
Remember me




We conducted a retrospective observational study including all patients diagnosed with Kawasaki disease (KD) at the University Hospital “Marqués de Valdecilla” (Santander, Spain), a tertiary pediatric referral center, between January 1994 and December 2024.
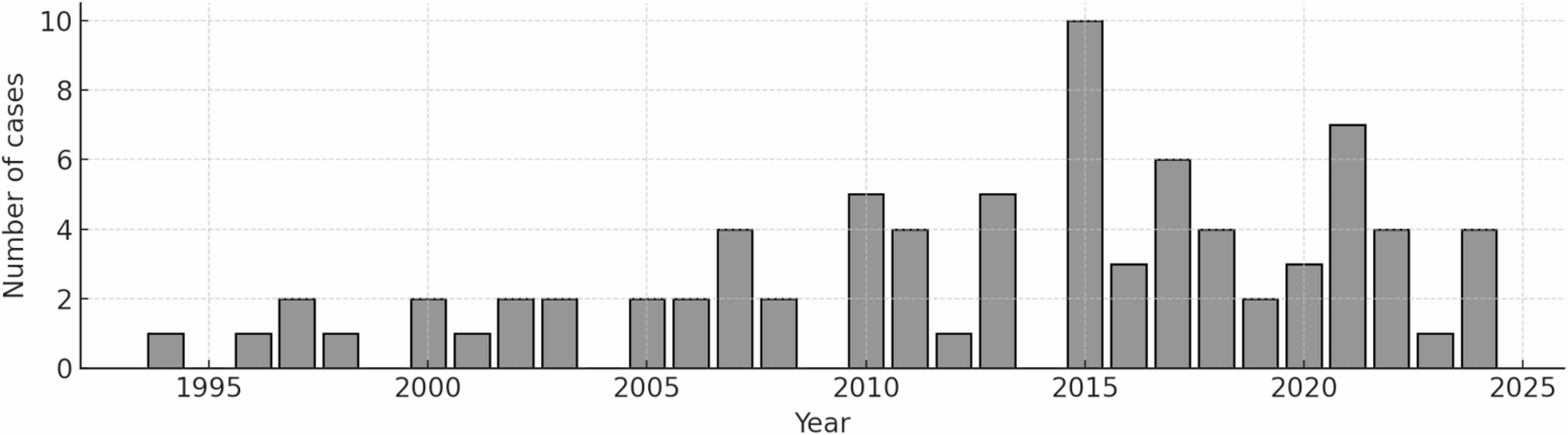
All KD diagnoses, were retrospectively re-evaluated to ensure consistency with the currently accepted clinical diagnostic criteria [1]. Although the core clinical features (≥ 5 days of fever plus ≥ 4 of the 5 principal clinical signs) have remained unchanged since the original description by Kawasaki [16], their application, particularly in incomplete presentations, has been progressively refined in successive AHA scientific statements [17]. This process ensured diagnostic homogeneity across the entire 30-year study period. Patients ≤ 18 years of age were eligible. Since 2020, patients meeting diagnostic criteria for Multisystem Inflammatory Syndrome in Children (MIS-C) or in whom a temporal association with SARS-CoV-2 infection was established, were excluded from the Kawasaki disease cohort and classified separately as MIS-C cases. A temporal representation of case distribution throughout the study period is provided (Fig. 1).
Fig. 1
Annual distribution of Kawasaki disease cases diagnosed in our cohort (1994–2024)
Baseline demographic, clinical, laboratory, and treatment characteristics were documented to contextualize the study population and to support the real-world applicability of the evaluated risk scores (Table 1).
Table 1 Baseline characteristics of Kawasaki disease patients (n = 81)The mean age at diagnosis was 40.9 ± 36.1 months; 10/81 patients (12.3%) were < 12 months old; and 44/81 (54.3%) were female. Most patients presented with complete KD (58/81; 72%), while 3/81 (3.7%) fulfilled criteria for KD shock syndrome. IVIG was administered in 76/81 patients (93.8%) and upfront combined IVIG plus corticosteroids in 17/81 (21%). Five patients did not receive IVIG due to spontaneous defervescence prior to treatment indication or late diagnosis without criteria for treatment at presentation. Among patients treated with IVIG, the median time from fever onset to initial infusion was 5 days (IQR 5–7). Most patients were of European ancestry (Spanish origin: 70/81–86,4%-), while the remaining children were South American (n = 6), Eastern European (n = 2), African (n = 2), Asian (n = 1), or Romani origin (n = 1).
