This is the first study addressing HRV, BRS, and SC on the basis of multimodal high-frequency monitoring during NIC following DC due to MMI. Consistent with reported findings of other brain injuries, e.g. TBI, ischemic, and hemorrhagic stroke [10,11,12,13,14,15,16, 23,24,25,26, 28,29,30,31,32,33], we observed impaired ANS including reduced HRV and BRS, as well as disturbed signal complexities of HR, MAP, ICP, and AMP in patients with MMI during the first 7 days of NIC after DC. Overall, low SC of HR, MAP, ICP, and AMP did not correlate with demographics or stroke severity, but were significantly associated with a greater burden of insults of key cerebral NIC variables, and reduced tolerance of such autoregulatory disturbances. Low signal complexities of MAP, ICP, and AMP were also independently associated with worse functional outcome. Therefore, SC may contain information that might aid in indicating the occurrence of and tolerance for secondary cerebral insults, including ICP, CPP, and PRx, to fine-tune NIC beyond the traditional treatment targets. Additionally, SC may be a useful tool for outcome prognosis in patients with MMI following DC.
ANS appeared to be impaired following DC in this cohort, with median SDNN of 112 ms, RMSSD of 28.5 ms, and BRS of 3.6 ms/mm Hg, i.e., lower compared with healthy individuals in previous studies [21, 22, 46]. These findings are consistent with reduced HRV and BRS in other brain injuries, such as TBI [15, 16, 47], and general acute ischemic stroke cohorts [10, 48, 49]. SDNN describes overall HRV, affected by both sympathetic and vagal modulation, while RMSSD reflects BtB variability, mainly influenced by parasympathetic tone [19]. Thus, the decreased SDNN and RMSSD together likely reflect suppressed vagal tone and overall autonomic imbalance. Similarly, BRS describes the heart rate response to spontaneous fluctuations and insults in blood pressure through vagal baroreflex control of the sinoatrial node [50]. Thus, reduced BRS also indicates disturbed parasympathetic modulation of heart rate in relation to blood pressure. SC is rather different from HRV and BRS, since absolute values cannot be compared across variables and cohorts. However, as SC of HR, MAP, ICP, and AMP demonstrated significant correlations with cerebral variables and outcome, we assumed that SC reflected disturbed cerebral physiology in some of our patients, in accordance with other acute brain injury conditions, such as aSAH and TBI [23,24,25,26, 28,29,30,31,32,33].
