
Remember me






We began by profiling peripheral blood mononuclear cells (PBMCs) from 22 patients with ALS and 18 healthy controls (HCs) using scRNA-seq (Fig. 1a). The ALS cohort comprised 18 patients with sALS and 4 with C9-ALS (Fig. 1a,b). To account for disease heterogeneity, patients with sALS were further stratified into slow-progressing (sALS-slow) and fast-progressing (sALS-fast) subgroups based on ALS Functional Rating Scale scores (Supplementary Table 1). Cohorts were well balanced for age and sex (Fig. 1c and Extended Data Fig. 1a). Because all patients with C9-ALS were female, comparisons involving the C9-ALS group were limited to female HCs to control for sex-specific immune differences.
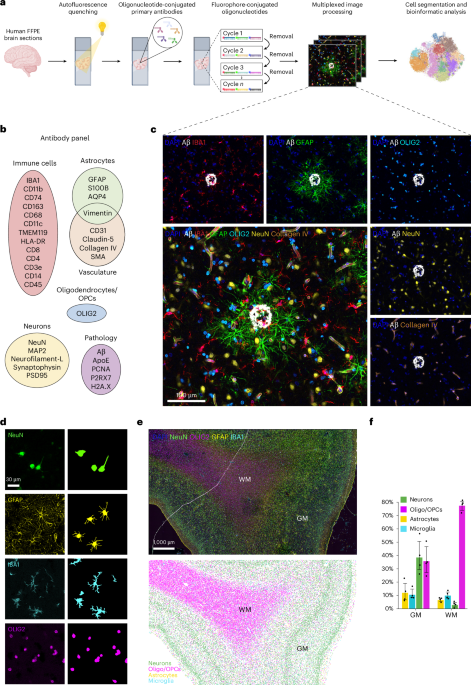
Fig. 1: Single-cell transcriptomic analysis of peripheral immune dysregulation in patients with ALS. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a, CRISPR-powered scRNA profiling was used to analyze PBMCs from patients with sALS and fALS with varying disease progression rates. b, Patient cohort distribution—n = 18 HC, n = 22 patients with ALS subdivided into fast sALS (sALS-fast, n = 9), slow sALS (sALS-slow, n = 9) and C9-ALS (n = 4); each sample represents PBMCs from one independent donor. c, Patient age distribution. d, UMAP showing 279,856 cells annotated into major immune subsets, integrated with Harmony. e, Bar plot showing the percentage of each cell type across cohorts. f, UpSet plot summarizing DEGs across all comparisons, highlighting both common and subtype-specific transcriptional changes. g, Heatmap of C9orf72 expression across diagnosis in cell types with at least 500 cells. h, Volcano plot comparing C9orf72 expression by differential expression in C9-ALS against female HCs across different cell types. P values were calculated using MAST and adjusted for multiple comparisons using the Benjamini–Hochberg method. i,j, Donut charts showing the distribution of cell types with >10% DEGs in ALS groups (i) and by sALS disease progression rate (j). NK, natural killer cells; MAIT, mucosal-associated invariant T cells; Mono, monocytes; HSPC, hematopoietic stem and progenitor cells; ASDC, AXL+ SIGLEC6+ dendritic cell; TCM, T central memory cell; γδ T, gamma delta T cell; ILC, innate lymphoid cell; pDC, plasmacytoid dendritic cell; dnT, double negative T cell. Schematic in panel a created in BioRender; Fontanna, T. https://biorender.com/a23j248 (2024).
To enhance the detection of biologically relevant transcripts, we used clustered regularly interspaced short palindromic repeats (CRISPR) technology for targeted transcript enrichment in our scRNA-seq libraries. This depletion method redirected sequencing reads from abundant mitochondrial and ribosomal molecules to lower-expressing, high-value transcripts in an unbiased manner. This approach led to a pronounced reduction in mitochondrial and ribosomal reads (Extended Data Fig. 1b,c). Notably, no significant differences were observed in unique molecular identifiers or gene counts, nor in mitochondrial or ribosomal gene content across samples, ensuring consistent data quality (Extended Data Fig. 1d–g).