Clinical and Laboratory DataDemographic, clinical, laboratory, treatment, and follow-up data were obtained from electronic medical records. Abnormal laboratory values were defined according to age-adjusted reference ranges used at our institution. Risk scores were only calculated when all required variables were available; no data were imputed.
Echocardiographic AssessmentTransthoracic echocardiography was performed by pediatric cardiologists according to AHA and American Society of Echocardiography standards [18]. Given the historical nature of the cohort (1994–2024), different Z-score reference systems were used over time depending on clinical availability. During the earlier years of the study period, coronary artery dimensions were interpreted using the reference tables from Boston Children’s Hospital [19]. In more recent years, the Dallaire and Dahdah equations [20] were adopted in routine clinical practice. Coronary artery involvement was categorized as dilatation (Z ≥ 2.0 to < 2.5), small aneurysm (Z ≥ 2.5 to < 5), medium aneurysm (Z ≥ 5 to < 10), and large/giant aneurysm (Z ≥ 10 or absolute diameter ≥ 8 mm), following AHA criteria [1, 15].
Coronary measurements were therefore interpreted according to the Z-score system in clinical use at the time of diagnosis, and uniform retrospective reclassification using a single contemporary reference system was not feasible.
IVIG Treatment ProtocolInitial treatment consisted of intravenous immunoglobulin (IVIG) administered at a dose of 2 g/kg as a single infusion over approximately 10–12 h, in accordance with contemporaneous American Heart Association recommendations [1, 15].
Despite the long study period, the core IVIG dosing strategy and timing of administration remained essentially unchanged, ensuring therapeutic consistency across decades. However, adjunctive treatment strategies evolved over time, particularly the increasing early use of corticosteroids in more recent years for patients considered at higher risk.
Patients who did not receive IVIG, mainly due to spontaneous defervescence prior to treatment indication or late diagnosis or late diagnosis without criteria for treatment at presentation were excluded from analyses evaluating IVIG-resistance risk scores.
From 2017 onwards, initiation of adjunctive corticosteroids was partly guided by baseline IVIG-resistance risk stratification, particularly the Kobayashi score and AEP high-risk criteria, reflecting real-world score-directed treatment escalation.
OutcomesThe primary outcomes were: (a) IVIG resistance, defined as persistent or recrudescent fever ≥ 36 h after completion of the initial IVIG infusion [1, 15]; (b) Coronary artery involvement, defined as any coronary dilation or aneurysm with a Z-score ≥ 2.0 in any major coronary segment during the acute or subacute phase [1, 15].
Risk Scores EvaluatedWe applied the following IVIG-resistance scores: Kobayashi [4], Egami [5], Sano [6], Kawanet [11], Kawanet-echo [12], Kawa-Race (IVIG resistance score) [13] and AEP consensus recommendations for therapeutic intensification [14]. For coronary risk prediction: Son score [10] and Kawa-Race (coronary involvement score) [13]. Each score was applied retrospectively using original published cut-off thresholds. Because IVIG resistance can only be defined in patients who actually received intravenous immunoglobulin, analyses of IVIG-resistance risk scores were restricted to patients treated with IVIG as initial therapy, consistent with original derivation and validation studies [4]. Because of the retrospective and historical nature of the cohort, some variables required for specific scores were not consistently available; therefore, the number of patients included in the analysis varied by score and is detailed in the Results and Tables.
Description of Risk ScoresThe Kobayashi score includes serum sodium ≤ 133 mmol/L, aspartate aminotransferase (AST) ≥ 100 IU/L, C-reactive protein (CRP) ≥ 10 mg/dL, neutrophils ≥ 80%, age ≤ 12 months, illness ≤ 4 days at initial treatment, and platelet count ≤ 300 × 10⁹/L, with a cutoff ≥ 4 indicating high risk of IVIG resistance [4].
The Egami score incorporates age ≤ 6 months, alanine aminotransferase (ALT) ≥ 80 IU/L, CRP ≥ 8 mg/dL, platelet count ≤ 300 × 10⁹/L, and illness ≤ 4 days at initial treatment, with a score ≥ 3 suggesting high risk [5].
The Sano score identifies high risk when at least two of the following are present: CRP ≥ 7 mg/dL, total bilirubin ≥ 0.9 mg/dL, and AST ≥ 200 IU/L [6].
