
Remember me

HIV is a treatable long-term health condition, with a normal life expectancy among people on suppressive antiretroviral therapy (ART) with high blood T cell CD4 counts [1]. Around 100,000 people (100,063) were receiving HIV care in 2023 across England, Wales and Scotland [2]. Despite remarkable advancements in the prognosis of HIV over the past three decades, improvements in the mental health of people with HIV are less apparent, with the burden of mental health conditions among people with HIV being greater than the general population [3,4,5]. For example, the prevalence of anxiety and depression among people living with HIV in the UK is about twice as high as the background population [5, 6]. Wider socioeconomic factors also impact people living with HIV in the UK including poverty, unemployment, lack of social support and intimate partner violence [7,8,9]. Smoking, alcohol and drug use may also influence the physical and mental health of people with HIV [10,11,12]. People with HIV often experience intersecting vulnerabilities including societal stigma, structural inequalities and co-morbidities which impact mental health and well-being [3].
Mental health and HIV appear to have a bi-directional relationship; poor mental health may increase risk of acquiring HIV and HIV may result in poor mental health [3, 13]. A HIV diagnosis may result in anxiety and fears for the future and may also affect interpersonal relationships, impacting mental health and well-being. A further negative impact on health and well-being for people with HIV are experiences of socioeconomic disadvantage and lack of social support, factors that have extremely strong associations with poor mental health and reduced quality of life [5, 6]. In addition, people with HIV experience different forms of stigma including perceived, internalised and intersectional, with stigma found to be associated with depressive symptoms, social exclusion and lower levels of social support [14, 15]. People with HIV may also experience enacted stigma, discrimination or marginalisation due to factors including sexual orientation, gender and ethnicity [14,15,16,17,18].
National guidelines [19] for virologically suppressed people living with HIV (approximately 86,178 of 88,116 people [20]) recommend six monthly HIV viral load checks and annual follow-up with specialist HIV services. However, the majority access HIV specialist services more frequently than that, with a mean of 6.4 clinic appointments every year in virologically suppressed people attending one London HIV clinic between 2010 and 2017 [21]. This may be partly due to the high levels of trust people with HIV have in HIV services and difficulties accessing primary care services. Primary care satisfaction and trust may also be lower due to concerns including perceived stigma, issues around confidentiality and a perceived lack of HIV expertise [22, 23]. There is increasing awareness that to reduce use of secondary care to recommended guideline levels [19] by people with stable and controlled HIV, wider psychosocial needs must be addressed. The current usual model of HIV care does not address needs such as stigma, social support or socioeconomic disadvantage.
The National Health Service (NHS) Long Term Plan aims to implement personalised care across England to improve the outcomes for people with long-term health conditions such as HIV [24]. This would shift healthcare towards a model of a “shared responsibility for health” [25]. There are six key components of the NHS Comprehensive model of Personalised Care: (1) shared decision making; (2) supported self-management; (3) personalised care and support planning; (4) social prescribing; (5) patient choice; (6) personal health budgets, “social prescribing and community-based support” and “supported self-management” [24, 26]. Health coaching is a key component of supported self-management, focusing on empowering people to play a more active role in their health by developing knowledge, skills and confidence and by engaging in goal setting to reach solutions [27, 28]. A health coach may also link individuals to existing sources of support or voluntary sector organisations (social prescribing) such as smoking cessation services and mental health support [29]. However, evidence on the effectiveness of health coaching interventions remains mixed with higher-quality evaluations needed and there are few studies evaluating the effectiveness of health coaching in people living with HIV [30, 31].