Uniform manifold approximation and projection (UMAP) revealed distinct clusters of immune-cell types across ALS and HC cohorts (Fig. 1d and Extended Data Fig. 1h). However, analysis of cell-type distributions did not reveal significant changes to immune populations in patients with ALS compared to HCs (Fig. 1e and Extended Data Fig. 1i).
Differential expression analysis across all immune-cell types revealed the most unique transcriptional alterations in patients with C9-ALS, followed by fast-progressing sALS cases (Fig. 1f). Notably, C9orf72 transcript levels were reduced in PBMC subsets from individuals with C9orf72-associated ALS compared to HCs (Fig. 1g). Differential expression analysis revealed pronounced downregulation of C9orf72 in CD16+ monocytes, memory B cells and intermediate B cells (Fig. 1h). These findings indicate that C9orf72 haploinsufficiency affects multiple circulating immune-cell subsets in ALS.
To further investigate immune dysregulation in ALS, we then examined cell-type-specific transcriptional changes across the PBMC compartment. Innate immune cells, including monocytes and mucosal-associated invariant T cells, demonstrated the highest enrichment of differentially expressed genes (DEGs; Fig. 1i,j, Extended Data Fig. 1j and Source data Fig. 1i,j). CD16+ monocytes were more transcriptionally dysregulated in sALS, whereas CD14+ monocytes exhibited greater alterations in C9-ALS.
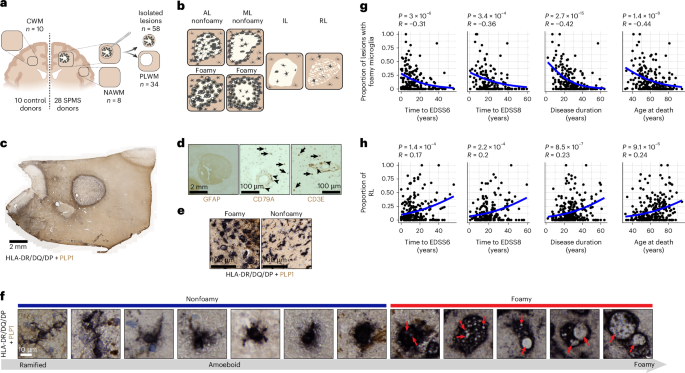
Differential expression analysis directly comparing C9-ALS and sALS, as well as fast versus slow progression within sALS, revealed that the majority of DEGs were concentrated in CD16+ and CD14+ monocytes (Fig. 2a). We therefore focused on CD16+ monocytes to identify genes associated with disease progression in sALS, and on CD14+ monocytes to investigate subtype-specific changes in C9-ALS. Within sALS, DEG analysis of CD16+ monocytes revealed significant upregulation of pro-inflammatory genes in fast progressors. Among these, key components of the innate immune complement system, including complement C1q A chain (C1QA) and complement C1q B chain (C1QB), were specifically elevated in the ALS-fast subgroup (Fig. 2b and Source data Fig. 2). A direct comparison of fast versus slow progressors within sALS confirmed increased expression of both genes (Fig. 2c). Additional genes associated with fast progression included MSR1, which encodes macrophage scavenger receptor 1, a pattern-recognition receptor involved in the uptake of modified lipoproteins, apoptotic cells and cellular debris9,10, and IFITM3, which encodes interferon-induced transmembrane protein 3, a downstream effector of type I interferon signaling known to modulate antiviral responses and amplify pro-inflammatory pathways11,12. Pseudobulk analysis further confirmed increased expression of C1QA and C1QB in sALS-fast (Fig. 2d and Extended Data Fig. 1k). These findings align with prior studies demonstrating increased concentrations of complement activation products in plasma13 and cerebrospinal fluid (CSF)14,15,16, as well as their deposition on innervated motor end plates in the intercostal muscle of patients with ALS17. Collectively, our results underscore complement activation in CD16+ monocytes as a key peripheral immune feature linked to sALS disease severity and progression.
