Our main aim for undertaking this work was to substantiate our impression that SOTs were on the increase. We were particularly interested in substantiating this because of the previous proposal we and others had made for the transparency of the ICs [4,5,6,7,8]. Since SOTs mainly aim to quantitate harm through empirical research, we reasoned that if we could substantiate the increase in SOTs, our proposal for the transparency of the ICs would strengthen.
Our review did not support our impression that the SOTs were on the increase . On the other hand, some features of RCTs in general and that of SOTs in particular we reviewed, we believe, further strengthened our plea for the transparency of the ICs.
Namely:
I.
More RCTs were being conducted in critical care settings where there are not infrequent issues in obtaining ICs [12].
II.
POMs like death, stroke, or myocardial infarction were common POMs among the SOTs of the later years. We are not aware of formal studies about the frequency of these particular POMs in SOTs nor how they have been or should have been related to a potential trial participant in plain words in the related ICs.
III.
A pragmatic study design, almost solely present among the later RCTs in our review, also potentially has ethical issues related to its ICs [13] as we will further discuss under a separate subheading.
It is important to note that our plea for the transparency of ICs only referred to the written ICs. In this line, it is important to note that the portion of such written ICs increased from 85% among the earlier to 96% among the latter group of trials (Table 1). This strengthens our assumption that once ICs are in the public domain, the frequency of the very risky POMs like death, stroke, and myocardial infarction will substantially lessen.
An important methodological issue was that the final decision was ours whether an RCT had the main aim of efficacy or safety. In many instances, these aims were in line with the POMs stated by the RCT authors. However, in some instances, an RCT might declare its POMs both as an E plus a S trial, or vice versa where the RCT authors use the stated order of POMs to prioritize their main aim. Also, the indicated main aim of an RCT might not be the same as what the reader might consider as the main aim after carefully going over the same RCT [14]. In our review where the RCT authors declared a dual aim, it was solely our judgment what the overriding aim was regardless of what the authors stated. We felt this was justified since our main concern was to identify SOTs where potential harms to the study patients were perhaps not adequately explained to the study participants during the IC procedure.
Ethical considerations
It seems the older consideration that the harm of a medical intervention, either in the official post-approval state or otherwise in routine clinical use, like many older medical remedies are, is best assessed by observational data [1] is currently being seriously challenged by SOTs. It is important to remember that the Nuremberg Code explicitly states that “No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects” [15]. We do not find such strong discouragement against SOTs in the ensuing Helsinki Declarations. These are eleven in number starting in 1964 and ending in 2022. However, starting with the 2000 version, in the last five versions of the Helsinki Declaration the following statement appears: “Physicians may not be involved in a research study involving human subjects unless they are confident that the risks have been adequately assessed and can be satisfactorily managed.” [16]. The exact wording here discouraging SOTs might not be as strong as that in the Nuremberg Code. Nevertheless, to reconcile a POM of death, being present in almost a half of the latter period SOTs we reviewed, with the quoted paragraph from the Helsinki Code is clearly difficult. Here we also draw attention to the fact that the same paragraph aimed at research in general and not necessarily to SOTs, almost as a rule related to officially approved medical remedies.
We like to emphasize that a meaningful majority of efficacy trials are currently conducted in critical care facilities (Table 2) where as we described the issue of IC is more involved. This is why we want to reiterate that ICs should better be transparent for all types of RCTs.
A related and a historically important document is the report of an expert committee of the National Academy of Sciences on the ethical issues in studying the safety of approved drugs. This report was prepared upon a request from the FDA specifically for post-approval RCTs of safety. The report initially appeared in a letter form [2] and later as a book. These documents point out that an SOT is only justified when observational studies have not provided or cannot adequately provide an answer to the existence and the importance of a newly observed/suspected treatment harm from an already approved medical product. The report also emphasizes that the related informed consent in an SOT is expected to be substantially different from an ordinary efficacy trial. Those safeguards should include “…. the determination by an appropriately constituted review committee that the additional risk is small enough for it to be ethical to ask people whether they are willing to accept it solely [sic] to contribute to the public good.” [2]. Personal vs. public gain is perhaps at the core of the ethics of IC process related to an RCT [17]. This concern in planning an SOT has also been an important drive behind our conducting this narrative review.
Furthermore, some contemporary authorities posit that SOTs are never justified. “Although the outcome of a trial is uncertain, the primary response variable should always be one where either benefit or noninferiority is achievable” [3].
In brief, we appreciate that great care is indeed currently taken to prepare the ICs by expert institutional review boards under the scrutiny of drug licensing authorities with due concern for and respect to the patient autonomy. However, these considerations do not deter us from wanting to know how exactly POMs like probable death, myocardial infarction, or a stroke are conveyed, in plain language, to a potential study participant during the consent procedure.
Pragmatic trials
Recently, a case for pragmatic trials has been made that they are more easily conducted in a real life setting and among greater number of patients and for longer time periods [18]. Our findings do support (Table 4) that the trial durations and the numbers of participants are indeed higher in trials described as pragmatic by their authors. Interestingly, as we gratifyingly note, the trial durations get notably shorter in SOTs with a pragmatic design (Table 4) giving less time for potential harm.
The reason we focused on the pragmatic trials as a separate group in this review was the fact that there are well recognized potential ethical issues with pragmatic trials, particularly related to what constitutes an actual minimal risk to a trial participant, in the consent procedure of such trials [18]. As we point out in Table 3, there were five pragmatic trials among the SOTs. Among these five trials, three had death and one cerebral bleeding as a POM. Admittedly the numbers at hand are yet small while we are concerned that such pragmatic trials with such POMs will get more frequent in time.
