Idolazzi et al. [13], which included only children aged 5 years and older and reported a lower incidence of fever, suggesting that APRs may be frequent in younger age groups. However, there was no statistically significant association between age and fever occurrence in our population. Therefore, patient age is not a reliable predictor for APRs after BPs. Nevertheless, even among our youngest patients, neridronate was generally well tolerated, with no severe adverse events observed.
We also investigated whether the severity of OI could be a predictor of the APR risk, but no correlation was found between OI severity and the occurrence of fever in our study. Other patient factors may influence the risk and severity of APRs after initial BP infusion and warrant further investigation. For example, low vitamin D levels prior to treatment may also be associated with more pronounced APRs [15]. Since vitamin D deficiency is highly prevalent, especially in children with chronic diseases like OI [32, 35], normalizing vitamin D levels prior to therapy start is mandatory to prevent hypocalcemia after BP infusion.
Our study has some important limitations. These include the single-center design and the limited generalizability to other BPs and patients with other bone disorders. Given the questionnaire-based design, the quality of the data depends on parental recall and the diligence with which the questionnaire was completed. In our youngest patients, the assessment of pain was only possible based on the observation of hospital staff and caregivers. Young children may be unable to reliably report pain scales, which may introduce reporting biases. A placebo-treated control group would be optimal to investigate the analgesic effects of BPs, although this is difficult in children due to ethical reasons. The questionnaire also collected information on post-discharge symptoms indicative of hypocalcemia. However, especially in very young infants, recognition of muscle cramps can be challenging, especially for parents. Future prospective studies with standardized adverse event reporting are warranted to validate these results and further elucidate the underlying mechanisms of the APRs to BPs.
However, our study reports from a relatively large cohort of children with OI, a rare genetic disorder. Since OI is still not well-known in all pediatric clinics and BPs are not yet approved for use in OI in most European countries, our data can help other clinicians with limited experience in pediatric BP use to gain confidence in administering this medication. Our findings underscore the importance of pre-infusion counseling for patients and caregivers regarding the potential for APR. Early treatment of fever or pain with acetaminophen or ibuprofen may mitigate these adverse effects and can improve patient comfort [36, 37]. Prophylactic medication is not indicated, since not every child develops an APR and we did not find a clear prognostic factor for who will. Given that the APRs are generally mild, we consider it reasonable to wait and identify which children actually develop a reaction, and then administer medication as needed to reduce fever and discomfort. Furthermore, monitoring younger patients closely for early signs of fever and pain can facilitate prompt management and enhance the overall treatment experience. Based on our data, we were able to reduce hospitalizations of the families. Inpatient admission is undertaken for general safety considerations during the initial administration of an unlicensed medication. Nevertheless, our data indicate that the treatment is safe and well tolerated. If no adverse reactions occur within the first 12 h following administration, patients can be safely discharged. Should mild reactions develop thereafter, they can be managed by caregivers, who receive intensive and repeated counselling during the inpatient stay. Providing comprehensive education on the anticipated course of such reactions further mitigates caregiver anxiety and facilitates adherence to the treatment regimen.





Comments (0)