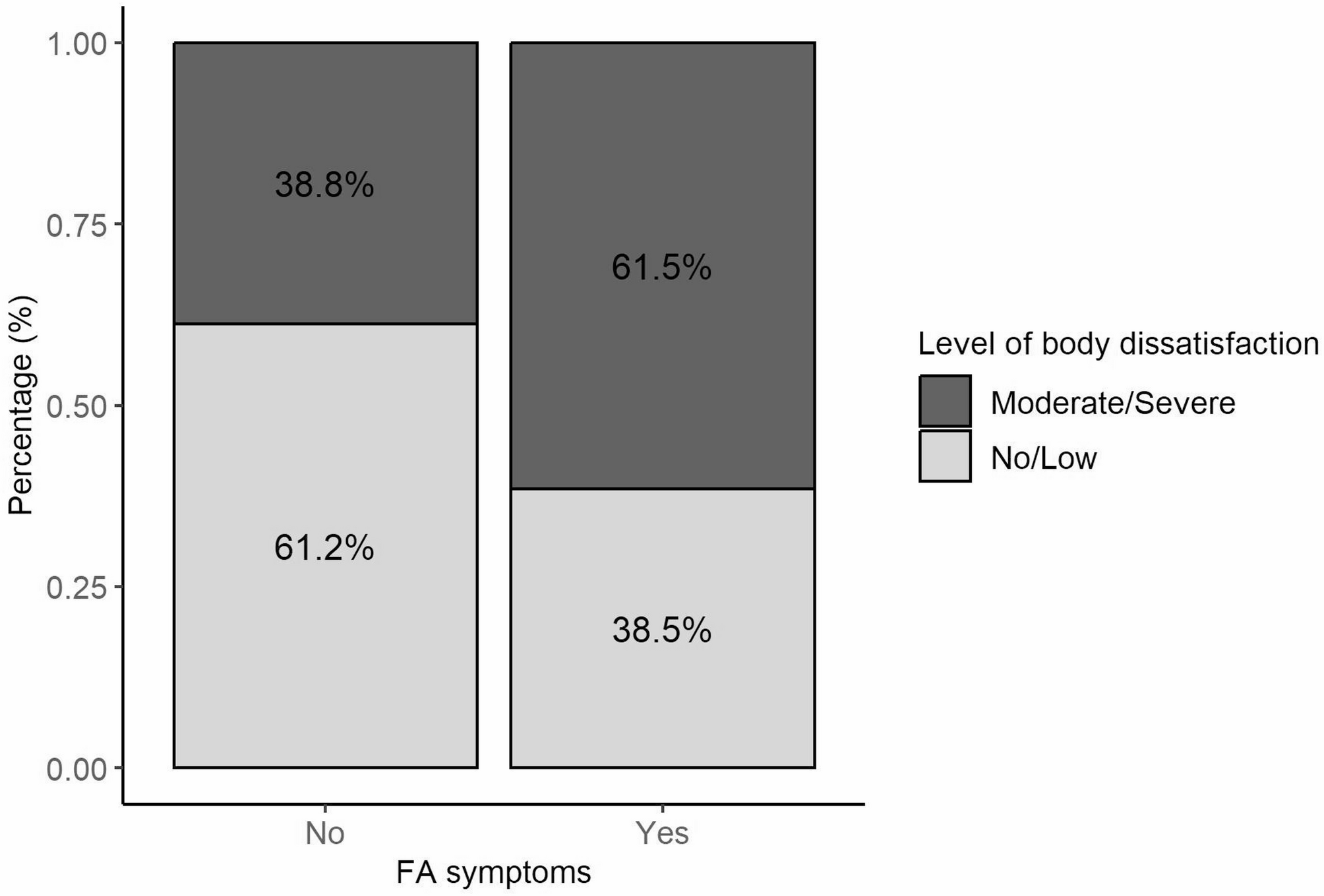
The present study explored the relationship between FA symptoms and body dissatisfaction in individuals seeking bariatric surgery, with a particular focus on the frequent occurrence of FA symptoms in those with obesity. Previous research suggests that the increased consumption of hyperpalatable foods is linked to the presence of FA [15, 29]. However, to the best of our knowledge, no prior studies have identified a direct association between FA and body dissatisfaction. The key finding of this study was the evidence that body dissatisfaction is associated with the presence of FA symptoms in the studied population.