RationaleWe propose an alternative model of care for people living with HIV, developed and evaluated through the “A person-centered Needs Informed model for Care for people with HIV” (NICHE) research programme. NICHE aims to improve the mental health and well-being of people living with HIV through a health and well-being coaching with social prescribing intervention delivered within specialist HIV services. The intervention aims to address and alleviate needs related to mental health problems, lack of social support, socioeconomic disadvantage and stigma. The health and well-being coaching will be delivered by HIV healthcare professionals who have undergone specialist training in coaching and social prescribing. This intervention will be evaluated in the randomised controlled trial (RCT) “Psycho-Social Intervention for People with HIV – Evidence from a Randomised Evaluation (SPHERE)” trial. HIV clinic populations will be screened to identify those individuals with psychosocial need. Consenting individuals will be randomised to either a one-to-one health and well-being coaching with social prescribing intervention or usual care. Our definition of psychosocial needs is broad and includes mental and physical health and well-being and social support. A psychosocial intervention addressing such needs could also have positive impacts on the delivery of HIV care in the UK as it may be cost-effective or cost-neutral for NHS services.
The trial research questions are:
(1)Does a health and well-being coaching and social prescribing intervention lead to an improvement in health and well-being among people with HIV who have psychosocial needs?
(2)How does the intervention achieve its outcomes?
(3)Is the intervention cost-effective?
Trial objectivesPrimary objectiveTo assess whether a psychosocial health and well-being coaching with social prescribing intervention improves participant-reported health and well-being for people with HIV who have physical, psychological, social or socioeconomic needs.
Secondary objectives (1)To assess the impact and mechanisms of action of the intervention on depressive symptoms, anxiety symptoms, health-related quality of life, stigma, social support, coping self-efficacy, resilience, lifestyle factors and NHS resource use.
(2)To assess the cost effectiveness of the intervention.
(3)To assess the acceptability of, uptake of, and long-term engagement with the intervention.
Internal RCT pilot objectives (1)To assess the feasibility of identifying eligible patients.
(2)To assess the acceptability of randomisation to receive the intervention or not.
(3)To determine if the pilot phase should continue to a full trial.
Observational cohort objectives (1)To investigate the feasibility of clinic-wide assessment of psychosocial needs.
(2)To assess the changes in psychosocial needs in people living with HIV in those who do not initially meet the screening criteria for trial entry.
(3)To identify factors associated with subsequent development of psychosocial needs.
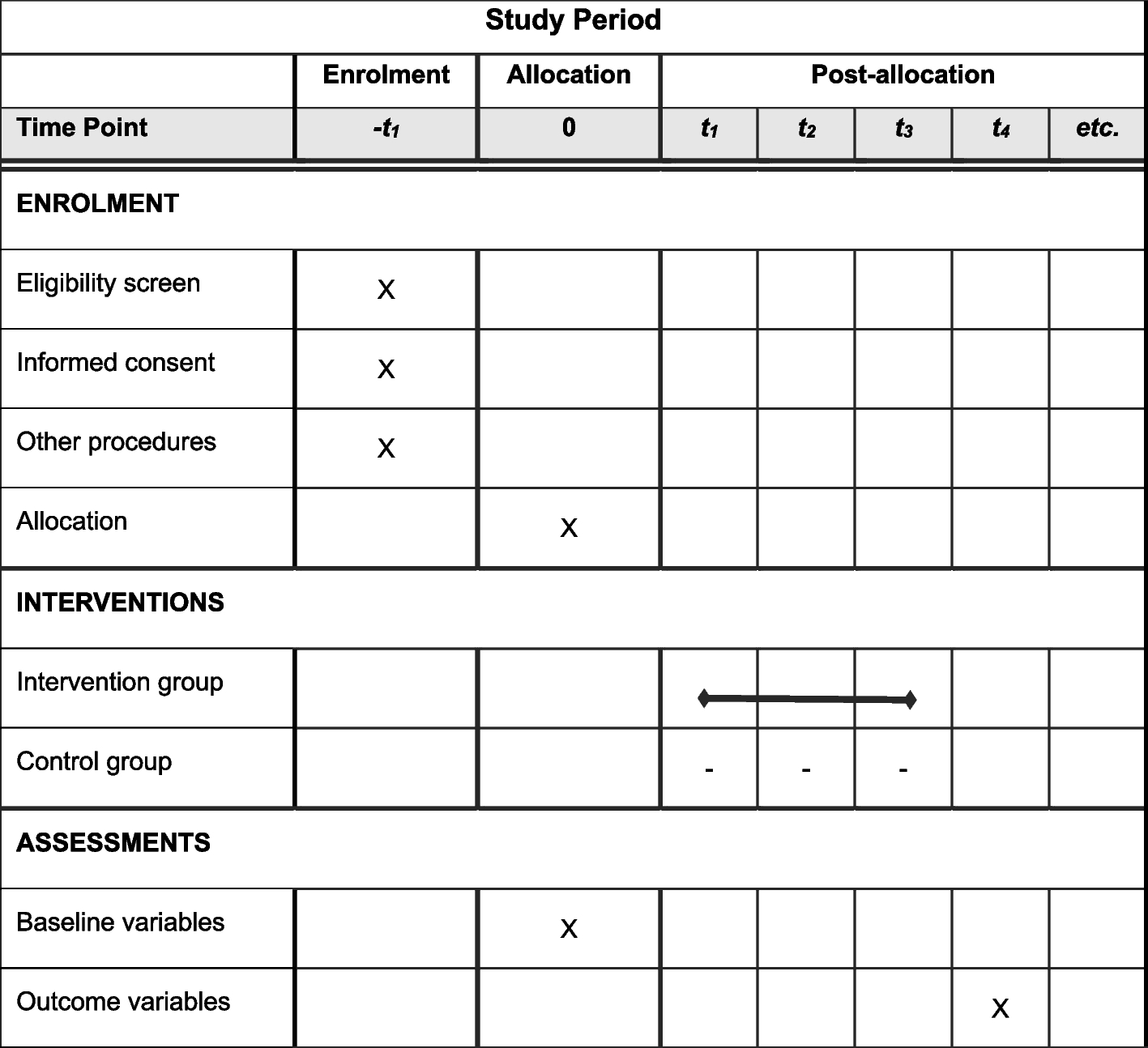
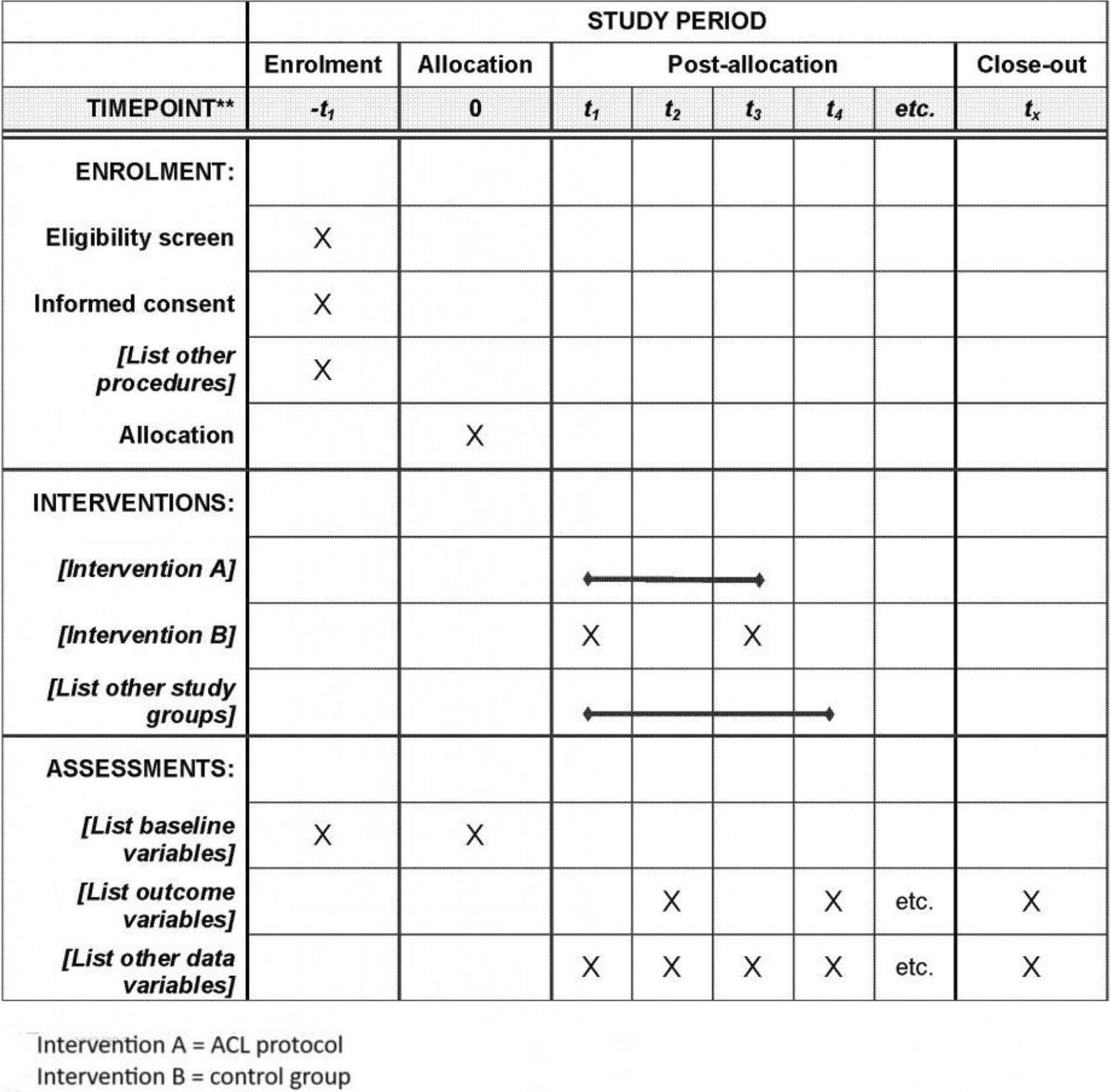
Trial methodsOur protocol adheres to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) [32] checklist (see Additional File 1).
Study designSPHERE is a national, pragmatic, multi-centre, individually randomised, two-arm, parallel group, superiority RCT that will use a routine assessment of psychosocial need in HIV care to identify those eligible for a health and well-being coaching and social prescribing intervention. The intervention will be delivered by HIV healthcare professionals who have received accredited training in coaching and social prescribing. Participants will be 1:1 randomised to receive the intervention or usual care. The trial will include an internal pilot phase (with stop/go criteria), process evaluation and economic evaluation (within-trial cost-effectiveness analysis), as well as a parallel observational cohort study among those not eligible for the intervention.
A shortened version of the Positive Outcomes tool [33] (“Positive Outcomes-11”) will be used to assess eligibility. This consists of eleven questions (each with response options 0 to 4, coded such that higher score indicates poorer health and well-being) covering physical health and well-being (pain; stomach or bowel problems; memory or concentration problems; sleep problems; ability to carry out usual activities), emotional/mental health and well-being (feeling anxious or worried; feeling depressed or in low mood; feeling good about yourself; feeling at peace), and social/socioeconomic well-being (having enough support from people around you; being worried about money), in the past 4 weeks. Those scoring above a threshold (16 or more out of a possible maximum score of 44) are eligible to be considered for randomisation.