Fig. 2: Single-cell transcriptomic analysis of dysregulation in innate immune cells of patients with ALS. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a, Bar plot summarizing the number of shared and unique DEGs between comparisons of different ALS subtypes across immune-cell types. b, log2(FC) plots for CD16+ monocytes (sALS-fast versus HC; sALS-slow versus HC). c, Volcano plot of DEGs between sALS-fast and sALS-slow in CD16+ monocytes. P values were calculated using MAST and adjusted for multiple comparisons using the Benjamini–Hochberg method. d, Per-donor pseudobulk normalized expression of C1QA and C1QB in CD16+ monocytes from HC (n = 18) and patients with sALS (n = 9 sALS-slow patients and n = 9 sALS-fast patients). Plots represent mean ± s.e.m. Outliers (>2 s.d. from the group mean) are shown as hollow points and were excluded from statistical testing. Two-sided Wilcoxon rank-sum test was used to compare groups. e, log2(FC) plots for CD14+ monocytes (sALS-fast versus HC; C9-ALS versus female HC). f, Volcano plot of DEGs between C9-ALS and sALS in CD14+ monocytes. P values were calculated using MAST and adjusted for multiple comparisons using the Benjamini–Hochberg method. g, GSEA of hallmark pathways comparing all patients with ALS against all HCs; only pathways enriched in at least two populations of innate immune cells are shown. Raw P values were computed by fgsea and adjusted for multiple testing using the Benjamini–Hochberg method.
Comparison of sALS and C9-ALS to HCs in CD14+ monocytes revealed distinct gene expression profiles that differentiate C9-ALS. Notably, the pattern-recognition receptor gene C-type lectin domain containing 7A (CLEC7A); the innate immune regulator tribbles pseudokinase 1 (TRIB1) and early growth response (EGR) genes EGR1 and EGR3 were specifically upregulated in C9-ALS (Fig. 2e and Source data Fig. 2). In contrast, genes uniquely upregulated in sALS included C-C motif chemokine ligand 3 (CCL3) and C-C motif chemokine ligand 3 like 1 (CCL3L1), highlighting subtype-specific inflammatory signatures (Fig. 2e and Source data Fig. 2). Direct comparison of CD14+ monocytes between C9-ALS and sALS further highlighted these subtype-specific programs. C9-ALS showed increased expression of IFITM2 and IFITM3, interferon-stimulated genes (ISGs) involved in antiviral defense and immune modulation18, whereas sALS showed elevated CCL3L1 and IL1B expression, key immunomodulators that mediate immune-cell recruitment19 and represent a downstream product of inflammasome activation, respectively20 (Fig. 2f). These findings demonstrate that unique innate immune activation pathways and transcriptional programs distinguish C9-ALS from sALS, suggesting distinct pathophysiological mechanisms underlying these ALS patient groups.
Gene set enrichment analysis (GSEA) of pathways shared by multiple innate immune cells revealed an increase in oxidative phosphorylation and a reduction in interferon-γ signaling in the combined ALS cohort (Fig. 2g). When focusing specifically on CD14+ monocytes, we observed significant enrichment of hallmark pathways related to reactive oxygen species production and hypoxia, which were increased only in sALS (Extended Data Fig. 1l). This suggests that the combined ALS signal may be primarily driven by the sALS subgroup. Tumor necrosis factor signaling through NF-κB was enriched in both patients with sALS and C9-ALS, while the inflammatory response signature in CD14+ monocytes was unique to C9-ALS (Extended Data Fig. 1l). Extending our analysis to adaptive immune cells, we identified pathways shared across multiple subsets (Extended Data Fig. 1m). Specifically, we found a downregulation of oxidative phosphorylation in CD4+ T cells and double-negative (dn) T cells, accompanied by an upregulation of tumor necrosis factor–NF-κB signaling and the p53 pathway across several adaptive immune-cell types. The contrasting effect of oxidative phosphorylation being higher in innate immune cells but lower in adaptive cells may reflect chronic innate activation compared to adaptive exhaustion. Notably, these findings prompted further examination of adaptive immune dysregulation in ALS.
