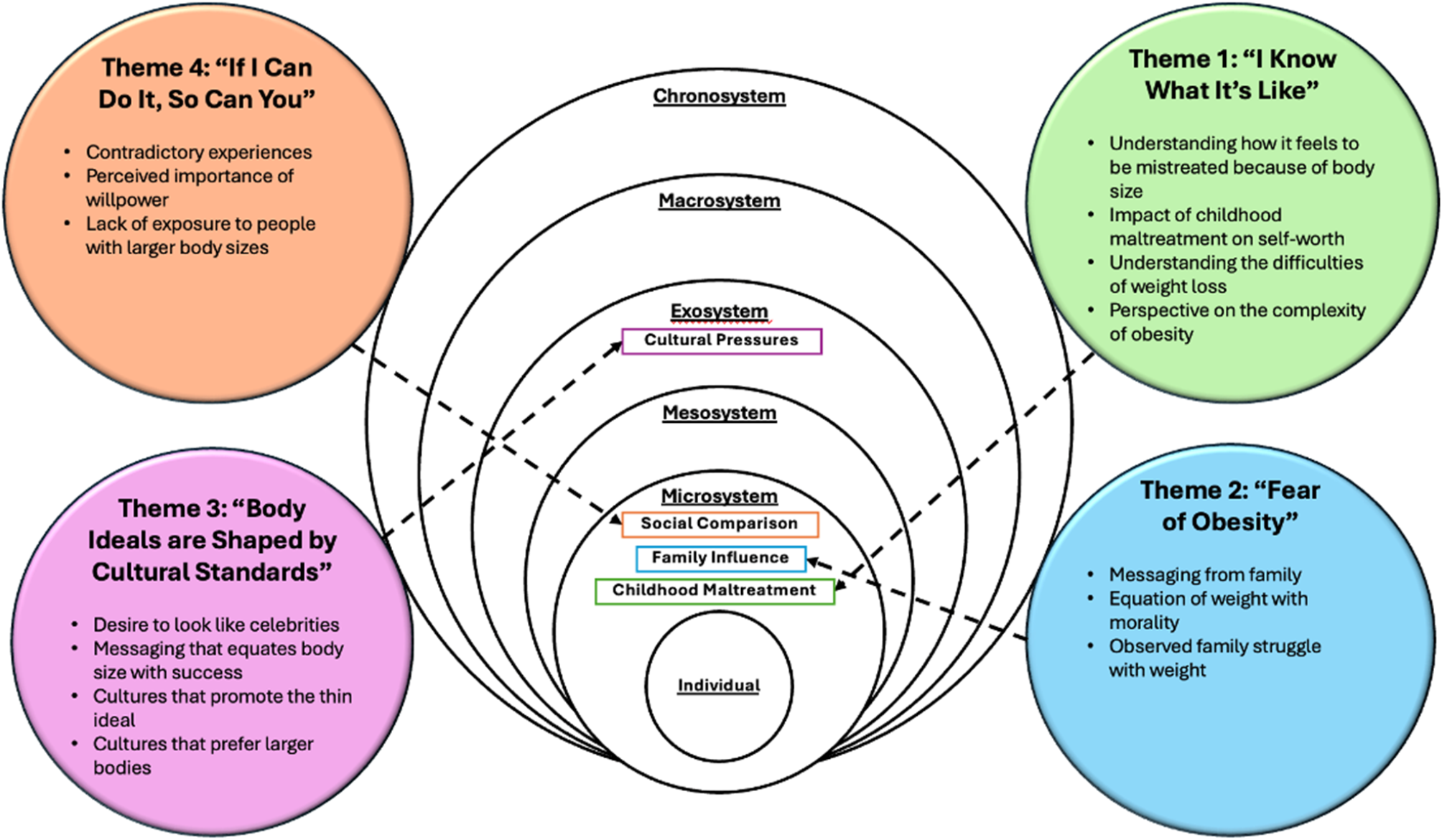
To our knowledge, this is the first study to explore medical student’s reflections on formative experiences of weight bias and their influence on their own current attitudes and beliefs about obesity. From the data, four important themes emerged. In the first theme, participants reported empathy towards individuals with larger bodies based on their own weight-stigmatizing experiences (I know what it is like). The second theme centered on participant’s perceived consequences of living with a larger body and how these shaped their beliefs about themselves and their worth (fear of having obesity). The third theme revealed medical students’ acknowledgment of the pervasiveness of weight bias from media and cultural ideals, including the inability to achieve societal body standards (body ideals are shaped by cultural standards). Last, the fourth theme focused on beliefs of personal responsibility for overcoming obesity (If I can do it, so can you).
Weight-related teasing is, by far, the most common form of bullying among children [38, 39], and such experiences were reflected in several quotes from the medical students. Weight stigmatization and more serious forms of discrimination can be formative and traumatic, contributing to the beliefs participants hold about themselves and their patients. Whether experienced directly, through bullying, or indirectly through social media, negative messages about body size and weight become ingrained and self-directed which is also known as internalized weight bias. Internalized weight bias is the process of applying negative weight-related beliefs to one’s sense of worth and has consistently been shown to be detrimental to physical and mental health independent of body weight [8, 40].
In some responses, the role of personal responsibility, including dietary and physical changes, was greatly emphasized, with little to no acknowledgment of factors such as genetic contributions, biological mechanisms that encourage weight regain, or the sociocultural environment. These findings are consistent with previous literature, such that providers with limited knowledge about the complexities and biological underpinnings of obesity generally tend to have fewer positive attitudes about patients with obesity [41]. Several medical students discussed the role of television, magazines, and social media in contributing to unrealistic appearance ideals and the negative characterization of people with obesity. Participants also discussed the difficulty of navigating Westernized appearance values in contrast to appearance expectations from their country of origin. The role of media, particularly social media, is likely to grow, indicating that media literacy, including how social media promotes weight bias, is crucial for trainee critical thinking and development.