The Kawanet score includes hepatomegaly, ALT ≥ 30 IU/L, lymphocyte count < 2400/mm³, and time to treatment < 5 days, assigning 1 point per variable with a cutoff ≥ 2 points indicating increased risk of of requiring second-line treatment after the first IVIG dose [11].
The Kawanet-echo modification combines the Kawanet score with an abnormal pre-treatment echocardiogram. (coronary artery Z-score ≥ 2.0, pericarditis, myocarditis, or reduced left ventricular systolic function) and predicts the need for second-line therapy after the first IVIG dose [12].
The Kawa-Race IVIG resistance score is a weighted multivariable model including male sex, age at admission < 3 months, fever duration ≥ 8 days, lymphadenopathy, cardiac involvement, serum creatinine ≥ 0.4 mg/dL, C-reactive protein ≥ 8.7 mg/dL, hemoglobin < 10 g/dL, and serum sodium < 134 mmol/L, with a cutoff ≥ 8 points indicating high risk of IVIG resistance [13].
The Spanish Pediatric Association (AEP) consensus was applied as a clinical severity framework to guide treatment escalation rather than as a numerical risk score [14]. Patients were classified as “high-risk” when early treatment intensification was indicated. High-risk criteria included the presence of at least one of the following prior to therapy: age < 12 months; marked elevation of inflammatory markers (CRP ≥ 90 mg/L, ESR ≥ 80 mm/h, or platelet count ≥ 900 × 10⁹/L); hepatic dysfunction (AST and/or ALT ≥ 2× the upper limit of normal and/or total bilirubin > 1 mg/dL); hypoalbuminemia (≤ 2.5 g/dL); hyponatremia (≤ 133 mmol/L); or a ≥ 2 g/dL decrease in hemoglobin relative to the age-specific lower limit. In these patients, treatment was intensified with IVIG combined with low-dose corticosteroids. “Severe KD” was defined by shock, coronary artery aneurysms, or other significant cardiac involvement (such as left ventricular systolic dysfunction or relevant pericardial effusion), or by age < 12 months combined with at least two of the high-risk laboratory criteria listed above; in these cases, upfront treatment with IVIG plus high-dose corticosteroid pulses was recommended [14].
For coronary outcomes, the Son coronary artery aneurysm risk score includes baseline left anterior descending or right coronary artery Z-score ≥ 2.0 (2 points), age < 6 months (1 point), Asian race (1 point), and CRP ≥ 13 mg/dL (1 point), classifying patients into low- (0–1), moderate- (2), and high-risk (3–5) groups [10].
The Kawa-Race coronary score is a weighted multivariable model including male sex, age at admission < 4 months, fever duration ≥ 10 days, lymphadenopathy, serum creatinine ≥ 0.3 mg/dL, C-reactive protein ≥ 13.6 mg/dL, hemoglobin < 10 g/dL, and serum sodium < 130 mmol/L, with a cutoff ≥ 8 points indicating high risk of coronary artery aneurysm development [13].
Laboratory values used for score calculations were the extreme values (highest or lowest, depending on the parameter) obtained before IVIG administration.
Statistical AnalysisCategorical variables were expressed as frequencies and percentages. Continuous variables were summarized as mean ± standard deviation (SD) or median and interquartile range (IQR), depending on distribution.
For each risk score, diagnostic performance metrics were calculated, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Exact 95% confidence intervals (CIs) were estimated using the Clopper–Pearson method. Given the small sample size and low number of outcome events, non-parametric bootstrap resampling was considered; however, exact binomial confidence intervals were preferred as a conservative and stable approach for rare-event diagnostic measures.
Because adjunctive corticosteroid therapy became increasingly used during the later years of the study period, an exploratory stratified analysis according to therapeutic era (pre-2017 vs. ≥ 2017) was performed to compare IVIG resistance, coronary outcomes, and score performance. When sample size allowed, descriptive comparisons were conducted between patients treated with IVIG alone and those receiving IVIG plus upfront corticosteroids. Because corticosteroid initiation in later years was partly guided by baseline IVIG-resistance risk stratification (particularly Kobayashi and AEP criteria), these stratified analyses were considered exploratory and potentially affected by confounding by indication.
Ethical ConsiderationsThe study was retrospective and based on anonymized clinical data obtained from electronic medical records. No direct patient contact occurred. The study protocol was approved by the Clinical Research Ethics Committee of Cantabria (CEIm code: 2024/114)., which also waived the requirement for informed consent due to the retrospective design and the use of anonymized historical data.
Comments (0)