To address this, we first examined DEGs in adaptive immune cells of C9-ALS and sALS compared to HCs. Notably, in each comparison, a high number of DEGs were identified in CD8 T effector memory (TEM) cells, a subset known to be antigen experienced (Extended Data Fig. 2a). To investigate further, we analyzed DEGs in clonally expanded T cell populations using our established T-cell-receptor-sequencing (TCR-seq) methods21,22,23. This analysis revealed numerous TCRβ chain genes that were uniquely dysregulated in C9-ALS or sALS compared to HCs, suggesting distinct CD8 TEM antigen-specific responses in each ALS subtype (Extended Data Fig. 2b). To assess clonal diversity, we analyzed TCR sequences from our scRNA-seq dataset. Clonotypes were defined as expanded if the same TCRβ CDR3 amino acid sequence was observed at least twice within an individual’s repertoire, a threshold commonly used to identify antigen-driven expansion24. While the number of expanded clonotypes did not differ significantly across groups, sALS-slow patients exhibited the highest proportion of unique clonotypes, suggestive of a more diverse, potentially polyclonal T cell response (Extended Data Fig. 2c). To investigate whether transcriptional changes observed in CD8+ TEM cells reflected underlying TCR gene usage biases, we compared differentially expressed TCR genes from the scRNA-seq dataset with V gene usage patterns from paired scTCR-seq data (Extended Data Fig. 2d). Notably, TRBV6-5, which was upregulated in sALS clonal CD8+ TEMs, showed the highest enrichment in sALS-fast patients, suggesting subtype-specific T cell activation.
Cumulatively, our findings reveal a striking alteration in immune-cell composition and activation states in patients with ALS, particularly among monocytes. The distinct inflammatory signatures observed in patients with sALS-fast and C9-ALS provide evidence for subtype-specific immune dysregulation. Furthermore, the identification of unique TCRβ chain gene expression patterns and a high number of DEGs in CD8 TEM cells underscores the potential involvement of antigen-specific T cell responses in ALS. These results highlight the role of peripheral immune activation in ALS pathophysiology and suggest potential therapeutic targets to modulate immune responses. To facilitate additional investigation, we have made these scRNA-seq data available as an interactive online resource at https://gatelabnu.shinyapps.io/als_app/.
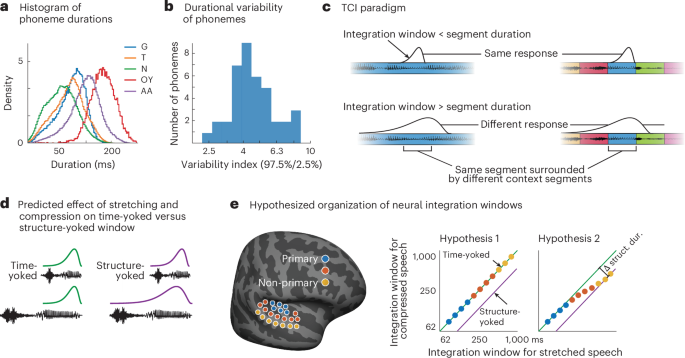
Gene expression changes and immune-cell dynamics in ALS CNS tissuesTo investigate inflammatory responses in patients with ALS within the CNS, we analyzed bulk RNA-seq datasets generated by the New York Genome Center (NYGC) ALS Consortium and Target ALS25 with a focus on immune signaling. We used a dataset of 1,464 postmortem samples derived from HCs (n = 92), ALS (n = 237), frontotemporal dementia (FTD; n = 50) and ALS/FTD (n = 26) patients, including tissues from the cerebellum, cortex (frontal, motor, occipital, temporal), hippocampus and spinal cord (cervical, thoracic, lumbar), collected from multiple clinical sites using standardized protocols (Fig. 3a, Extended Data Fig. 3a and Source data Fig. 3). We performed differential gene expression analysis between controls and ALS, ALS/FTD and FTD cases for each CNS tissue with at least three independent samples, while controlling for several variables (Methods; Fig. 3a and Extended Data Fig. 3b,c). In ALS cases, we observed the largest number of DEGs in the lumbar spine, motor cortex and cervical spine, respectively (Fig. 3a and Extended Data Fig. 3c). ALS/FTD samples displayed a similar pattern (Extended Data Fig. 3b,c), while FTD cases exhibited a substantially larger number of DEGs in the frontal cortex compared to ALS cases. This is consistent with the clinical presentation of these patients (Fig. 3a and Extended Data Fig. 3b,c). Intriguingly, the cerebellum, a region typically not thought to be involved in ALS/FTD26,27, exhibited a considerable number of DEGs (Extended Data Fig. 3c). To determine whether the DEG effect size was influenced by sample size, we used all ALS tissues and conducted serial downsampling. This analysis showed that, even in cases with as few as ten samples per tissue, spinal cord sections were the most affected CNS region in patients with ALS, as measured by DEG number (Extended Data Fig. 3d).