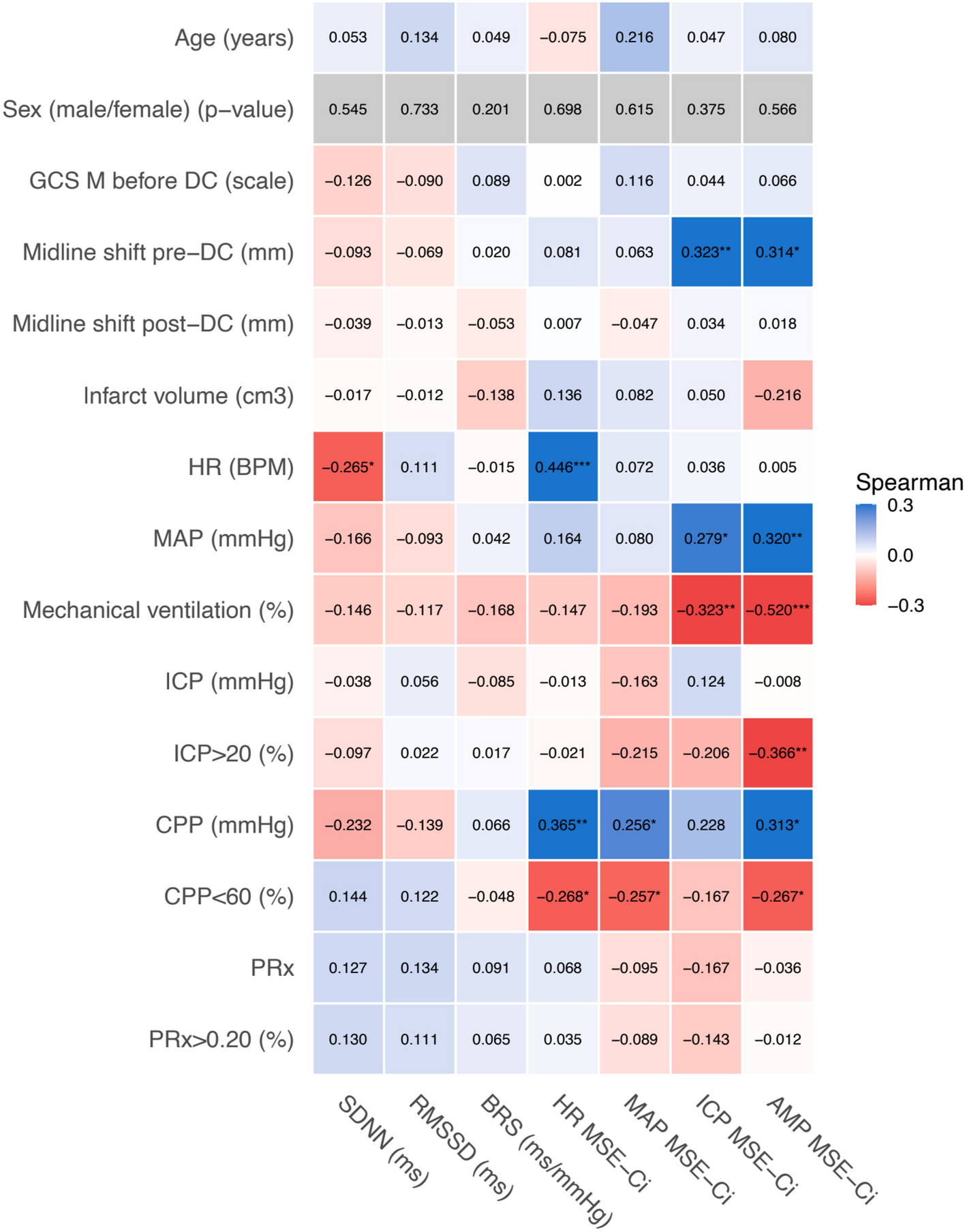
Multiple demographic and clinical factors may have affected autonomic function and SC in our cohort. Age and common comorbidities in patients with stroke, e.g., atherosclerosis, hypertension, heart failure, and coronary artery disease, are known to reduce HRV and BRS [21, 22, 46, 48, 49]. These factors may have partly contributed to disrupted ANS in this cohort with a median age of 57 years and typically heavy cardiovascular comorbidities. Interestingly, important markers of stroke severity, e.g., GCS M, midline shift, and infarct volume, did not correlate significantly with HRV, BRS, and SC either, except for higher midline shift pre-DC with higher SC of ICP and AMP. Still, the impaired ANS in patients with MMI, observed in this study, is likely partly caused by the widespread underlying brain injury caused by ischemia and space-occupying edema in important areas that control autonomic functions [10, 17]. Nevertheless, the lack of significant correlations between age and stroke severity vs. HRV, BRS, and SC can be explained by the homogeneity of the analyzed subgroup composed of older patients with MMI, which by definition is a severe and widespread hemispheric brain injury [1]. Although the pathophysiology cannot be fully elucidated, decreased HRV and BRS together may reflect sympathetic overdrive and vagal withdrawal due to central autonomic dysfunction caused by impaired insula or subsequent to injury to the brainstem in case of brain herniation [48, 50]. Additionally, mechanical ventilation and some medications administered in NIC, including sedatives, are known to decrease autonomic variability [18, 19, 44]. Most patients herein, particularly those with more severe underlying injuries or secondary brain injuries, spent the first 7 days of NIC time following DC sedated and mechanically ventilated. In other words, the sedatives together with the ventilatory support may have partly contributed to the suppressed HRV and BRS in our cohort, despite the lack of formal statistical association. Lower SC of ICP and AMP did correlate significantly with greater percentage of monitoring time in ventilatory support. However, it is difficult to specify whether the sedation and mechanical ventilation reduced intracranial SC or the reduced complexity impacted the chance of extubation.