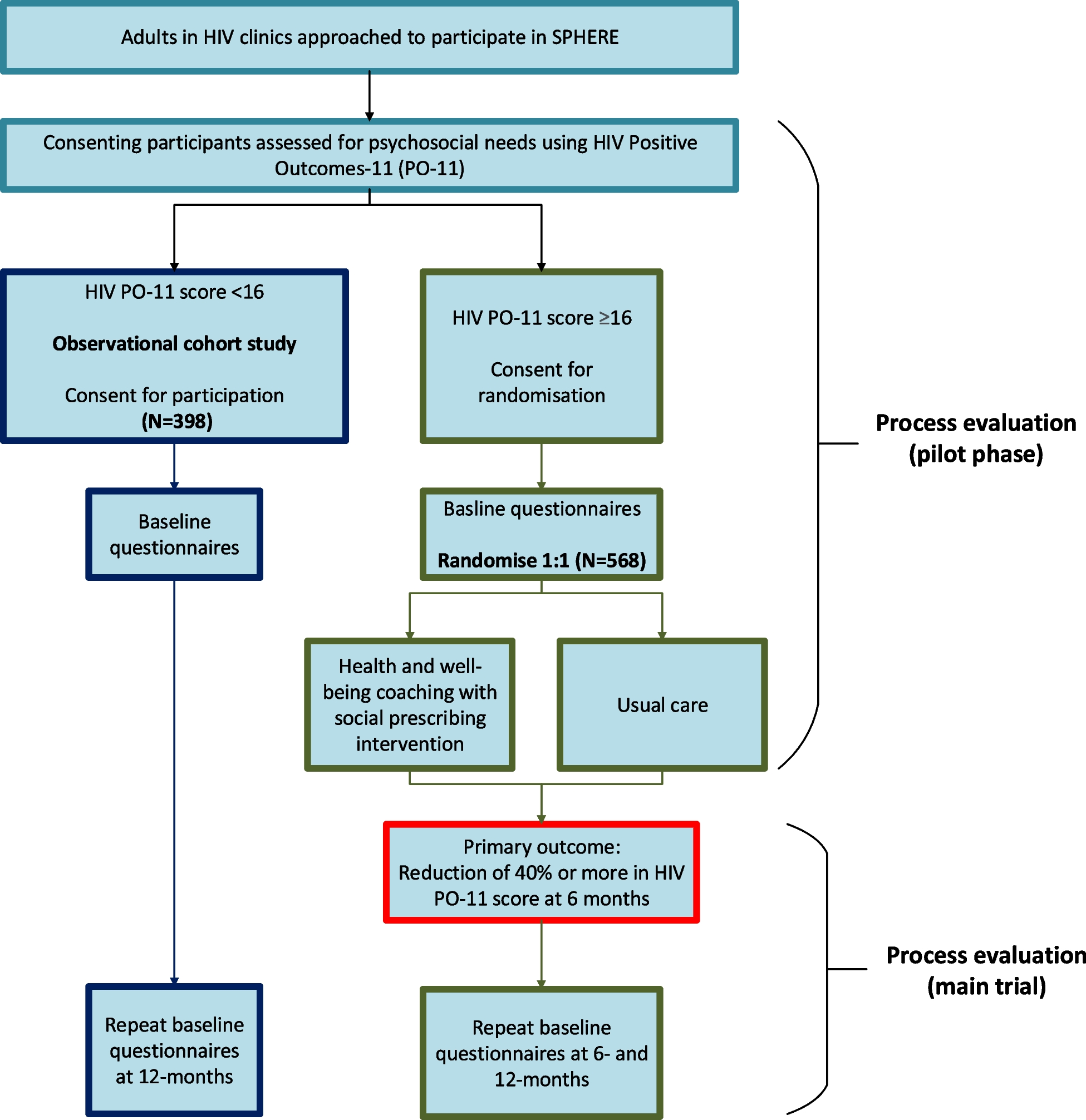
People with HIV who are eligible and consent to participate will be randomised at the level of the individual in a 1:1 ratio to either a health and well-being coaching with social prescribing intervention or usual care (Fig. 1). Participants will be followed-up for 12 months, with the primary outcome assessed at 6 months.
Fig. 1
SPHERE trial schema. Green boxes indicate RCT arm; dark blue indicates observational cohort
The intervention was informed by a mixed-methods programme of original research, namely a systematic review [31], qualitative research (focus group discussions and key informant interviews) [34], a national survey or people living with HIV [7] and a discrete choice experiment [35]. The programme theory was developed in Theory of Change workshops with 39 stakeholders including people with HIV, doctors, nurses, psychologists, third sector representatives (e.g. health coaching and social prescribing practitioners), commissioners and academics (manuscript in development).