Fig. 3: Bulk RNA analysis of ALS CNS tissues reveals widespread changes in spinal cord cell types. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a, Schematic representation of different CNS regions examined, color coded based on the number of DEGs when comparing ALS or FTD postmortem samples to HCs from the Target-ALS/NYGC databases. b, Volcano plot of DEG analysis in the motor cortex of patients with ALS compared to HCs. c, Lollipop plot displaying the top 15 most enriched terms as determined by GSEA for cell-type markers, in the motor cortex of patients with ALS, compared to HCs. d, Volcano plot of DEG analysis in the cervical spine of patients with ALS compared to HCs. e, Lollipop plot displaying the top 15 most enriched terms as determined by GSEA for cell-type markers, in the cervical spine of patients with ALS, compared to HCs. f, Schematic representation of the cellular deconvolution method used to infer population changes in bulk RNA-seq datasets of CNS tissue based on scRNA-seq datasets30,31,32. g, Heatmap displaying inferred cell-type changes in ALS cortical tissues (frontal, motor, occipital, temporal cortices) based on the cellular deconvolution. h, Heatmap displaying cell-type changes in ALS spinal cord sections (lumbar, thoracic, cervical) based on the cellular deconvolution (top), and cell-type changes in ALS cervical spinal cord stratified by ALS-associated mutations (C9-ALS, sALS, SOD1-ALS; bottom). Statistical significance in g and h determined by Wilcoxon test; *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. MC, motor cortex; OC, occipital cortex; TC, temporal cortex; FC, frontal cortex; CB, cerebellum; CS, cervical spinal cord; TS, thoracic spinal cord; LS, lumbar spinal cord; OPC, oligodendrocyte precursor cell; SMC, smooth muscle cell; Prolif., proliferating.
We then focused on ALS cases, which had the largest sample size, to investigate the nature of gene expression changes. In the ALS motor cortex, some of the most significantly upregulated genes included MGAT4A, a Golgi-enriched glycosyltransferase enzyme; NAA50, an acetyltransferase-encoding gene; and the ferroptosis-associated ACSL4 gene (Fig. 3b). GSEA against cortical cell-type markers28 downloaded from the Molecular Signatures Database (MSigDB) revealed a strong upregulation of oligodendrocyte, microglia and inhibitory neuron signatures and a concordant downregulation of excitatory neurons and endothelial cells (Fig. 3c). In the ALS cervical spine, we observed upregulation of several immune-related genes including CHIT1, GPNMB, CD48, APOE, APOC1 and the complement genes C1QA, C1QB and C1QC (Fig. 3d). GSEA revealed a significant enrichment for microglia, brain immune cells, astrocytes and B cell and T cell signatures (Fig. 2e). In contrast, endothelial cells, excitatory neuron and oligodendrocyte terms were de-enriched (Fig. 3e). The upregulation of immune-cell expression signatures, particularly Microglia 3, was consistently found in both the motor cortex and cervical spinal cord of patients with ALS. To define the nature of this microglial subtype, we leveraged a recently reported annotation of human microglia transcriptional states29 and found an enrichment of genes related to lipid processing, ribosome biogenesis, phagocytic and inflammatory microglia states (Extended Data Fig. 3e). Intriguingly, although the cerebellum exhibited a very high number of DEGs, there was no significant enrichment for Microglia 3, while brain immune-cell signatures were de-enriched in this tissue except for cycling microglia 1 (Extended Data Fig. 3f).