Study limitations
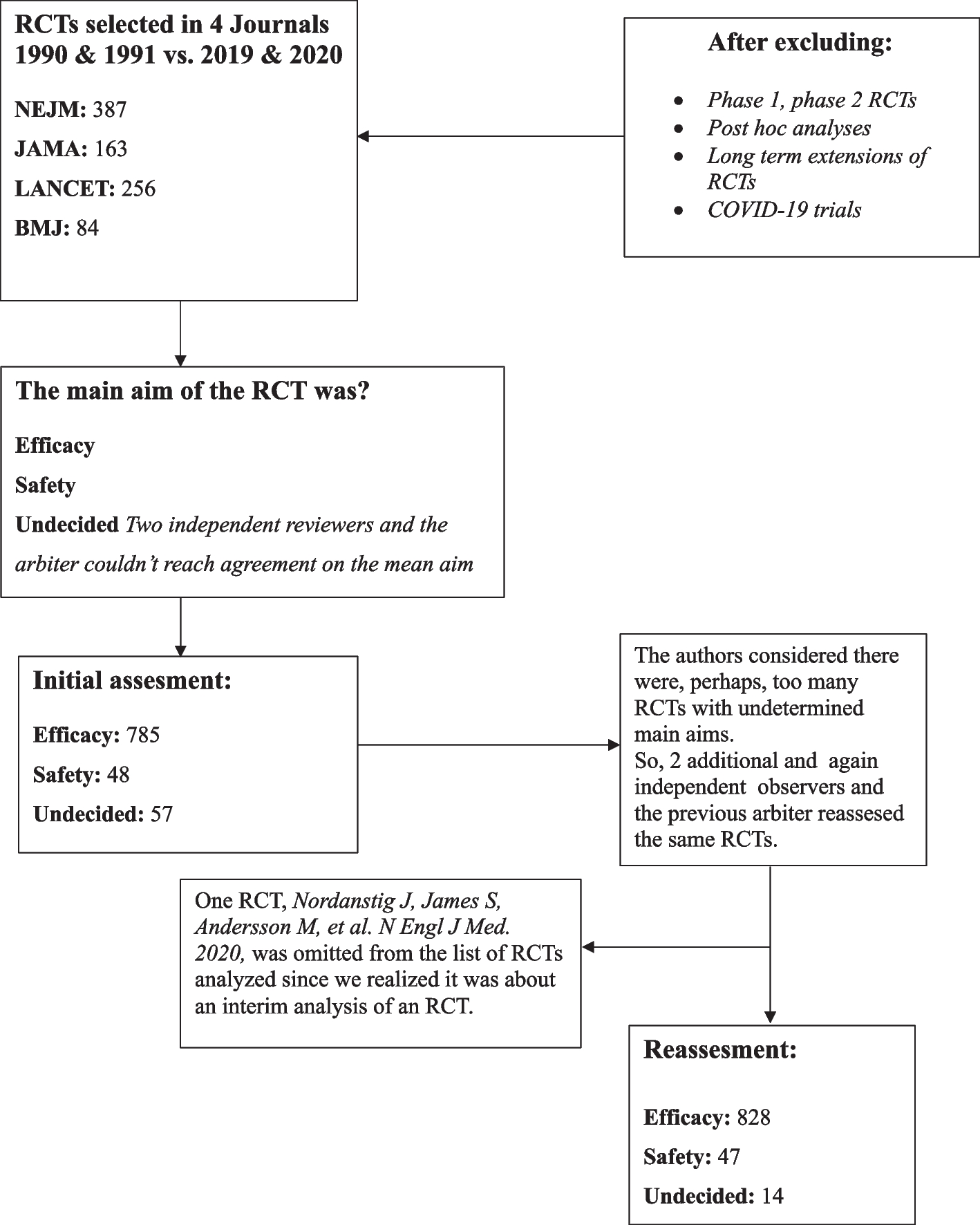
We consider our study to have two potential limitations. Paramount was accurately classifying the RCTs we reviewed as efficacy or safety trials. This was mainly the reason we recruited two additional colleagues into our review as we summarized in the methodology section. As is shown in Fig. 1 and can be seen in detail in Supplementary materials 2, 3, and 4, the main result of utilizing two additional observers was a significant decrease in the number of U trials the majority of which were reclassified under the E group (Supplementary material 5). We reason this notable decrease in the U trials in the second assessment the result of the observers not being bound by the generalization that the presence of potential serious harm to patients in any one arm of the study also qualified an RCT as an SOT in the reassessment.
It is interesting to note while we call the difficulty to tell an SOT from an efficacy trial as a limitation of our work, on further consideration, this very limitation can be viewed as supporting our call for transparency. Our observers and our arbiter are academics particularly interested and versed in RCTs. The consideration that even with this background we experienced serious difficulties in classifying a portion of completed RCTs published in our high impact medical journals as whether testing efficacy or safety, makes us feel more justified in our wanting to know how the main aims of these trials were conveyed to potential trial participants in plain language. We envisage that our not formally tabulating the POMs among the E and the U groups may also be considered as a potential limitation. On the other hand, our not tabulating death, stroke, or myocardial infarction as POMs among the E and U group of trials would, we reason, might even be a bias in the right direction in that this would only strengthen or plea to know how these particular POMs were, again, vocalized to the trial subjects.
The second potential limitation of our survey was in identifying the pragmatic trials. The pinpointing of an RCT as pragmatic can indeed be difficult. It has been said that the distinction between an explanatory, be it efficacy or safety, and a pragmatic trial can indeed be difficult and according to one scheme can range from a very explanatory to very pragmatic [19]. For this reason, we chose to use the authors’ naming their own trials as pragmatic, in our tabulations.


Comments (0)