There is a paucity of longitudinal data on changing symptoms and needs among people with HIV. Therefore, those who are not eligible for the trial (i.e. those with a PO-11 score < 16) will be invited to join a longitudinal observational study that will run in parallel with the RCT. This will investigate changes in well-being in this population to inform frequency of routine psychosocial assessment, with a view to implementing it as part of a new model of care for people living with HIV.
Primary and secondary outcomesThe primary outcome is health and well-being at month 6, measured using a binary outcome in which success is defined as a reduction of 40% or more in the Positive Outcomes-11 (PO-11) score [33] from baseline to month 6. PO-11 is comprised of 11 questions on health and well-being, each with a 5-point Likert scale response (scored 0 to 4). The total score ranges from 0 to 44 with a higher score indicating poorer health and well-being. Initial feasibility work for SPHERE has shown PO-11 to be a statistically valid tool that is effective in identifying people with poor mental health and well-being [33].
Secondary outcomes (all measured post-randomisation)Clinical (1)Health and well-being at month 12, measured using a binary variable in which success if defined as a 40% or greater reduction from baseline in the PO-11 score [33].
(2)Health and well-being at month 6 and month 12, measured using the PO-11 total score as a continuous measure (range 0 to 44). [33].
(3)Health and well-being at month 6 and month 12 measured using the PO-20 total score as a continuous measure (range 0 to 80). PO-20 is a longer form of the Positive Outcomes questionnaire [36] from which the PO-11 was derived [33]. It is comprised of 20 questions covering health and well-being and concerns in the past 4 weeks, each question with a 5-point Likert scale response (0 to 4, with a higher score indicating poorer health and well-being).
(4)Depressive symptoms at month 6 and month 12 measured using the total score of the Patient Health Questionnaire (PHQ-9) [37]. PHQ-9 is comprised of nine questions covering depression symptoms in the past 2 weeks each with a 4-point Likert scale response (0 = not at all to 3 = nearly every day). The total score ranges from 0 to 27 with a higher score indicating higher depression severity.
(5)Depressive symptoms at month 6 and month 12 as a binary measure, defined as PHQ-9 total score ≥ 10.
(6)Anxiety symptoms at month 6 and month 12 measured using the total score of the General Anxiety Disorder-7 questionnaire (GAD-7) [38]. GAD-7 is comprised of seven questions covering anxiety symptoms in the past 2 weeks, each with a 4-point Likert scale response (0 = not all to 3 = nearly every day). The total score ranges from 0 to 21 with a higher score indicating higher anxiety severity.
(7)Anxiety symptoms at month 6 and month 12 as a binary measure, defined as GAD-7 total score ≥ 10
(8)Plasma HIV viral load (VL) suppression as a binary measure, defined as all VL measures ≤ 40 copies/mL from baseline to month 12.
(9)Self-stigma at month 6 and month 12, measured using three questions from the relevant section of the Positive Voices questionnaire [39] that concern being ashamed about HIV status; having poor self-esteem because of HIV status; finding it difficult to tell people about HIV status. Each question has a 4-point Likert scale response (strongly disagree to strongly agree). Each question will be considered separately, with strong agreement or agreement classified as positive for self-stigma. Experienced and anticipated stigma because of HIV (from family, friends, in healthcare settings) in the last three months, measured at month 6 and month 12, using five questions from the relevant section of the Positive Voices questionnaire; each question will be considered separately
(10)Social support at month 6 and month 12, measured using the mean score from a modified version of the Duke-UNC Functional Social Support Questionnaire (FSSQ) [40]. The modified FFSQ is comprised of six questions about aspects of social support received, each with a 5-point Likert response (1 = much less than I would like to 5 = as much as I would like). An individual’s mean score across the six questions will be used, and will range from 1 to 5 with a higher score indicating greater perceived social support.