To determine whether the DEGs within the bulk RNA-seq of multicellular tissue samples were influenced by differential cell proportions, we performed bioinformatic cell-type deconvolution (Fig. 3f). To ensure accurate cell-type identification, we used multiple single-nucleus RNA-seq datasets from the human frontal cortex30, motor cortex30 and spinal cord31,32 for tissue-specific cell deconvolution. We used a signature matrix generated from a frontal cortex single-cell dataset30 to deconvolute the corresponding frontal cortex bulk RNA-seq data, a motor cortex dataset30 to deconvolute motor cortex data and a combination of both regions to deconvolute the occipital and temporal cortex data (Extended Data Fig. 4a,b; Methods). Tissue-specific deconvolution is critical, as the inferred proportions of certain cell subtypes, such as inhibitory neurons, pericytes, T cells and oligodendrocyte precursor cells, are strongly affected by the source dataset (Extended Data Fig. 4c). Consistent with the GSEA analysis, we found a significant increase in inhibitory interneurons and a reduction in endothelial cells, in both the motor and the frontal cortex of patients with ALS (Fig. 3g). We also found an increase in the proportion of microglial cells specifically in the motor cortex, while other brain regions showed no substantial population changes, except for an increase in fibroblasts in the occipital cortex (Fig. 3g). More granular deconvolution of distinct neuronal subtypes revealed a complex interplay between excitatory and inhibitory neuron changes in the frontal and motor cortex of patients with ALS (Extended Data Fig. 4d,e). There were inferred increases in neurogliaform (SST-NPY-neg) and Rosehip (Rosehip-LAMP-PMEPA1) interneurons, as well as bidirectional changes in excitatory neurons (Extended Data Fig. 4e).
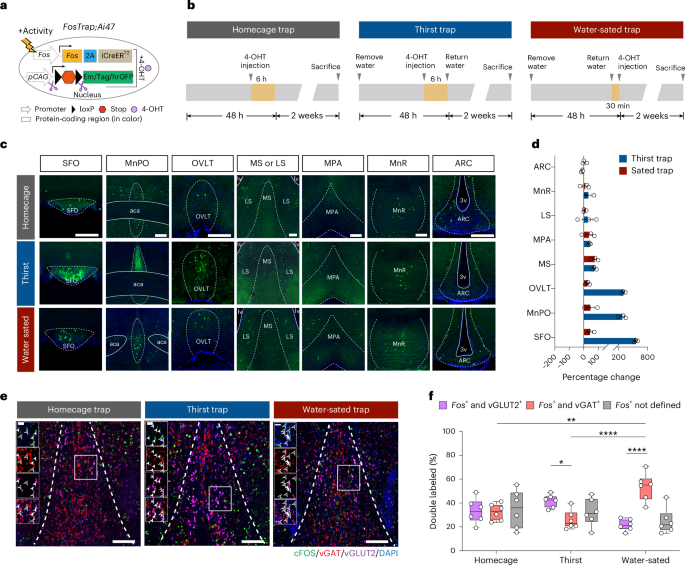
To deconvolute the bulk RNA-seq spinal cord data, we integrated single-nucleus RNA-seq data from a recently published spinal cord atlas32, with another spinal cord dataset generated using a neuronal enrichment strategy31 (Extended Data Fig. 5a–c; Methods). This analysis revealed significant proportional changes in several cell types. MNs and oligodendrocytes were reduced within the lumbar and cervical spinal cord sections of patients with ALS (Fig. 3h, top), while several types of immune cells, including macrophages, microglia and lymphocytes, were increased, along with astrocytes, Schwann cells and oligodendrocyte precursor cells (Fig. 3h, top). Notably, these changes were consistent across distinct ALS subtypes, including mutant C9-ALS, SOD1-ALS and sALS cases (Fig. 3h, bottom). To validate the shift from neurons to immune cells inferred by bioinformatic analysis, we performed immunohistochemistry (IHC) on cervical spinal cord sections from patients with ALS (n = 7) and HCs (n = 4–8). We observed a striking reduction in the number of large Microtubule-associated protein 2 (MAP2)+ neurons in the anterior horn of ALS cases (Extended Data Fig. 5d), along with a concomitant increase in the fraction of IBA1+ myeloid cells throughout the spinal cord (Fig. 4a,b and Extended Data Fig. 5e). Interestingly, these IBA1+ cells appeared larger and more morphologically complex (Fig. 4c and Extended Data Fig. 5f), suggesting an activated phenotype. Overall, the increase in the proportion of immune cells was more pronounced in the spinal cord compared to other CNS regions in patients with ALS (Fig. 4d).
