This study aimed to determine the prevalence rates of eating disorder risk and low energy availability risk in collegiate athletes at a large Division 1 university in the Midwest. The prevalence rates were further evaluated by sport, sport type, and sex to evaluate how risk differs amongst these variables. This information could help build more targeted and personalized approaches to identify and improve eating behaviors and attitudes in college athletes.
Based on this study’s results, a significant number of collegiate athletes, from both sexes and all identified sports and sport types, were identified as at risk for an ED and/or LEA. More specifically, female athletes were found to be at a greater risk for ED and LEA when compared to male athletes. Aesthetic sport athletes were at the highest risk for an ED while athletes of all sport types were at high risk for LEA. In accordance with aesthetic sport athletes as a sport type having the highest ED risk, dance team and women’s gymnastics had the highest risk for ED out of the sports evaluated in this study. On the other hand, dance team was at the lowest risk for LEA, while women’s gymnastics and field hockey had the highest risk for LEA out of the female sports. For male sports, wrestling had a higher risk for an ED while men’s volleyball had a higher risk for LEA.
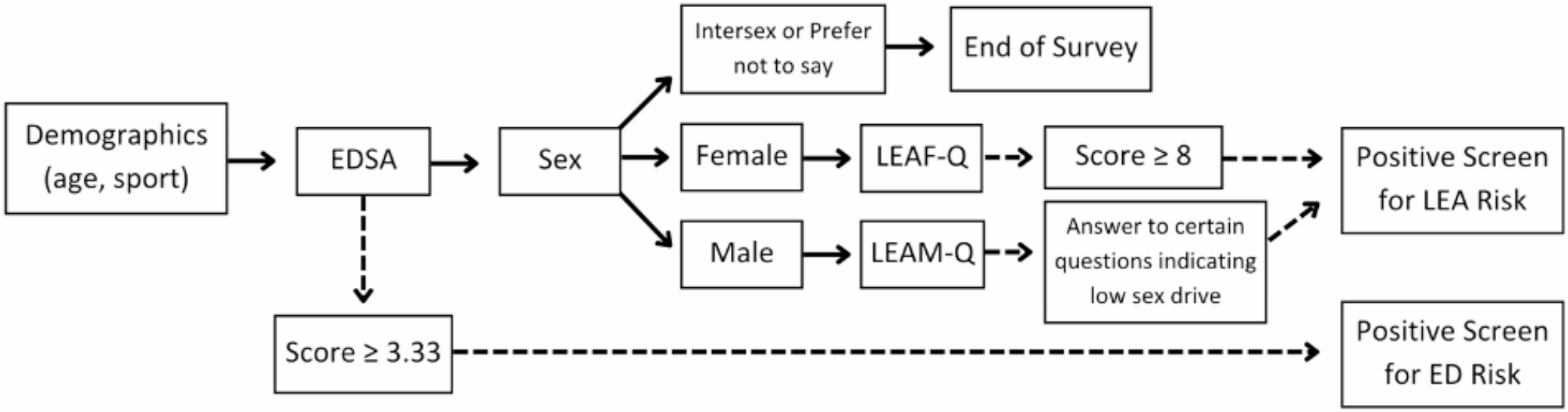
Studies conducted by Sundgot-Borgen and Torsviet [4], Thiemann et al. [10], and DiPasquale and Petrie [26] reported ED risk prevalence rates of 8–15%, although the prevalence of ED risk found in this study (38.18%) adds a higher prevalence rate to the literature. Previous research has determined that female athletes tend to be at a greater risk for an ED [3]. The present study adds to this consensus in the literature, as over twice as many female athletes screened positive for ED risk. However, this comparison does not discount the finding that almost a quarter of male athletes surveyed did screen positive for ED risk. The validation study of the EDSA reported average scores of 3.29 and 2.86 in female and male athletes in their sample [16], which is similar to the average scores on the EDSA in the present study with female athletes in the present study also averaging close to the positive screen cut-off score of 3.33.
Most LEA risk prevalence studies report rates of over 50% in female athletes [20,21,22], to which the prevalence rate of 62.86% found in this study aligns. Torres-McGhee et al. [20] and Sharps et al. [21] found a higher prevalence of LEA risk than ED risk in female athletes, a pattern to which the current study adds evidence. Limited LEA research exists in male athletes, although one study that has previously been conducted in male athletes found an LEA prevalence of 16.67% (23). This study adds to the evidence that male athletes do suffer from LEA, though potentially at a higher rate than previously reported. Currently, little research exists comparing the prevalence of LEA risk between male and female athletes within the same population, a novel aspect of the current study. While females had a significantly higher prevalence of LEA risk than males, this research provides evidence that LEA still affects male athletes and, in turn, male athletes can develop REDs from a prolonged energy imbalance.