In contrast to TBI and general ischemic stroke cohorts [10, 15, 16, 47,48,49], HRV and BRS were not associated with ICP, CPP, or PRx in our cohort. However, consistent with other acute brain injury conditions [23,24,25,26, 28,29,30], SC was significantly linked to key NIC variables in this study. For instance, higher SC of HR, MAP, and AMP correlated significantly with higher CPP and lower %VMT of CPP below 60 mm Hg. Likewise, AMP SC was significantly associated with lower %VMT of ICP above 20 mm Hg. The hypothetical mechanism is that lower SC may indicate reduced adaptive capacity to compensate for spontaneous fluctuations and pathological insults in autonomic regulation of heart rate and blood pressure through the baroreflex and autoregulatory modulation of cerebral blood flow and vascular tone [23,24,25,26, 28,29,30,31]. Hence, systemic and cerebral vascular responses to insults are less complex, and these rigid responses may therefore not fully compensate for pathological signal fluctuations [23,24,25,26, 28,29,30,31]. However, the causal direction of this association is rather difficult to define. On the one hand, low cerebral and systemic SC may not be able to properly compensate for the disrupted ANS with reduced BRS and HRV, leading to excessive fluctuations in blood pressure [51]. The result can, in turn, be impaired CPP and a heavier burden of cerebral insults, facilitating secondary brain injury and further development of edema [51]. On the other hand, physiological systems progressively lose their adaptive capacities when exceeding pathological thresholds [51], meaning that a certain burden of physiological insults may overload compensatory mechanisms, decreasing SC.
Furthermore, HRV and BRS did not correlate with outcome in our cohort, contrary to studies of general ischemic stroke and TBI [10, 15, 16, 47,48,49]. However, lower signal complexities of MAP, ICP (both p < 0.001), and AMP (p < 0.01) were significantly associated with worse outcome in multivariable ordinal logistic regression models adjusted for age (years), Glasgow Coma Scale motor score pre-DC (scale), infarct volume (cm3), and time proportion of the first 7 days of NIC spent on mechanical ventilation (%). These findings are consistent with TBI cohorts [23,24,25,26, 28,29,30,31,32,33], except for HR SC, which was not associated with outcome in our cohort. Additionally, low signal entropy of MAP, ICP, and AMP combined with high ICP, low CPP, and high PRx were particularly associated with poor outcome, possibly reflecting an exhaustion of adaptive physiological reserves to cope with such cerebral insults. This inability to compensate, especially during insults, could be linked to the loss of complexity and interdependent feedback loops [32]. Our findings suggest reduced SC to be a biomarker for pathological cerebral and systemic states, and thus associated with unfavorable outcome. Additionally, low SC may contribute to a greater burden of secondary insults of cerebral and systemic homeostasis and/or fail to compensate for such insults when they occur, possibly as low complexity reflects more rigid interactions between the cerebral and systemic vascular physiology. Thus, SC may potentially be a useful tool to aid in identifying patients more susceptible or less tolerant of secondary physiological insults as a means to fine-tune NIC post-DC and also in making outcome prognosis. However, confounders may have influenced our analyses. For instance, although systematic reviews report no difference between dominant and nondominant hemispheres in MMI outcome after DC [52, 53], patients with infarct lateralized to the right hemisphere demonstrated significantly better cerebral autoregulation (PRx) and 6-month mRS (p < 0.05) in this cohort. Therefore, our preliminary results require further exploration and prospective, multicenter validation before they can be implemented in clinical practice.





Comments (0)