Implications for education and training
Themes generated indicate that the subset of medical students in this study were generally aware of their weight bias and carrying varying degrees of traumatic stress from weight-related experiences. Reflecting on one’s own lived experiences may help to increase empathy and understanding of a patient’s lived experiences. Taking that into consideration, it is important for schools to recognize that medical students come with their own formative experiences, many of which have caused significant pain, which likely impact their own confidence, sense of worth, and their receptivity to overt and hidden curriculum messages. Drawing on early lived experiences can help medical students cultivate compassion for themselves and others through remembering their own vulnerabilities and emotional experiences surrounding weight bias. Such experiences also help us understand that weight bias is socially constructed, and by creating shifts in our social environment, such as medical training settings, new learning can occur, and biases can be shifted. Reflecting on these experiences and beliefs also has the potential to improve patient care, especially in pediatric and young adult populations. By providing a safe space to discuss weight bias and focus on patients’ needs, medical students as future healthcare providers can make more equitable and compassionate treatment decisions [27].
A trauma-informed care approach [42], which is important for practicing physicians to use with their patients, may also be useful in educating students about obesity and weight bias. This approach positions faculty and educators to recognize that individuals may likely have their own experiences of trauma and uses strategies like creating space for students to share their perspectives free of judgment and creating opportunities for peer support when exploring issues related to obesity-related conditions, obesity pathophysiology, obesity care, and weight bias. Medical students will likely benefit from personal reflections or open dialogues about the role of formative experiences contributing to their current attitudes and beliefs about obesity. Self-reflection in medical training, in addition to other interventions, is common and effective for reducing stigma in other areas, including anti-racism [43] and substance misuse [44]. Strategies to reduce weight bias should also provide education about the complex, multifaceted etiology of obesity, encouraging students to place less blame on the individual for not achieving a lower weight on their own and focusing on how students can advocate for policy, environmental, and global changes that can promote novel therapeutic interventions and equitable access to resources to encourage sustainable healthy behaviors.
Furthermore, the use of narrative approaches in medical training can help to increase compassion, empathy, and a willingness to hear patient’s stories. Through reflection of their formative experiences of weight bias, medical students may be able to connect more closely with their patients’ narratives, and resonate with their patient’s lived experiences. Narrative approaches focus on patient storytelling, active listening, and challenging assumptions about the “causes” of illness, such as the recognition of the role weight bias plays on exacerbating obesity [45, 46]. Importantly, such approaches must also be actively role-modeled by clinicians and supervisors in the field, as medical students are susceptible to repeating the behaviors they observe from their superiors. Similarly, teaching and role modeling person-first language can reduce stigmatizing language, which has been implemented in several other areas of medicine [47, 48]. Saying “patient with obesity” as opposed to “obese patient,” respects the person independent of their condition. Providers should also consider patients’ preferred terms for discussing body weight, as “obesity” is a clinical term and generally not preferred from a patient point of view [49, 50]. Lastly, role-playing among students of hypothetical scenarios in direct patient care offers opportunities to practice these skills [51].
Importantly, strategies to reduce weight bias can only be successful if medical schools also explicitly address the competing tensions that exist within medical training. For example, students with lived experiences of weight bias are also receiving subtle messaging that providers should role model a “healthy” (i.e., thin) body size [52]. Similarly, medical schools project a focus on student well-being, yet aspects of medical training (e.g., lack of quantity/quality sleep, increased stress/anxiety, long work hours) promote impaired metabolic health and increase risk for rapid weight gain [53]. In addition, classroom lectures and clinical experience often hyperfocus on the “othering” of individuals with obesity, because of associated disease risk reflected in the literature. Students might be encouraged to engage in reflection and other activities to reduce weight bias, yet they also might observe their superiors stigmatize patients and fail to acknowledge the complexity of obesity [54]. These competing tensions leave students dealing with a double-standard that may feel difficult to navigate. Strategies to reduce this tension might include implementing policies that prohibit derogatory language about patients with obesity and providing peer support groups for students [52].
Strengths and limitations
This research study’s strengths include a large sample size of medical students, which allowed for an expansive evaluation of formative experiences of weight bias, current obesity-related beliefs, and potential implications for their work with all patients and particularly those with obesity. Furthermore, this study provided a unique opportunity to better understand the harmful experiences and pain medical students and likely many practicing clinicians carry, including internalized weight bias, some of which enhanced their own empathy towards individuals with overweight and obesity, yet was clearly still painful for many students. These findings provide a strong foundation for future research and medical training curriculum development. Limitations of the study include that only a small portion of participants described formative experiences (N = 212/716, 29.6%), and the use of only one writing prompt. It is likely that our sample does not represent the full pool of people for whom childhood experiences have influenced their attitudes about body size. Moreover, our prompt question did not specifically seek information about formative experiences, and it is possible our sample reflects a highly specific group of individuals that were particularly sensitive to this topic. Future research should explore the use of other qualitative research methods, including interviews and focus groups, to achieve a more comprehensive understanding of students’ formative experiences and internalized weight bias. It would also be helpful to gather more information about how students perceive these formative experiences as influencing their current work in healthcare. In addition, this analysis was focused on a group of medical students who took the IAT for weight bias and whose responses were selected for analysis because they contained reference to formative experiences. Students likely perceived the importance of being aware of weight bias through their engagement in this IAT exercise, which, in partnership with social desirability bias, might have created pressure for students to write what they believed faculty would perceive more favorably as opposed to their more genuine thoughts. The generalizability of findings from this cohort to other medical students, trainees, and practicing clinicians is important to explore in future research.

Comments (0)