Other studies have reported that aesthetic sport athletes have a significantly higher prevalence of ED risk and diagnosis than other sport types [4, 10, 11, 15, 27]. It is proposed that emphasis on leanness, revealing sport uniforms, early age of sport specialization, and the role appearance plays on judgment of performance are all sport-specific risk factors for eating disorders in aesthetic sports [10, 28]. While individual pairings of sport types were not assessed for significant differences, ED risk prevalence was significantly different by sport type, and the prevalence of ED risk in aesthetic sport athletes was greater than the prevalence in the other two sport types by over 20%.
LEA risk did not significantly differ by sport type. Over half of the athletes in all three sport types were at risk for LEA, and the average LEAF-Q scores for aesthetic, endurance, and ball sport athletes were all above the positive cut-off score of 8, with endurance sport athletes having the highest average LEAF-Q score (9.44 ± 4.07). The validation study of the LEAF-Q found a 62.22% prevalence of LEA risk in endurance athletes—which closely matches the result in this study (59.09%)—but no research has evaluated LEA risk in female athletes from other sport types or in male athletes by sport type [22].
Previous studies have also identified a high prevalence of ED risk in dance team and women’s gymnastics while findings are mixed amongst ball sport athletes [17, 20, 29]. Similarly, the current study adds evidence to a high prevalence of ED risk in dance team and women’s gymnastics athletes as these two sports had the two highest ED risk prevalence rates by sport, while some ball sports in the present study had high prevalence of ED risk (50% or greater) and other ball sports had a lower prevalence of ED risk (less than 25%). In contrast, little research exists evaluating ED risk by sport in male athletes and none exists regarding LEA risk by sport in male athletes. A previous meta-analysis found disordered eating to be a prevalent issue in male wrestlers, a conclusion to which the present study can add as almost half of the surveyed wrestlers screened positive for ED risk [30].
Most subgroups identified in this study had a higher proportion of athletes at risk for LEA than for an ED with male, aesthetic sport, dance team, and wrestling athletes the only subgroups that had a higher prevalence of ED risk than LEA risk. Evaluation of LEA in male athletes is still in its infancy, so it is unknown whether male athletes truly had a lower prevalence of LEA risk, or if the measurement of LEA risk in male athletes is less robust than the measurement of ED risk. The two risk proportions were similar in aesthetic sport athletes, and 40.54% of these athletes screened positive on both questionnaires (the highest proportion of any sport type), pointing to a potential association between the two conditions in this group. Overall, higher proportions of LEA risk in most sports could indicate that athletes across many sports have high training demands that could lead to an energy imbalance with or without an ED. While the other sports category was not analyzed due to its heterogeneity, it is important to note that athletes from a variety of sports can be at risk for an ED and LEA.
Several of the limitations in this study were related to the screening tools used in data collection. Screening tools are intended for use in larger populations to identify individuals for closer monitoring and follow up, but errors are inherently part of the process. The LEAM-Q, while validated, is a relatively new screening tool with limited use, and factors such as length, question content, and scoring criteria may have affected athlete answers and screening outcomes [5, 23, 25]. The current conceptual models for LEA and REDs focus on sex hormones and reproductive system responses to LEA [5, 22, 23]. However, other systems are affected by LEA. Typical LEA signs and symptoms often have other possible etiologies—such as polycystic ovary syndrome (PCOS) leading to menstrual dysfunction in women or exercise hypogonadal male condition (EHMC) leading to low testosterone in male athletes—which can often not be evaluated from screening tools alone [5, 22, 23, 31]. Additionally, athletes were routed to an LEA questionnaire based on their sex assigned at birth response, but situations in which an athlete may not fall into the typical gender and sex assigned at birth societal norms present further evidence to the limitations of the LEA screening tools and the sex hormone focus linked to LEA [5, 22, 23, 25]. Other limitations to data analysis include the number of athletes who answered per team—which affected the proportions of positive and negative screens—and the time of year in which the screening was administered—which affected the training demands an athlete currently faced.
There are several opportunities for further research related to both the screening tools themselves and practical application of these findings within athletic departments. For example, future studies should expand the sports included to capture this data across a breadth of athletic teams. Data can be collected for all teams during the same season of training or collected throughout the year to assess any data trends with changes in training seasons. Researchers should consider administering screening measures for these conditions during a dedicated time, such as with yearly physicals or scheduled medical assessments, to improve compliance and reduce needed time outside of these dedicated and medically focused events. Different ED and LEA screening tools can be used within the same population, and results of risk prevalence can be compared among the various screening tools. Additionally, screening results can be compared to physiological markers of LEA, such as bone density measured by dual x-ray absorptiometry (DXA). Researchers should also explore standardized implementation of screening protocols that are both assessable and manageable in collegiate settings as an intervention to evaluate how protocols may affect detection of ED and LEA in athletes.
Screening for ED and LEA can help sports dietitians and other members of the performance paradigm detect athletes at risk for these conditions to receive further evaluation and, if needed, treatment to improve overall health and athletic performance. It is important that athletes and athlete support staff are aware of the signs, symptoms, and impact of ED and LEA. Improved education and scalable detection methods can be used by healthcare professionals and athletic support staff to increase early recognition and treatment of ED and LEA, leading to improved outcomes [3, 5, 6, 24].

Comments (0)