(11)Resilience at month 6 and month 12, measured using the total score of the Resilience Scale (RS14) [41]. RS14 is comprised of 14 statements, each with a 7-point Likert scale response (1 = strongly disagree to 7 = strongly agree). The total score ranges from 14 to 98. A higher score indicates greater levels of resilience.
(12)Current cigarette smoking status at month 6 and month 12 as a binary measure (current smoker or not).
(13)Alcohol use at month 6 and month 12 measured using the total score of the Alcohol Use Disorders Identification Test Consumption (AUDIT-C) [42]. AUDIT-C consists of three questions on frequency of drinking, typical amount consumed and frequency of heavy drinking with a standard scoring system [42]. The total score ranges from 0 to 12 (0 = no alcohol use) with a higher score indicating higher alcohol intake. Alcohol use at month 6 and month 12 will also be evaluated as a binary measure with a total AUDIT-C score of 5 or above indicating drinking that is potentially or currently harmful to health.
(14)Recreational drug use including any use of recreational drugs, polydrug use (use of ≥ 3 drugs) and chemsex (use of one or more specific recreational drugs before or during sex) in the past 3 months, will be categorised and reported at month 6 and month 12. These are measured using the relevant sections of the Positive Voices questionnaire [39].
(15)Physical activity at month 6 and month 12 measured using the second question of the General Practice Physical Activity Questionnaire (GPPAQ) [43]. which covers five activity domains. Standard scoring methods will be used to score activities into four levels: inactive, moderately inactive, moderately active and active [43]. Walking pace will be measured using the third question of the GPPAQ which is categorised as slow pace, steady average pace, brisk pace, and fast pace [43].
(16)Coping self-efficacy at month 6 and month 12, measured using (i) the total score from the 13 items of the shortened version of the Coping Self-Efficacy Scale (CSES) [44] and (ii) the total score from 16 items of the CSES (the shortened version plus 3 additional items) [44]. Each CSES item has an 11-point Likert scale response (0 = cannot do at all to 10 = certain can do). Measures (i) and (ii) above range from 0 to 130 and 0 to 160 respectively, with a higher score indicating a higher level of coping self-efficacy.
Cost effectiveness (17)Health-related quality of life measured at 6 and 12 months captured using the generic EuroQol five dimension five level (EQ-5D-5L) score [45], which facilitates the calculation of quality adjusted life-years (QALYs) for both the within-trial and model extrapolated analysis.
(18)Health care, social care and welfare utilisation (self-reported) measured at 6 and 12 months captured using a modified Client Services Receipt Inventory [46] designed specifically for this study to complement the intervention costing that will be conducted within the trial period.
Eligibility criteriaTo be eligible to participate in either the RCT or observational cohort study, participants must be:
Adults living with HIV (aged 18 +)
Attending a specialist HIV clinic in England
Able to provide informed consent to participate, willing and able to participate
Available for the duration of follow-up in the study.
Sufficient level of English to take part.
Participants will not be eligible for the RCT if they:
Have an active serious mental health condition (including psychosis, bipolar disorder, or active suicidality) determined by the staff member obtaining consent in consultation with the site Principal Investigator
Are within the first 12 weeks of receiving a new psychotherapy intervention.
Potential participants will complete an eligibility screening survey [the HIV Positive Outcomes (PO-11) [33] either online or on paper. To be randomised to the RCT, participants must have a PO-11 score ≥ 16, indicating poorer psychosocial health and well-being. If they score < 16, they will be invited to enrol in the observational arm of the study. Screening logs will be used to calculate response rates including eligibility, numbers excluded and reasons for exclusion.
Setting and recruitmentThe study will take place across seven HIV outpatient clinics in England: London (three clinics), Brighton, Bristol, Manchester and Sheffield. A full list of participating clinics can be found on the trial registration website [47]. We determined that a secondary-care intervention based in HIV services would have the greatest potential for success. People
Comments (0)