Food addiction is part of a broader pathological framework where the neurobiology of eating disorders reveals an eating behavior phenotype similar to substance dependence, distinguishing it from other disorders in the eating disorder spectrum, such as Binge Eating Disorder and Bulimia Nervosa [21, 22]. While there does not seem to be a direct link between body weight and food addiction (FA), weight stigma plays a critical role in understanding this condition. Individuals with severe obesity, along with the stigma surrounding the condition, often experience higher rates of FA. Greenberg et al. (2021) examined how internalized stigma can lead to social isolation and increased compulsive food consumption as a way of coping with emotional distress [30]. Similarly, Koehler et al. (2021) found that weight stigma contributes to the continuation of disordered eating behaviors, negatively impacting psychological well-being and the success of bariatric interventions [31]. In Bianciardi’s (2019) study, the primary predictors of body image dissatisfaction included binge eating, depression severity, female sex, and insecure attachment traits, highlighting the importance of mood assessments and evaluations of psychological and psychiatric symptoms [32].
Based on mYFAS 2.0 assessments, 21% of participants of this study exhibited symptoms of food addiction. It is believed that one of the reasons for seeking surgery is the difficulty in controlling eating behaviors to manage body weight. A systematic review and meta-analysis of 40 studies found a prevalence of FA in 32% of patients during the preoperative period (95% CI: 27–37%) [22]. Additionally, Koball (2021), in an analysis of 1,006 patients undergoing pre-surgical psychological evaluations, reported a prevalence of 18%, with 56% of these individuals exhibiting severe FA symptoms [5].
On the other hand, Lipsky et al. (2024) reported a prevalence of FA symptoms in 4.7% of young adults, with 91% of cases occurring in women, and found no correlation with other sociodemographic factors [33]. It is important to note that the predominance of female participants may limit the generalizability of these results to both sexes. Consistent with this finding, the demand for bariatric surgery remains higher among women, as observed in the present study.
Current scientific evidence suggests that women with obesity are more prone to social isolation, disordered eating behaviors, and body image dissatisfaction, which serve as major motivators for seeking surgical treatment. This supports the hypothesis that men experience less societal pressure related to body aesthetics, resulting in lower levels of body dissatisfaction [34, 35]. In a cross-sectional study by Bianciardi (2019), which included 536 pre-bariatric surgery patients (70.7% women) with an average age of 43.88 years and a mean BMI of 42.98 kg/m², 60% of participants reported moderate or severe body dissatisfaction [32]. Similarly, the study by Bosc et al. (2022), which assessed 61 patients before and five years after bariatric surgery, found significant improvements in body image satisfaction and self-confidence within 12–18 months postoperatively. However, these effects were not sustained over the full five years following surgery [36].
Although a correlation between BMI and FA is expected in the population with obesity, due to FA’s impact on eating behavior and body weight, there is still limited research to fully explore this relationship. In the Brazilian cross-sectional study by Lima et al. (2024), which followed 303 participants across all BMI levels for 21 months (mean age 37.03 years, 84.16% women), FA symptoms were identified in 40.26% of participants (n = 122), with a significant but weak positive association between FA and BMI [20]. Similarly, the Spanish cross-sectional study by Escrivá-Martinez et al. (2023), which included 400 university students (51% women, mean age 23.35 years, mean BMI 21.90 kg/m²), found a prevalence of 31.9% of FA symptoms but did not observe a positive association between BMI and FA, which aligns with our findings [37].