Fig. 4: Innate immune cells are dysregulated in the ALS spinal cord and associated with disease duration. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.a, Digital representation of microglia cell distribution in the cervical spinal cord of patients with ALS and HCs. Each blue pixel corresponds to an IBA1+ cell, based on IHC staining. b, Bar plot quantifying the number of IBA1+ cells detected in a single cervical spinal cord section from patients with ALS and HCs. Plot represents mean ± s.e.m. Statistical significance determined by two-sided unpaired t test; P < 0.01. c, Superplot displaying the area of IBA1+ cells in the cervical spinal cord of patients with ALS and HCs. Small dots represent individual cells, large dots represent the mean value per patient and colors denote individual patients. Statistical significance determined by two-sided Welch’s t test; P < 0.01. d, Schematic representation of different CNS regions, color coded based on the number of changes in the proportion of immune cells (microglial cells, macrophages, lymphocytes) inferred from RNA-seq-based cellular deconvolution when comparing ALS samples to HCs. e, Scatterplot showing the correlation between changes in the proportion of immune cells (microglial cells, macrophages, lymphocytes) in the cervical spinal cord and disease duration in patients with ALS. Statistical significance determined by linear regression; shaded area represents the 95% confidence interval. f, Box plot showing inferred proportions of cell types in the cervical spinal cords of patients with ALS, split by short (n = 38) or long (n = 36) disease length. Box plots show median (centerline), IQR (box) and 1.5× IQR whiskers. Significance determined by Wilcoxon rank-sum exact test (*P < 0.05; astrocytes, P = 0.032; macrophages, P = 0.050; microglia, P = 0.033). g, Volcano plot ranking genes based on their expression correlation with disease duration in ALS patient cervical spinal cord. Blue dots represent negative and red dots represent positive correlation. Statistical significance determined by linear regression. h, Scatterplot showing the correlation among APOC1, CHIT1, LSP1, C1QA, C1QB and C1QC expression in the cervical spinal cord and disease duration in patients with ALS. Statistical significance determined by linear regression; CHIT1 (P = 2.76 × 10−10, r = −0.440, FDR = 6.48 × 10−6), APOC1 (P = 4.63 × 10−6, r = −0.327, FDR = 0.003), C1QA (P = 0.02, r = −0.164, FDR = 0.33), C1QB (P = 0.0022, r = −0.222, FDR = 0.09) and C1QC (P = 0.0009, r = −0.240, FDR = 0.055), LSP1 (P = 3.83 × 10−8, r = −0.388, FDR = 0.0003). i, Bar plot displaying the top ten most enriched terms from GSEA for cell-type markers (green) and Gene Ontology Biological Process terms (purple), based on genes showing the strongest negative correlation with disease duration in patients with ALS (blue dots in g). NES and corrected P value calculated by the fgsea implementation of the GSEA algorithm. IQR, interquartile range; NES, normalized enrichment score; mo, months.
Finally, we examined whether gene expression and cell-type changes correlated with ALS disease duration. In terms of cell-type changes, there was a negative correlation between the proportion of immune cells and disease duration (Fig. 4e), as well as the proportion of microglia (Extended Data Fig. 5g). There was no significant correlation between immune cells and age of disease onset (Extended Data Fig. 5h), nor was the same association with disease duration seen in other non-neuronal cell types (Extended Data Fig. 5i). To examine the association with disease progression in another way, we selected all 226 patients with ALS from the cohort with available disease duration data and partitioned them into fast and slow progressors. Specifically, patients in the top 25% and bottom 25% percentile in terms of disease duration (<22 or >48 months, respectively) were classified as fast progressing and slow progressing (Extended Data Fig. 5j). Using our original spinal cord deconvolution, we compared immune proportions between these groups. Notably, patients with a short disease course exhibited significantly higher proportions of macrophages and microglia in their spinal cords based on cell deconvolution analysis (Fig. 4f). Together, these results suggest that immune-cell changes appear to be more related to disease progression rather than the time of initial onset of ALS.
An unbiased analysis highlighted numerous myeloid genes negatively correlated with disease duration (Fig. 4g). These included CHIT1, which is substantially upregulated in ALS spinal cord33, as the top gene showing a strong negative correlation with disease duration in the ALS patient cohort (Fig. 4g,h and Source data Fig. 4g). leukocyte-specific protein 1 (LSP1) was the third top gene negatively associated with disease duration and is known to localize to nascent phagocytic cups during Fcγ receptor-mediated phagocytosis34. Consistent with a role in phagocytic activation, we found that LSP1+/IBA1+ microglia were increased in both the gray and white matter regions of the ALS spinal cord by IHC analysis (Extended Data Fig. 5k,l). Additionally, APOC1, implicated in macrophage activation through its role in lipid metabolism and inflammation, and the complement genes C1QA, C1QB and C1QC, which we also found to be upregulated in peripheral blood of patients with ALS (Fig. 2b–d), all showed a negative correlation with disease duration (Fig. 4h). To investigate whether the genes with the strongest negative correlation to disease duration were enriched for a particular pathway, we performed GSEA, which revealed microglia-enriched and immune-related categories as strong negative predictors of disease duration (Fig. 4i). These findings highlight profound cell-type shifts and immune activation in the ALS spinal cord, with reductions in neurons and oligodendrocytes accompanied by increased immune-cell populations, including activated myeloid cells, and suggest that upregulation of CHIT1, LSP1, APOC1 and microglia cells may serve as molecular markers linked to disease progression.
Regional specificity of inflammatory changes in ALS spinal cordTo further investigate the molecular mechanisms underlying spinal cord inflammation in ALS, we used SP to concurrently assess RNA and protein expression in spinal cord sections from nine HC, five sALS and four C9-ALS cases (Fig. 5a and Supplementary Table 1). Our approach included a panel of 31 barcoded immune antibodies, which were codelivered to tissue slides along with RNA probes. This enabled a spatially resolved analysis of both immune-cell populations and gene expression profiles within the tissue (Methods). Each SP spot was annotated based on our tissue staining (Methods) to correspond to one of four regions—anterior/lateral white matter, posterior white matter, anterior or posterior horns (Fig. 5b). Differential gene expression analysis between ALS and HC spinal cords was conducted for each region, identifying DEGs in the anterior/lateral white matter and anterior horns (Fig. 5c). Consistent with findings in peripheral monocytes of ALS-fast patients (Fig. 2a), we noted upregulation of complement genes C1QA and C1QB, as well as C1QC in the anterior/lateral white matter of ALS spinal cords compared to HC tissues (Fig. 5d and Source data Fig. 5d). Consistent with the bulk RNA-seq analysis (Fig. 3d), APOC1 emerged as a shared DEG across both the anterior/lateral white matter and anterior horns (Fig. 5d). Additionally, in the anterior horn where MNs reside, we
Comments (0)