Other studies suggest that psychiatric distress and body image dissatisfaction may be worsened by FA, creating a vicious cycle of binge eating, guilt, and shame that begins in the preoperative period. Cassin et al. (2021), evaluated post-operative bariatric surgery patients and found that those with FA reported greater binge eating characteristics and psychiatric distress relative to those without FA symptoms [38]. Recently, Kalan et al. (2024) further support this connection, noting that body image dissatisfaction is directly linked to the worsening of psychiatric symptoms in adults with FA [39].Lacroix et al. (2019), in their study on how Brazilian adults define and experience “addictive eating,” highlight the interrelation between FA and body image disturbances. Their findings suggest that body image distress accounts for more variance in psychosocial impairment related to eating than YFAS scores alone. These results underscore the importance of addressing potential body image disturbances in interventions aimed at treating FA [40].
It is also important to consider the impact of FA on body weight regain after bariatric surgery. A study conducted in Texas with 294 patients found that the rates of severe, moderate, and mild FA were 12.55%, 7.36%, and 7.36%, respectively. However, with no significant association between FA and postoperative body weight regain [41]. Similarly, Walø-Syversen et al. (2024) studied 69 bariatric surgery candidates and found that 16% met the diagnostic criteria for FA. While FA was associated with problematic eating behaviors and depression, it did not affect post-surgical weight loss [42]. These findings highlight the complexity of FA and its relationship with psychological factors, emphasizing the need for multidimensional approaches in obesity management and the evaluation of bariatric surgery candidates.
Notably, body image refers to how individuals perceive, feel about, and behave toward their own bodies. The findings of this study highlight the importance of understanding the factors associated with body satisfaction and its connection to disordered eating behaviors. In the context of bariatric surgery, this understanding is crucial for enhancing quality of life and fostering improved body satisfaction following surgery.
This investigation did not address intervention strategies, there is a growing need to examine how body image interventions should be tailored for individuals exhibiting symptoms of food addiction. Traditional body image treatments for eating disorders typically emphasize food positivity, body acceptance, and moderation. However, body image interventions for individuals with food addiction should not simply follow the traditional approaches used for eating disorders without adaptation. While body image disturbance is a significant contributor to psychosocial impairment in food addiction and warrants targeted intervention, food addiction and eating disorders, though overlapping, have distinct clinical features and underlying mechanisms. In this way, it may be required to address specific features such as compulsive eating, craving intensity, and emotion-driven consumption. In addition, protocols should be adapted rather than directly adopted from existing eating disorder guidelines, with an emphasis on individualized, multidisciplinary care, especially in populations with severe obesity preparing for bariatric surgery [40].
Therefore, the importance of interdisciplinary follow-up both before and after bariatric surgery is emphasized. Such support can help prevent and manage mental health issues, given the strong connection between body dissatisfaction, anxiety, depression, and other psychological disorders [2, 43].
This study utilized the YFAS 2.0, a validated instrument available in multiple languages, which is widely recognized as a valuable tool for assessing food addiction in Brazilian bariatric surgery candidates and individuals with a BMI ≥ 30 kg/m [44]. In Brazil, the short version of the YFAS 2.0 (mYFAS 2.0) has demonstrated high reliability (α = 0.915) in clinical samples with depressive disorders, suggesting its potential as a brief and effective screening tool for FA in this population [20]. However, as a self-report instrument, it is not intended to serve as a diagnostic tool, as it does not include a clinician-led assessment.
Although this study did not explore intervention strategies, we recognize the growing need to investigate how body image interventions should be approached in individuals exhibiting food addiction symptoms. Traditional body image treatments for eating disorders often emphasize food positivity, body acceptance, and moderation. However, it is still unclear whether these approaches are equally effective or appropriate for individuals with food addiction, particularly given the compulsive, craving-driven nature of the behavior [40].
If food addiction becomes recognized as a distinct eating disorder in the future, it may be appropriate to integrate existing evidence-based interventions that address body image and the internalization of weight stigma. Conversely, if it remains outside the formal diagnostic framework, it may require the development of adapted or novel approaches that target not only body image disturbance but also the addictive-like eating patterns. More research is needed to clarify whether these interventions should converge with or diverge from traditional eating disorder treatments, especially in populations with severe obesity preparing for bariatric surgery [40].

Comments (0)